1 Efficacy and safety of NRTI´s switch to tenofovir plus emtricitabine (Truvada ® ) vs. abacavir...
32
1 Efficacy and safety of NRTI´s switch to tenofovir plus emtricitabine (Truvada ® ) vs. abacavir plus lamivudine (Kivexa ® ) in patients with virologic suppression receiving a lamivudine containing HAART: The BICOMBO study Martinez E. 1 , Arranz J.A. 2 , Podzamczer D. 3 , Ribera E. 4 , Knobel H. 5 , Roca V. † 6 , Gutierrez F. 7 , Llibre J.M. 8 , Sans J. 2 , Barragan P. 3 , Clotet B. 9 , Dalmau D. 10 , Segura F. 13 , Arribas J.R. 14 , Cosin J 15 ., Force L. 16 , Palleras A. 17 , de los Santos I. 18 , Peraire J. 19 , Galo F. 20 , Pich J. 11 , de Lazzari E. 12 , Gatell J.M. 1 , for the BICOMBO study group 1Hospital Clinic Universitari, Infectious Diseases, Barcelona, Spain, 2Principe Asturias, Medicina, Oviedo, Spain, 3Bellvitge, Infectious Diseases, Barcelona, Spain, 4Vall d´Hebron, Infectious Diseases, Barcelona, Spain, 5Hospital del Mar, Infectious Diseases, Barcelona, Spain, 6Clinico San Carlos, Medicina, Madrid, Spain, 7Hospital de Elche, Medicina, Elche, Spain, 8Hospital Calella, Medicina, Calella, Spain, 9Fundacio IrsiCaixa, HIV, Barcelona, Spain, 10Mutua de Tarrasa, Medicina, Tarrasa, Spain, 11Hospital Clinic Universitari, Pharmacology, Barcelona, Spain, 12Hospital Clinic Universitari, Biostatistics, Barcelona, Spain, 13 Hospital Parc Tauli. Sabadell, 14 Hospital La Paz, Madrid, 15 Hospital Gregoria Marañon, Madrid, 16 Hospital de Mataro, 17 Hospital Son Llatzer, Baleares, 18 Hospital de la Princesa, Madrid, 19 Hospital Joan XXIII, Tarragona, 20 Hospital Sierrallana IAS meeting Sydney, Australia, July 22-26, 2007
-
Upload
amaya-ridout -
Category
Documents
-
view
219 -
download
0
Transcript of 1 Efficacy and safety of NRTI´s switch to tenofovir plus emtricitabine (Truvada ® ) vs. abacavir...

1
Efficacy and safety of NRTI´s switch to tenofovir plus emtricitabine (Truvada®) vs. abacavir plus lamivudine (Kivexa®) in patients with virologic suppression receiving a lamivudine containing
HAART: The BICOMBO study
Martinez E.1, Arranz J.A.2, Podzamczer D.3, Ribera E.4, Knobel H.5, Roca V. † 6, Gutierrez F.7, Llibre J.M.8, Sans J. 2, Barragan P.3, Clotet B.9, Dalmau D.10,
Segura F.13, Arribas J.R.14, Cosin J15., Force L.16, Palleras A.17, de los Santos I.18, Peraire J.19, Galo F.20, Pich J.11, de Lazzari E.12, Gatell J.M.1 , for the
BICOMBO study group1Hospital Clinic Universitari, Infectious Diseases, Barcelona, Spain, 2Principe Asturias, Medicina, Oviedo, Spain, 3Bellvitge, Infectious Diseases, Barcelona,
Spain, 4Vall d´Hebron, Infectious Diseases, Barcelona, Spain, 5Hospital del Mar, Infectious Diseases, Barcelona, Spain, 6Clinico San Carlos, Medicina, Madrid,
Spain, 7Hospital de Elche, Medicina, Elche, Spain, 8Hospital Calella, Medicina, Calella, Spain, 9Fundacio IrsiCaixa, HIV, Barcelona, Spain, 10Mutua de Tarrasa,
Medicina, Tarrasa, Spain, 11Hospital Clinic Universitari, Pharmacology, Barcelona, Spain, 12Hospital Clinic Universitari, Biostatistics, Barcelona, Spain, 13
Hospital Parc Tauli. Sabadell, 14 Hospital La Paz, Madrid, 15 Hospital Gregoria Marañon, Madrid, 16 Hospital de Mataro, 17 Hospital Son Llatzer, Baleares, 18
Hospital de la Princesa, Madrid, 19 Hospital Joan XXIII, Tarragona, 20 Hospital Sierrallana
IAS meetingSydney, Australia, July 22-26, 2007

2
Background
Tenofovir (TDF) plus emtricitabine (Truvada®) and abacavir (ABC) plus lamivudine (Kivexa®) are fixed dose combinations and the most commonly recommended and used nucleoside analogs backbone for initial antiretroviral therapy
Kivexa® has favourably compared with zidovudine plus lamivudine (Combivir®) while Truvada® has demonstrated superiority.
However, no head to head comparison has been performed so far between Truvada® and Kivexa®.

3
Objective
To compare the efficacy and safety of Truvada® vs. Kivexa® in patients with virologic suppression and receiving a lamivudine containing regimen.

4
Switch to Kivexa® † Switch to Truvada ® *
* Tenofovir 300 mg plus emtricitabine 200 mg + unchanged NNRTI or PI.† Abacavir 600 mg plus lamivudine 300 mg + unchanged NNRTI or PI.
Study Population (N = 335) Stable lamivudine based Regimen for > 6 months (VL < 200)
No contraindications for abacavir or tenofovir based regimens
No HLA screening
The study was conducted in Spain
Primary Analysis, Week 48
1:1 Randomization
Study Design

5
Primary end-point
– The proportion of patients with treatment failure for any reason through Week 48• Includes virologic rebound (> 200 cp/mL),
discontinuation of study therapy or lost to follow-up, progression to a new CDC category C event or death.
• Non-inferiority study of Kivexa® vs Truvada®. Upper limit of 95% CI of estimated difference < 12.5%.

6
Secondary end-points
– The proportion of patients with virologic failure at or prior to week 48• Confirmed on-study HIV RNA ≥ 200 copies/mL or
last on-study HIV RNA ≥ 200 copies/mL followed by discontinuation
– Time to treatment failure and to virologic failure
– CD4 changes– Safety– Changes of fasting plasma lipids, body fat,
bone mineral density and renal function

7
KIVEXA ® TRUVADA ®
N = 167 N = 166
Median Age, y 43 43
Gender, N (%)
Male 130 (78) 127 (77)
Risk group, N (%)
Heterosexual trans. 55 (35) 55 (35)
MSM 55 (35) 51 (32)
IDUs 47 (30) 53 (33)
AIDS, N (%) 63 (38) 65 (39)
Glomerular filtration rate (CG) ml/mit 102 97
Creatinine, mg/dL 1 0.9
CD4 < 200, cells/ mm3 13 (9) 15 (10)
Median CD4, cells/mm3 520 508
Baseline Characteristics

8
KIVEXA ® TRUVADA ®
N = 167 N = 166
TG > 500 mg/dL, N (%)1 (1 %) 3 (2 %)
Cholesterol > 240 mg/dL, N (%)22 (14%) 25 (16%)
LDL > 130 mg/dL, N (%)51 (38%) 49 (37%)
HDL < 40 mg/dL, N (%)26 (18%) 29 (20%)
ALT > 40 iu/ml, N (%) 23 (16 %) 36 (25 %)
AST > 40 iu/ml, N (%) 48 (31 %) 54 (35 %)
ALT or AST > 40 iu/ml, N (%) 49 (32%) 62 (40 %)
Baseline Characteristics

9
KIVEXA ® TRUVADA ®
N = 167 N = 166
ARV exposure, yr. 4.2 3.7
1st. ARV regimen, N (%) 48 (29) 29 (17)*
Efavirenz 94 (56) 88 (53)
Nevirapine, N (%) 56 (34) 62 (37)
PI, N (%) 17 (10) 16 (10)
Previous NRTI
ZDV+3TC, N (%) 59 (35) 48 (29)
d4T +3TC, N (%) 21 (13) 27 (16)
ddI +3TC, N (%) 31 (19) 23 (14)
TDF +3TC, N (%) 44 (26) 56 (34)
ABC +3TC, N (%) 12 (7) 18 (11)
Baseline Therapy
* P=0.01

10
Patient Disposition at week 48
Patients enrolled(n=335)
Assigned to KIVEXA ®
(n=167)Assigned to TRUVADA ®
(n=166)#
Continuing assigned therapy 138† (83%)Discontinued 29 (17%)
Adverse events 17 * Death 0Virological failure 2Lost to follow-up 5Patient decision 4Other 1
Continuing assigned therapy 144 (87%)Discontinued 22 (13%)
Adverse events 9Death 1**Virological failure 0Lost to follow-up 8Patient decision 2Other 2
† 2 subjects with virological failure and
1 with a new CDC event (cervix carcinoma)* 3 subjects lost to follow-up and 1 new CDC event
(Cryptosporidiosis)
# 2 additional were not eligible ** Cerebral hemorrage

11
Primary EndpointTreatment Failure through Week 48
-2 0 Treatment Failure KVX% – TVD%
12.5
95% CI for difference
-2.0 14.05.9
-2 0 Treatment Failure 12.5
95% CI for difference
-2.0 14.05.9
KIVEXA TRUVADA
0
5
10
15
20
25
30
19%
13%
32/167 22/166
Per
cen
tag
eo
fp
atie
nts
wit
htr
eatm
ent
fail
ure
KIVEXA TRUVADAKIVEXA ® TRUVADA ®
0
5
10
15
20
25
30
19%
13%
32/167 22/166
Per
cen
tag
eo
fp
atie
nts
wit
htr
eatm
ent
fail
ure

12
Secondary EndpointVirologic Failure (≥ 200 c/mL) through Week 48
0 KVX% – TVD%
12.5
95% CI for difference
6.0
0 Virologic Failure 12.5
95% CI for difference
0.05 2.4
KIVEXA TRUVADA ®KIVEXAKIVEXA ®
Pe
rce
nta
ge
of
pa
tie
nts
wit
h v
iro
log
ic f
ail
ure
2.4%
0%0
2
4
6
8
10
4/167 0/166

13
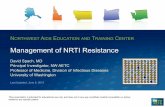
Secondary EndpointVirologic Failure (≥ 200 c/mL) through Week 48
4 patients developed VF in the Kivexa arm
4 / 4 no resistance tests before any ART regimen4 / 4 two or more previous ART regimens for 1-5 years. Never exposed to ABC 1 / 4 previous virologic failure. Wild type virus
VF developed between months 4-8 of the study
4 / 4 were receiving Kivexa + Nevirapine or Efavirenz2 / 4 genotypic test available at failure 75I, 184V, 219E, 101E, 181E 74V, 100I, 103 ,63S4 / 4 VL became undetectable with same (n=1) or different ART (n=3)

14
CD4 Changes
Median changes in CD4 cell count were: +44 cells/mm3 (KIVEXA ®) and – 2.7 cells/mm3 (TRUVADA ®) through Week 48 (p=0.032)
Me
dia
n C
ha
ng
e i
n C
D4
1,000
500
0
-500
-1,000
Weeks 4 16 32 48KVX TVD KVX TVD KVX TVD KVX TVD

15
Adverse Events
KIVEXA ® TRUVADA ®
N = 167N (%)
N = 166N (%)
Death 0 (0) 1 (1) &
Any AE 109 (65) 89 (54)*
AE leading to discontinuation: Total 17 (10) 9 (5) **
Suspected ABC hypersensitivity 9 (5) 0 (0)
Cefalea, fever, asthenia, diarrhoea 4 (2) 0 (0)
CNS 1 (1) 3 (2)
GI 1 (1) 2 (1)Rash 0 (0) 1 (1)
Kidney 0 (0) 2† (1)Lipodystrophy 1 (1) 1 (1)Liver 1# (1) 0 (0)
& Cerebrovascular accident; * P=0.02 ** P=0.004; † highest creatinine 1.1 and 6.1; # highest ALT/AST 42/ 59;

16
LAB Abnormalities
Liver Function Abnormalities (ALT/AST > 200)N (%)
KIVEXAN = 167
TRUVADA N = 166
ALT 1 (1%) 0 (0%)
AST 1 (1%) 1 (1%)
ALT or AST 1 (1%) 1 (1%)

17
0
12
7
0
-16
-9
-4 -4
-20
-15
-10
-5
0
5
10
15
Mg/dL (Month 12 - Month 0)
Change in Median Fasting Plasma Lipids
Triglycerides Cholesterol LDL HDL
P = 0.01 P = 0.001 P < 0.0001 P < 0.0001
KIVEXA TRUVADA
0 0
1
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
TC
/HD
L ratio
P =0.015

18
449
13280
164
0
100
200
300
400
500
600
700
800
900
1000
Fat g (Month 12 - Month 0)
Change in Mean Total and Limb Fat and Bone Mineral Density (n=47)
Total Fat Limb Fat
P = ns P = ns
0.0009
-0.0061
-0.04
-0.02
0
0.02
0.04
Bone Mineral Denisty mg/mL
(Month 12 - Month 0)
P = ns
KIVEXA ® TRUVADA ®N=23 N=24

19
RENAL FUNCTION. Median Changes From Baseline (mo. 12 – baseline)
KIVEXA ® TRUVADA ®
n Median (IQR) n Median (IQR)
∆ Creatinine , mg/dL
124 -0.03 (-0.1,-0.04)
129 -0.02 (-0.1, 0.03)
∆ GFR (CG), ml/mit
107 1.3 (-5, 7) 129 -0.5 (-5, 9)
Note: Only 1 patient (Truvada arm) developed a plasma creatinine >= 2 mg/dL

20
HLA TYPING
N (%)HLA-B05701+ HLA-B05701-
CASES (N=9) * 3 (33%) 6 (67%)
CONTROLS (N=14) 1 (7%) 13 (93%)
* KIVEXA ® interruption due to suspected Abacavir hypersensitivity

21
Conclusions
In patients switching from a lamivudine containing regimen:
For treatment efficacy, the Kivexa ® group did not meet the non-inferiority endpoint compared to the Truvada ® group– the difference was mainly driven by Kivexa
discontinuations due to suspected abacavir hypersensitivity
For the virologic efficacy, Kivexa ® met non-inferiority criteria compared to Truvada ®
– however, there were more failures with Kivexa ® than Truvada ® (2.4% vs 0%)

22
Conclusions
On switching from a lamivudine nucleoside backbone to either Kivexa ® or Truvada ® :
Retrospective HLA testing showed B5701+ in 3/9 cases of suspected HSR
Safety endpoints showed:
– A more favorable lipid profile (cholesterol, TG and LDL but not HDL) for those switching to Truvada ® vs Kivexa ®
– No differences in renal function or bone mineral density between Truvada ® and Kivexa ® treatment arms

23
BICOMBO Study GroupHOSPITAL CLINICE. MartínezJ.M. GatellJ. PichE. de LazzariJ. M. MiróJ. MallolasM. LoncàA. CrucetaH. AgellJ.A. Arnaiz
HOSPITAL BELLVITGEHOSPITALETD. PodzamczerP. Barragán
HOSPITAL VALL D’HEBRÓNBARCELONAE. RiberaA. Currán
HOSPITAL ELCHEF. GutiérrezM. MasiáS. PadillaE. Bernal
HOSPITAL MARBARCELONAH. KnobelA. GonzálezJ. Mercadal
HOSPITAL GREGORIO MARAÑÓN MADRIDJ. BerenguerM. SánchezM. RamírezI. Gutiérrez
HOSPITAL PRINCIPEASTURIAS MADRIDJ.A. ArranzJ. SanzE. CasasJ.M. Prieto HOSPITAL CLÍNICO
SAN CARLOS MADRID
V. Roca †M. Fuster
HOSPITAL JOAN XXIII TARRAGONA
F. VidalJ. PeraireM. Saumoy
HOSPITAL SON LLATZERPALMA MALLORCAA. Palleras
HOSPITAL MATARÓMATARÓLl. ForceP. Barrufet
HOSPITAL CALELLACALELLAJ.M. LlibreS. Valero
HOSPITAL MUTUA TERRASSAD. DalmauM. Cairó
HOSPITAL LA PAZMADRIDJ.R. ArribasM. MontesJ.M. Castro
HOSPITAL LA PRINCESA MADRIDI. de los SantosR. Carrillo
HOSPITAL GERMANS TRIAS I PUJOLBADALONAB. ClotetP. EcheverriaI. Bravo
HOSPITAL PARC TAULÍSABADELLF. SeguraE. Penelo
HOSPITAL SIERRALLANACANTABRIAF.G. Peralta
AND 335 PATIENTS !!!!

24
Backup slides

25
Time to treatment failure
p=0.609, long rank test
P=0.5P=0.12

26
Time to virological failure
p=0.609, long rank test
P=0.5P=0.5
P=0.19

27
Range of Possible Outcomesfor Non-inferiority Study Designs
∆ non-inferiority margin
A
B
C
D
E
95% confidence interval of the difference in effect
0
Favours the new drug Favours the active-control drug
Non-Inferior
Superior
Non-Inferiority, but Inferior
New drug is:
Non-Inferiority not demonstrated
Non-Inferiority not demonstrated, but inferior

28
LAB Abnormalities
Liver Function Abnormalities (ALT/AST > 200
when ALT/AST were > 40 at baselineN (%)
KIVEXA N = 49
TRUVADAN = 62
ALT 1 (2 %) 0 (0%)
AST 1 (2%) 1 (2%)
ALT or AST 1 (2%) 1 (2%)

29
Lipid lowering agents
N (%)KIVEXA N = 167
TRUVADAN = 166
Baseline 11 (7) 18 (11)
At mo. 12 18 (11) 21 (13)

30
PLASMA LIPIDS ABOVE/BELOW NCEP RECOMMENDATION FOR TREATMENT
-10
0
10
20
Kivex Truv Kivex Truv Kivex Truv Kivex Truv
TG>500 Cholest>240 LDL>130 HDL< 40
PERCENTAGE (Mo. 12 - Mo. 0)

31
Metabicombo
Mitochrondial toxicity
Patients never exposed to abacavir
(n=155) or tenofovir (n=110)
Planned sub-studies / subanalysis

32
Virologic Failure (≥ 200 c/mL)Treatment Failure
KIVEXA TRUVADA
0
5
10
15
20
25
30
21%
13%
32/155 14/110
Difference Estimate (95% CI) 8% (–1.4%, 16.8%) 2.6% (-0.08%, 6%)
Treatment Failure and Virologic Failure (≥ 200 c/mL) through Week 48 among patients never exposed to abacavir or tenofovir
0
5
10
15
20
25
30
3%
0%
4/155 0/110
Pro
po
rtio
n o
f p
atie
nts
Pro
po
rtio
n o
f p
atie
nts