1 EXECUTIVE RESPONSIBLE Adam Cairns Chief Executive AUTHOR (if different from above) Paul Hodson...
12
1 EXECUTIVE RESPONSIBLE Adam Cairns Chief Executive AUTHOR (if different from above) Paul Hodson Head of Contracts & Performance Pete Gordon Head of Continuous Improvement William Wraith Head of Human Resources Tony Brown Assistant Director Financial Performance CORPORATE OBJECTIVE Enhancing Patient Experience, Safety and Effectiveness, Achieving NHS Foundation Trust Status BUSINESS PLAN OBJECTIVE NO(S) 6.1 - Establish a new Quality Framework for the Trust. 6.1.1 - Develop an integrated performance management framework that includes a balanced set of quality metrics across the domains of safety, effectiveness and patient experience. EXECUTIVE SUMMARY This paper reports current performance against a number of KPIs for the period up to the end of October 2010. As detailed in previous papers this reports only includes slides for those KPIs identified as suitable for monthly reporting. The summary sheet will continue to show a RAG for all KPIs with quarterly KPIs showing their RAG status at the end of the KEY FACTS • Daycase rate decreased in October. • Elective length of stay decreased at RSH and increased at PRH. • Non elective length of stay decreased at RSH and increased at PRH. • The number of staff employed was 4,231 WTE at the end of October. • Validated sickness absence rate for July was 4.5%. RECOMMENDATION S The Board is asked to NOTE: • performance against a range of Key Performance Indicators covering Quality, Delivery and Foundations. INTEGRATED PERFORMANCE REPORT for period ending 31 st October 2010 Trust Board – 3 December 2010 Enclosure 5
-
Upload
lynn-anthony -
Category
Documents
-
view
213 -
download
0
Transcript of 1 EXECUTIVE RESPONSIBLE Adam Cairns Chief Executive AUTHOR (if different from above) Paul Hodson...

1
EXECUTIVE RESPONSIBLE
Adam CairnsChief Executive
AUTHOR (if different from above)
Paul HodsonHead of Contracts & Performance
Pete GordonHead of Continuous Improvement
William WraithHead of Human Resources
Tony BrownAssistant Director Financial Performance
CORPORATE OBJECTIVE
Enhancing Patient Experience, Safety and Effectiveness,Achieving NHS Foundation Trust Status
BUSINESS PLAN OBJECTIVE NO(S)
6.1 - Establish a new Quality Framework for the Trust.6.1.1 - Develop an integrated performance management framework that includes a balanced set of quality metrics across the domains of safety, effectiveness and patient experience.
EXECUTIVE SUMMARY
This paper reports current performance against a number of KPIs for the period up to the end of October 2010. As detailed in previous papers this reports only includes slides for those KPIs identified as suitable for monthly reporting. The summary sheet will continue to show a RAG for all KPIs with quarterly KPIs showing their RAG status at the end of the last full quarter.
KEY FACTS • Daycase rate decreased in October.
• Elective length of stay decreased at RSH and increased at PRH.
• Non elective length of stay decreased at RSH and increased at PRH.
• The number of staff employed was 4,231 WTE at the end of October.
• Validated sickness absence rate for July was 4.5%.
RECOMMENDATIONS The Board is asked to NOTE:• performance against a range of Key Performance
Indicators covering Quality, Delivery and Foundations.
INTEGRATED PERFORMANCE REPORT for period ending 31st October 2010 Trust Board – 3 December 2010
Enclosure 5

2
Integrated Performance Report:Delivery (CO2, CO3 & CO4) Foundations (CO5 & CO6)
Target (2010/11)
Executive Lead
Monthly Performance
Direction of Travel
Year to Date Forecast Commentary Frequency
Increasing productivity and encouraging innovation
Theatre Utilisation % Utilisation of funded theatre sessions DoS AMBER = AMBER GREENOverall theatre performance remains constant but revised action plan
should improve performance M
Length of Stay (LOS)
Elective - To achieve upper 20th percentile performance within five years from 2009 DoS GREEN AMBER GREEN
Increase at PRH of 0.2 daysand a decrease at RSH of 0.4 days M
Reduce total number of surgical pre-operative bed days per month DoS GREEN = GREEN GREENDecrease of 28 bed days at PRH and a decrease of 20 bed days at
RSH M
Non Elective - To achieve upper 20th percentile performance within five years from 2009 DoS AMBER = AMBER AMBER Increased by 0.3 days at PRH and decreased by 0.1 days at RSH M
Daycases Maintain a daycase rate above 78% DoS AMBER GREEN GREEN Decreased to 76.5% during October M
Outpatient Utilisation
% of patients booked in the capacity available (CO2.4) FD AMBER = AMBER AMBEROverall DNA rate in October was 6.3% Ophthalmology and T&O
remain higher than the Trust average M
Supporting and developing our workforce in a learning
organisation
Workforce Numbers
All staff Whole Time Equivalent (WTE) employed on permanent & fixed contracts DCA RED = RED GREEN
Recruitment of Junior Medical Staff far more successful this year which should reduce Locum costs M
Sickness % Sickness Absence and WTE Days Lost DCA GREEN = GREEN GREEN Validated absence level 0.2% lower than this month last year M
Ensuring a clinically viable & financially sustainable
organisation
Financial Risk Rating
Maintain Monitor Governance Risk Rating at Amber or above FD RED = RED Risk Score below target M
Governance Risk Rating
Assess performance against Monitor Governance Risk DSD RED AMBER GREEN Monitor Governance Risk Rating of Red Q
Achieving N
HS Foundation Trust status
Foundation Trust Status
To achieve NHS Foundation Trust status in 2011 DoS RED = RED AMBERDetails for organisational transition continue to emerge in November.
A revised trajectory for the Trust’s FT application must be agreed with the SHA and informed to the DH during November 2010
M

3
Theatre Utilisation
Target (2010/11) Executive Lead
Monthly
StatusDirection of
TravelYear to
DateForecast Commentary
Theatre Utilisation% Utilisation of funded theatre sessions. DoS AMBER = AMBER GREEN
Overall theatre performance remains constant but revised action plan should
improve performance
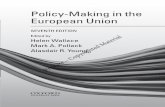
Theatre Utilisation: Theatre Utilisation for PRH in October is 81% and RSH 75% which is a 2% increase at
PRH and a reduction of 4% at RSH compared to the previous month. The key reasons for under utilisation resulting in lost activity at RSH are: - Fixed emergency/trauma sessions 5% - Closed sessions 8% - Unused Theatre time 12% - Total RSH under-utilisation 25%
- RSH lost a total of 100 theatre sessions in October.
Performance Management: Data is available for each Centre split by speciality. Speciality data can be split by Consultant. Percentage data can be converted into number of theatre sessions lost. Data can be broken down into cancelled operations and the reasons why. Data can be broken down into late starts and the reasons why. Data is available for unfunded sessions, majority funded by WLT.
Actions: • Report findings to Clinical Leads and Divisional General Managers. A fortnightly meeting has now commenced and following actions have been agreed:- Start times for theatre sessions.- The removal of fixed emergency trauma sessions from theatre utilisation.- Continue with implementation of Theatre Briefing and roll out pilot in December as part of Productive Theatre.- Paper for Management Executive in January regarding Productive Theatre.
Theatre utilisation at PRH & RSH Oct 09 - Oct 10
0%20%40%60%80%
100%
PRH 79% 57% 66% 67% 87% 82% 84% 84% 79% 76% 72% 78% 81%
RSH 79% 82% 65% 73% 74% 73% 76% 81% 77% 78% 68% 79% 75%
Target 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
Oct Nov Dec J an Feb Mar Apr May J une J uly Aug Sep Oct
Number of Theatre non attenders by three most frequent reasons between Oct 09 - Oct 10
0
50
100
150
200
250
300
Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10
DNA Not fit No Bed

4
Actions:• Continued bi-weekly meetings of the Elective Length of Stay Project Group.• Increase usage of Surgical Admission Suite at RSH. Capital work to expand the area commences 15th November with a planned completion date - 17th Dec 2010.• Covert inpatients to daycase where possible using BADS (British Association Day Surgery) criteria.• Continued implementation of the Enhanced Recovery Programme.
Elective Length of Stay (LOS)
Target (2010/11)Executive
LeadMonthly
StatusDirection of
TravelYear to
DateForecast Commentary
Length of Stay (LOS) – Elective
To achieve upper 20th percentile performance within five years from 2009
DoS GREEN AMBER GREENIncrease at PRH of 0.2 days
and a decrease at RSH of 0.4 days
• PRH Elective LOS Increased by 0.2 days between September and October.The median elective length of stay remained at 1 day during October.
• RSH Elective LOS Decreased by 0.4 days between September and October.The median length of stay reduced to 1 day during September.
PRH - Elective Length of Stay October 09 -October 10
0.0
1.0
2.0
3.0
4.0
LO
S
Mean 3.3 3.7 2.9 2.5 2.9 2.8 3.5 3.1 2.7 2.8 3.3 2.6 2.8
Mean Target 3.0 3.0 3.0 2.9 2.9 2.9 2.9 2.9 2.9 2.9 2.9 2.9 2.9
Median 2 2 1 2 1 2 1 1 1 1 1 1 1
Oct-09 Nov-09 Dec-09 J an-10 Feb-10 Mar-10 Apr-10 May-10 J un-10 J ul-10 Aug-10 Sep-10 Oct-10
RSH - Elective Length of Stay October 09 - October 10
0.0
1.0
2.0
3.0
4.0
LO
S
Mean 3.6 3.2 3.3 3.2 3.1 2.8 3.0 3.5 3.3 3.4 3.8 3.3 2.9
Mean Target 3.1 3.1 3.1 2.9 2.9 2.9 2.8 2.8 2.8 2.8 2.8 2.8 2.8
Median 2 2 2 2 2 2 2 2 2 2 2 2 1
Oct-09 Nov-09 Dec-09 J an-10 Feb-10 Mar-10 Apr-10 May-10 J un-10 J ul-10 Aug-10 Sep-10 Oct-10

5
Elective Surgical Pre Operative Bed Days per Month
Target (2010/11)Executive
LeadMonthly
StatusDirection of Travel
Year to Date
Forecast Commentary
Elective Surgical Pre Operative Length of Stay (LOS)
Reduce total number of surgical pre-operative bed days per month DoS GREEN = GREEN GREEN
Decrease of 28 bed days at PRH and a decrease of 20 bed days at RSH
• The number of elective surgical pre operative bed days decreased at PRH by 28 from September and decreased by 20 at RSH.
• The median number of pre operative bed days per month over the last 12 months at PRH is 105 and 129 at RSH.
• The Surgical Admission Suite (SAS) at RSH is currently open 4 days a week. 124 patients were admitted via the SAS in October 2010 (the highest to date). Capital work to expand the SAS & pre-operative assessment area commences 15 th November with a planned completion date 17 th December 2010. This will enable more elective surgical patients at RSH to be admitted on the day of surgery.
Actions:• Increase the number of patients being admitted via the Surgical Admission Suite.• Provision of monthly Elective Surgical Pre-operative Length of Stay information for clinical and managerial staff.• Increase day of surgery admission for elective Orthopaedic inpatients at PRH.
Elective Surgical Pre Operative Bed Days per month October 09 - October 10
20406080
100
120140160180200
Oct Nov Dec Jan Feb Mar Apr May June July Aug Sept Oct
PRH RSH

6
Target (2010/11)Executive
LeadMonthly
StatusDirection of
TravelYear to
DateForecast Commentary
Length of Stay (LOS) – Non Elective
To achieve upper 20th percentile performance within five years from 2009
DoS AMBER = AMBER AMBERIncreased by 0.3 days at PRH and
decreased by 0.1 days at RSH
• PRH Non Elective LOS
Increased by 0.3 days between September and October.The median length of stay remained constant at 2 days.
• RSH Non Elective LOS Decreased by 0.1 days between September and October.The median length of stay remained constant at 2 days.
Non Elective Length of Stay (LOS)
Actions:• Continue monthly ‘Joint Discharge Transformation Team’ meetings focussing upon significant areas of delay for patients with continuing healthcare needs.• New model of Consultant Working to commence December 2010 at RSH.• Live ‘visual’ SQL reporting for admissions, discharges and discharge lounge utilisation available via intranet to all SATH staff. • A number of QIPP schemes focussed upon improving patient flow are being introduced to ensure closer partnership working between primary & secondary care. These include 7 day working within DAART, GPs within the emergency departments and a ‘virtual ward’.• Confirm clinical lead for unscheduled care to enable improved flow management within the local health economy.• Implement patient status at a glance technology Trust wide.
PRH - Non Elective Length of Stay October 09 - October 10
0.0
2.0
4.0
6.0
8.0
LO
S
Mean 6.0 6.4 6.8 6.0 6.7 5.9 5.8 5.9 5.6 5.7 6.0 6.3
Mean Target 5.4 5.4 5.1 5.1 5.1 5.0 5.0 5.0 4.9 4.9 4.9 4.9
Median 2 2 2 2 2 2 2 2 2 2 2 2
Nov-09 Dec-09 J an-10 Feb-10 Mar-10 Apr-10 May-10 J un-10 J ul-10 Aug-10 Sep-10 Oct-10
RSH - Non Elective Length of Stay October 09 - October10
0.0
2.0
4.0
6.0
8.0
LO
S
Mean 4.28 5.7 5.1 5.4 5.3 5.2 5.1 4.7 4.5 5.1 5.1 5.2 5.1
Mean Target 3.98 4.0 4.0 4.0 3.8 3.8 3.8 3.7 3.7 3.7 3.6 3.6 3.6
Actual 2 2 2 2 2 2 2 2 2 2 2 2 2
Sep-09 Oct-09 Nov-09 Dec-09 J an-10 Feb-10 Mar-10 Apr-10 May-10 J un-10 J ul-10 Aug-10 Sep-10

7
Daycases
Target (2010/11)Executive
LeadMonthly
StatusDirection of
TravelYear to
DateForecast Commentary
Daycases Maintain a daycase rate above 78% DoS AMBER GREEN GREEN Decreased to 76.5% during October
• This key performance indicator measures the percentage of Daycase procedures as a total of all elective procedures.
• Daycase rate for October decreased by 2.8% to 76.5%.
Actions:• Convert inpatients to daycase where possible.• Create BADS (British Association of Day Surgery) report within MedeAnalytics for Consultants.
Day Case October 09 - October 10
70%
75%
80%
85%
Series1 80.2% 79.7% 74.7% 78.2% 77.8% 78.3% 78.4% 77.3% 79.5% 77.9% 80.9% 79.2% 76.5%
Series6 78% 78% 78% 78% 78% 78% 78% 78% 78% 78% 78% 78% 78%
Oct Nov Dec J an Feb Mar Apr May J un J ul Aug Sep Oct

8
Outpatient Utilisation
Target (2010/11)Executive
LeadMonthly
StatusDirection of
TravelYear to
DateForecast Commentary
Outpatient Utilisation% of patients booked in the capacity available (CO2.4) FD AMBER = AMBER AMBER
Overall DNA rate in October was 6.3% Ophthalmology and T&O remain
higher than the Trust average
• In October, the total OP attendances were 52,005 (19,064 new and 32,941 follow-up).
• The Scheduling Team booked an additional 33 OP clinics in October, arranged within 3 weeks notice to meet national standards (21 at RSH and 12 at PRH). Other additional clinics booked by the SDUs are not recorded in these numbers.
• Recorded total DNA rate in October was 3,641 (6.3%), an improvement of 0.3% compared with September 2010.
• DNA rate in Ophthalmology was 9.7% for new appointments and 7.8% for follow-up and DNA rate in T&O was 6.5% for new appointments and 11.4 % for follow-up.
• Ophthalmology OP appointment letters were amended in October following feedback from patients and GPs, offering the date of appointment directly, but giving the choice to change if the appointment offered is not convenient. Appointment letters are sent 30 days prior to the appointment date.
Actions:• DNA rate for Ophthalmology will be monitored following the change to the appointment letter.• Investigation underway to add a further text reminder via SEMA.
2010/11 OP DNA rate compared with 2009/10
3.00%4.00%5.00%6.00%7.00%8.00%
Actual 5.70% 5.90% 6.10% 5.70% 5.90% 6.60% 6.30%
Profile 6.30% 6.30% 6.10% 6.30% 5.90% 6.20% 6.00% 5.90% 6.50% 7.30% 5.60% 5.90%
Apr 10 May 10 J un 10 J ul 10 Aug 10 Sep 10 Oct 10 Nov 10 Dec 10 J an 11 Feb 11 Mar 11

9
Target (2010/11)Executive
LeadMonthly
StatusDirection of Travel
Year to Date
Forecast Commentary
Workforce NumbersAll staff Whole Time Equivalent (WTE) employed on permanent & fixed contracts
DCA RED = RED GREENRecruitment of Junior Medical Staff far more successful this year which should
reduce Locum costs
Thresholds Descriptions:Green: WTE > 95.9% of establishment AND total workforce cost < budgetAmber: WTE = 93.0-95.9% of establishment AND total workforce cost < budgetRed: WTE < 93.0% of establishment AND total workforce cost > budget
• 4,231 WTE substantive staff, end of October 2010; increase of 1 since end September (ESR).
• 91.7% of monthly budgeted establishment; 93.1% YTD average of monthly budgeted establishment; YTD rating amber except for cost.
• The contracted figure is 4,245 WTE.• The budgeted establishment for October was 4,615 WTE (£14.421M). The chart
illustrates total workforce for October from all sources was 4,521 WTE (£15.138M) - met through the use of permanent staff, overtime, bank and agency staff.
• Areas of highest use of agency (by cost): Medical Staff Anaesthetics – RSH (£95,302), Medical Staff General Medicine – RSH (£45,552), Medical Staff General Medicine – PRH (£34,097), Medical Staff Ophthalmology – RSH (£29,837).
• Total Agency spend: £0.552M.• Agency use by WTE:
Workforce Numbers
Actions:• Recruitment is being closely monitored by the Executive Team.• The use of bank and agency staff is continuously reviewed on a weekly basis by the Line-Managers and the Executive Team.
Medics Nursing Other
Aug. 37 2 17
Sep. 41 3 11
Oct. 38 13 11
Workforce Numbers WTE (Whole Time Equivalent)
3650
3750
3850
3950
4050
4150
4250
4350
4450
4550
4650
WT
E
Actual Worked Agency Staff WTE 2010-11 83 68 69 70 56 55 62
Actual Bank Worked WTE 2010-11 221 183 174 193 204 214 223.1
Staff Utilised WTE 2010-11 67 19 38 37 6 2 -9
Contracted Staff WTE 2010-11 4235 4239 4237 4237 4255 4240 4245
Total Staff 2010-11 (Excluding Bank WTE) 4220 4232 4239 4229 4231 4230 4231
Total Staff 2009-10 (Excluding Bank WTE) 3898 3914 3921 3923 3950 3985 4047 4122 4120 4169 4191 4196
Total Staff 2008-09 (Excluding Bank WTE) 3796 3805 3790 3789 3814 3835 3852 3847 3865 3882 3893 3895
April May June July Aug Sept Oct Nov Dec Jan Feb Mar

10
Sickness
Target (2010/11)Executive
LeadMonthly
StatusDirection of Travel
Year to Date
Forecast Commentary
Sickness% Sickness Absence and WTE Days Lost DCA GREEN = GREEN GREEN
Validated absence level 0.2% lower than this month last year
• Overall validated absence level is 0.2% lower than for same month last year. Year to date validated level is less than last year’s average.
• Benchmarking data provided by the West Midlands for July 2010 showed SaTH to be 15th lowest of all 44 Trusts in the West Midlands.
• SaTH's sickness absence for 2009/10 was 4.3% (0.1% lower than 2008/9). A target of 4.2% has been set for 2010/11. It should be noted that the DoH have set a target of 3.39% for the West Midlands, to be achieved by 31st March 2013.
• Validated sickness average for April to June 2010 is 4.0%, mirroring 2009.
• Divisions continue to manage sickness absence in line with Trust policy and with support from HR, which includes using HR generated trigger lists to ensure early intervention in management of sickness absence, and completion of return to work interviews.
Actions:• There is a proposed new draft Management Sickness Absence policy, which is currently subject to consultation with staff-side representatives.
% Sickness Absence
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
%
%2010-11 4.0% 4.1% 4.1% 4.5% 4.7% 4.8%
%2010-11 Validated 3.8% 4.0% 4.1% 4.5%
%20010-11 YTD Validated 3.8% 3.9% 4.0% 4.1%
% 2009-10 Average 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3% 4.3%
% 2009-10 4.0% 4.0% 4.2% 4.7% 4.1% 4.1% 4.4% 4.3% 4.3% 4.5% 4.6% 4.5%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
WTE Days Lost
0
1000
2000
3000
4000
5000
6000
7000
WT
E D
ays L
ost
Certif ied (>7days) Lost WTE Days 5126 4671
Uncertif ied (1 to 7 days) Lost WTE Days 1080 1453
Validated Certif ied (>7days) Lost WTE Days 3666 4018 3947 4599
Validated Uncertif ied (1 to 7 days) Lost WTE Days 1124 1199 1273 1292
Total Lost WTE Days 2009-10 4627 4814 4890 5751 5038 4870 5554 5349 5554 5784 5358 5871
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar

1111
FinanceTarget (2010/11)
3
MonthlyStatus
Direction of Travel
Year to Date Commentary
Monitor Risk Rating Risk Score = 2 RED ═ RED Risk Score below target
•Month 7 EBITDA £1.409m (Plan £1.498m) : shortfall to plan £0.089m•Cumulative EBITDA £7.041m (Plan £9.786m) : shortfall to plan £2.745m•Month 7 I&E Surplus £0.275m (Plan Surplus £0.370m) shortfall to plan £0.095m•Cumulative Deficit £0.820m (Plan Surplus £.1.868m) : shortfall to plan £2.688m
•Unfavourable Emergency Threshold adjustment £0.262m in Month 7 (£1.465m cumulative) •Pay overspend £0.717m (£4.323m cumulative)•Pay spend Month 7 £15.138m (Months 1 to 6 average £15.238m) •Agency spend Month 7 £0.552m (Months 1 to 6 average £0.617m)•Working capital and cash management pressure continues.
•Trust plan £2.6m surplus for year, at Month 7 the forecast position is a £0.225m surplus.
Actions :
•Pay run rate reduction schemes identified, control totals issued to Divisions.
•All non pay spend for non-clinical items continues to be reviewed by senior finance officers prior to approval.
•Financial Performance reviews at SDU level.
Metric Value Rating
EBITDA margin 4.5% 2EBITDA, % achieved 71.9% 3ROA 2.8% 2I&E surplus margin -0.5% 2Liquid ratio 7.8 1
Weighted Average 2
2010/2011 EBITDA
0.000
2.000
4.000
6.000
8.000
10.000
12.000
Apr '10 May J un J ul Aug Sep Oct Nov Dec J an '11 Feb Mar
P lan (£m) (cum) Actual (£m) (cum)

12
Target (2010/11)Executive
LeadMonthly
StatusDirection of Travel
Year to Date
Forecast Commentary
Foundation Trust StatusTo achieve NHS Foundation Trust status in 2011 DoS RED = RED AMBER
Details for organisational transition continue to emerge in November. A revised trajectory for the
Trust’s FT application must be agreed with the SHA and informed to the DH during November 2010
Monitor Compliance Framework
Foundation Trust steering groups
Current PositionThe current assessment of performance against Monitor’s Compliance framework shows:• a financial risk rating remains of 2 (RED)• a governance risk rating which has moved to 3 (RED) during Q2.
Maintaining essential standards of safety and quality through the appropriate governance mechanisms is the primary focus of the Board at this time.
Establishing our NHS Foundation Trust (FT) trajectoryThe Trust will shortly be assessed by the SHA Regional Director of Provider Development on our ‘state of readiness’, where assurances are expected by the Department of Health that the organisation has a robust plan to achieve FT within the expected timescale. The assessment; an evidence based preparatory phase, will assure the DH of our fitness for purpose and will inform the SHA’s view in support of our FT application. This process, consisting of a Quality Review, and assessment of the capacity and capability of Board, will be undertaken between January and March 2011.
Foundation Trust Status
Actions:• Board assessment of trajectory for FT authorisation to be outlined in November 2010 for agreement with SHA. • Chairman asked to inform the Secretary of State of the proposed FT timetable by 30 November.• SHA assessment of organisational state of FT readiness during Q4.
Governance, Membership and ConstitutionSteering Group
Partnership Forum
Finance and PerformanceSteering Group
GovernanceFinance