1 Dr. Zohair Al aseri FRCPC Emergency Medicine FRCPC Critical Care Medicine Assistant Professor &...
69
1 Dr. Zohair Al aseri FRCPC Emergency Medicine FRCPC Critical Care Medicine Assistant Professor & Chairman Dept. of Emergency Medicine College of Medicine King Saud University Hospitals Anaphylax Anaphylax is is
-
Upload
sophia-mitchell -
Category
Documents
-
view
224 -
download
1
Transcript of 1 Dr. Zohair Al aseri FRCPC Emergency Medicine FRCPC Critical Care Medicine Assistant Professor &...

1
Dr. Zohair Al aseri
FRCPC Emergency Medicine
FRCPC Critical Care Medicine
Assistant Professor &
Chairman Dept. of Emergency Medicine
College of Medicine
King Saud University Hospitals
AnaphylaxisAnaphylaxis

2
52 y o m pt presented to er c/o
Vomiting blood 2 times @ home
NO other complaints
PMH : PUD 10 y ago, HTN
Med : ACEI & metoprolol
V/S : tachy
CNS, CHEST& HEART exam were normal
Hg 50 ,
blood transfusion started
CASE 1

3
52 y o m pt presented to ER c/o vomiting blood
GI consulted @ 1.00 am , came & decided to do endoscope in ER
Procedure started by sedation propafol iv & lidocain spray
Pt became hypotensive , itching all over ,a/w swelling
GI staff decided to leave & come back again If the pt became more stable.
CASE 1

4
• What is your 1st line treatment ?
• What is your diagnosis?
• What are the indications of intubation in this pt?
• What are your choice of medication for induction & paralysis ?
• What about post intubation sedation & pain control ?
• What is your plan if your pt remain hypotesive after resuscitation?
52 y o m pt presented to ER c/o vomiting blood
CASE 1

5
Definition
Anaphylaxis is derived from the Greek word ana meaning backward or against and phylaxis meaning protection
There is no universally accepted clinical definition of anaphylaxis
AnaphylaxisAnaphylaxis

6
Data regarding the incidence and prevalence of
anaphylaxis and the number of deaths
caused by it are limited.
Epidemiology in SA
AnaphylaxisAnaphylaxis

7
Foods Medications (eg, antibiotics) Aspirin NSAID Venoms Latex Allergen vaccines Animal or human proteins Polysaccharids Exercise
Anaphylactic (IgE dependent)
EtiologyEtiology

8
Anaphylactoid (IgE independent)
Multimediator complement activation-
Radiocontrast media
ACEI
Ethylene oxide gas on dialysis tubing???
Protamine
AnaphylaxisAnaphylaxis
EtiologyEtiology

9
Cytotoxic
Transfusion reactions to cellular elements (IgG,Igm)
AnaphylaxisAnaphylaxis
EtiologyEtiology

10
Etiology
Idiopathic anaphylaxis is one of the most common causes, accounting for approximately one third of cases in retrospective studies
Its a diagnosis of exclusion.
AnaphylaxisAnaphylaxis

11
Pathophysiology
Some authors reserve the term anaphylaxis only for IgE-dependent events and the
term anaphylactoid to describe IgE-independent reactions that otherwise are
clinically indistinguishable.
AnaphylaxisAnaphylaxis

12
PathophysiologyPathophysiology
AnaphylaxisAnaphylaxis

13
o Histamineo Tryptaseo Platelet-activating
factoro Heparin
o PGDo Leukotriene o Histamine-releasing
factor o Chymase
Pathophysiology
Biochemical mediatorsBiochemical mediators

14
• Postmortem serum tryptase might be useful in establishing anaphylaxis as the cause of death in subjects experiencing sudden death.
Increased postmortem tryptase levels have been
reported • 12% of healthy adults with sudden death• 40% of victims of (SIDS)
Pathophysiology
AnaphylaxisAnaphylaxis

15
•Recent findings: Anti-IgA is not responsible for most reactions.
•Anti-haptoglobin antibodies are responsible for more reactions than anti-IgA in Japan.
•The cause of most reactions is still not known.
•The incidence of reactions to platelets is the highest compared with fresh frozen plasma and red blood cells.
Anaphylactic transfusion reactions
Anaphylactic transfusion reactions. Current Opinion in Hematology. 10(6):419-423, November 2003.Gilstad, Colleen W.

16
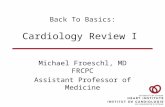
1–4:100
1–4:100
1:1,000
1:5,000
1:12,000
1:100,000
1:150,000
Febrile (FNHTR)
Allergic
Delayed hemolytic
TRALI
Acute hemolytic
Fatal hemolytic
Anaphylactic
Risks of Transfusion Complications

17
•The most frequent potentially severe outcomes for red cell transfusion were hemolytic reactions and volume overload
•for platelet transfusion were major allergic reactions and bacterial contamination
Risks associated with transfusion of cellular blood components in Canada
Comprehensive review of risks associated with allogeneic red blood cell and platelet transfusions in Canada.

A 9-year retrospective review
"severe allergic" reactions occurred in 1:53,612 blood components•1:9630 platelets •1:28,831 FFP•1:57,869 RBC transfusions
Domen RE, Hoeltge GA: Allergic transfusion reactions. Arch Pathol Lab Med 2003, 127:316-
320. Nine-year retrospective review of all transfusion reactions reported to the Cleveland
Clinic transfusion service

19
Generalized urticaria and angioedema are the most common manifestations .
Cutaneous manifestations might be delayed or absent in rapidly progressive anaphylaxis.
Manifestations
SKIN

Increased skin temperature (redistribution of blood)
Urticaria (hives) Flushing
Periorbital edema Perioral edema Diaphoresis Itching Burning
Manifestations
SKIN

21
The next most common manifestations are The respiratory
symptoms
Manifestations
AnaphylaxisAnaphylaxis

22
Manifestations
SIGNS Increased RR Stridor (laryngeal edema) Wheezing (bronchospasm) Decreased pulmonary
compliance Pulmonary edema Respiratory failure
SYMPTOMS Dyspnea Chest discomfort Coughing Sneezing
Respiratory

23
Manifestations
Hypotension Increased HR Decreased svr Dysrhythmias
• Retrosternal pain• MI• Cardiac arrest • ECG Changes
CVS

24
Manifestations
CNS
Non-specific Disorientation LOC Dizziness Light-headedness Malaise
GI
Non-specific
Vomiting Diarrhea Nausea Abdominal pain
AnaphylaxisAnaphylaxis

25
Dyspnoea 61 (43) Wheeze 50 (35.2) Vomiting 27 (19.0) B.spasm 26 (18.3) Syncope &
dizziness 21 (14.8) R. rate ≥25 19 (13.4)
• Laryngeal edema 15 (10.6) • Hoarseness 14 (9.9) • SBP <90 mmHg 13 (9.2)• GCS <15 4(2.8) • Loc 3 (2.1) • Stridor 2 (1.4)• Cyanosis 2 (1.4)
ED AED Anaphylaxisnaphylaxis
A review of 142 patients in a single year
Anthony F. T. Brown MB Brisbane, Australia (J Allergy Clin Immunol 2001
133 (94%) of the 142 patients had cutaneous features.

26
Fever
Hypotension
Generalised oozing from wounds or puncture sites
Haemoglobinaemia
Haemoglobinuria
Transfusion Reaction
Signs

27
Feeling of apprehension or something wrong
Agitation
Flushing
Pain at venepuncture site
Pain (abdomen , flank or chest )
Transfusion Reaction
Symptoms

28
TREATMENT Stop Administration of Antigen (blood)
Establish and maintain a/w
100% oxygen administration,
intravascular volume expansion.
Epinephrine
Systemic glucocorticosteroid
AnaphylaxisAnaphylaxis

29
AIR WAY
Low Threshold
Tube Size?
Induction Agent?
paralytic agent?
TREATMENTTREATMENT

30
Bronchospasm
For bronchospasm resistant to epinephrine
AnaphylaxisAnaphylaxis
Give Nebulized (albuterol, salbutamol)
repeated doses

31
Persistent Bronchospasm
Aminophylline, a phosphodiesterase inhibitor, weak bronchodilator that also increases R&L ventricular contractility and decreases pulmonary VR.
An IV loading dose of 5 to 6 mg/kg of aminophylline given over 20 m. should be followed by an infusion of 0.5 to 0.9 mg/kg /h
AnaphylaxisAnaphylaxis

32
To achieve rapid intravenous induction with minimal hemodynamic effect and little respiratory depression, etomidate
(Amidate) is the agent of choice.
IV Induction agent
Etomidate
AnaphylaxisAnaphylaxis & IVIA & IVIA

33
SEDATIVES
IV DOSE (mg/kg)
ONSET(min)
Effect on BP
Effect on ICP
Midazolam 0.2 – 0.4 1 – 2 Minimal Minimal
Etomidate 0.2 – 0.4 < 1 Minimal/
Thiopental 2 – 5 < 1
Ketamine 1 – 2 1 Minimal/
Propofol 2 – 3 < 1
AnaphylaxisAnaphylaxis & IVIA & IVIA
IV Induction agent

34
Volume Expansion
Volume expansion is important
Initially, 1 to 3 L of RL ,NS
AnaphylaxisAnaphylaxis

35
Catecholamines
Life-saving
First-line catecholamines include epinephrine
Dopamine????
AnaphylaxisAnaphylaxis

36
EPINEPHRINE
α1 -adrenergic : Vasoconstriction
β1 -adrenergic Vasoconstriction Increased peripheral vascular resistance Increases myocardial contractility Decreased mucosal edema)
AnaphylaxisAnaphylaxis

37
EPINEPHRINE
β2 -adrenergic effects are of primary importance
Bronchodilation
Release of histamine, tryptase, and other chemical
mediators of inflammation from mast cells and
basophils by cAMP production)
AnaphylaxisAnaphylaxis

38
EPINEPHRINE
There are no absolute contraindications to epinephrine administration in
anaphylaxis
Contraindication

39
HOW DO YOU GIVE IT?
The UK consensus panel on emergency guidelines states that the subcutaneous route of administration
for epinephrine has “no role” in anaphylaxis
EPINEPHRINEEPINEPHRINE

40
Epinephrine absorption in adults
IM versus SQ injection
Prospective, randomized, blinded placebo- controlled 6-way crossover study in healthy allergic men age 18 to 35 y
CONCLUSION IM injection of epinephrine into the thigh
is the preferred method of administration in the initial treatment of anaphylaxis
F. Estelle R. Simons MD (Journal of Allergy and Clinical Immunology 2001)

41
Epinephrine absorption in children
Prospective, randomized, blinded, study in 17 children with a history of anaphylaxis
SQ V/S IM from autoinjector.
Plasma epinephrine concentrations, HR, BP, and adverse effects were monitored.
F. Estelle R. Simons MD Winnipeg, Manitoba, Canada Allergy and Clinical Immunology
AnaphylaxisAnaphylaxis

42
The IM route of injection is preferable.
Epinephrine SQ 0.27 ± 0.04
Epinephrine IM 0.3
Epinephrine absorption in childrenEpinephrine absorption in children

IM EpinephrineIM Epinephrine
The IM route has several benefits:
• There is a greater margin of safety.
• It does not require intravenous access.
• The IM route is easier to learn.
The best site for IM injection is the anterolateral aspect of the middle third of the thigh.

Adrenaline IM dose – adults0.5 mg IM (= 500 micrograms = 0.5 mL of 1:1000) adrenaline
Adrenaline IM dose – children> 12 years: 500 micrograms IM (0.5 mL) i.e. same as adult300 micrograms (0.3 mL) if child is small or prepubertal
> 6 – 12 years: 300 micrograms IM (0.3 mL)> 6 months – 6 years: 150 micrograms IM (0.15 mL)< 6 months: 150 micrograms IM (0.15 mL)
IM EpinephrineIM Epinephrine

45
IV EPINEPHRIN
IV Epiniphrine
Indications
1) Shock
2) Coma & hypotension
3) Stridor + a/w edema
4) No response to I/M epiniphrine

46
IV IV EPINEPHRINEPINEPHRIN
0.1 mg (0.1 ml) of 1:1,000 with 10 ml of n/s.
This is equivalent to a 100 mcg bolus given at 10 mcg/min.
Once therapy has begun, a continuous infusion could be delivered with 0.5 to 5 mcg/min titrated to clinical response.
AnaphylaxisAnaphylaxis

47
Epinephrine infusions
Useful in patients with persistent hypotension or bronchospasm after initial resuscitation
Infusions should be started at 5 to 10 μg/min (approximately 0.05–0.1 μg/kg per minute) and titrated to correct hypotension.
AnaphylaxisAnaphylaxis

48
Catecholamine Infusions
Norepinephrine infusions may be required
5 to 10 μg/min (0.05–0.1 μg/kg per mi) and titrated to correct hypotension.
AnaphylaxisAnaphylaxis

Inject hydrocortisone slowly intravenously or intramuscularly,
The dose of hydrocortisone for adults and children depends on age:>12 years and adults: 200 mg IM or IV slowly>6 – 12 years: 100 mg IM or IV slowly>6 months – 6 years: 50 mg IM or IV slowly<6 months: 25 mg IM or IV slowly
AnaphylaxisAnaphylaxis
Steroid

50
Antihistamine
Ranitidine50 mg in adults (1 mg/kg) in children,
diluted in 5% dextrose to a total volume of 20 mL and injected IV over 5 minutes.
Cimetidine (4 mg/kg) may be administered to adults,
but no pediatric dosage in anaphylaxis has been established.
AnaphylaxisAnaphylaxis

51
Improve outcomes???
a randomized, double-blind, 91 adult patients with acute allergic syndromes were treated with
1. 50 mg of diphenhydramine and Placepo
2. 50 mg of diphenhydramine and 50 mg of ranitidine
Lin RYAnn Emerg Med. November 2000
HH11 and H and H22 antagonists antagonists

52
Ranitidine Placebo(n=48) (n=43)
Methylprednisolone 28 27
Additional H2 blocker
2 0Epinephrine 17 9Additional antihistamine
2 10Albuterol nebulization
6 7
Treatment
HH11 and H and H22 antagonists antagonists
Lin RYAnn Emerg Med. November 2000
Antihistamine

53
Antihistamine
Conclusion: These findings favour the recommendation for
using combined H1 and H2 antihistamines in acute allergic syndromes.
Lin RYAnn Emerg Med. November 2000
AnaphylaxisAnaphylaxis

Unlikely to be lifesaving in a true anaphylaxis Inject chlorphenamine slowly IV or IM The dose of chlorphenamine depends on age:
>12 years and adults: 10 mg IM or IV slowly >6 – 12 years: 5 mg IM or IV slowly >6 months – 6 years: 2.5 mg IM or IV slowly <6 months: 250 micrograms/kg IM or IV slowly
54
Antihistamine
AnaphylaxisAnaphylaxis

55
Biphasic Anaphylaxis
Rare. Rates between 5% to 20%. Recurrence Ranging from mild to sever life-
threats
TTT
Prolonged observation is required.
AnaphylaxisAnaphylaxis

56
Risk Of Biphasic Anaphylaxis
Joyce M. Lee MD Children's Hospital, Harvard Medical School
Biphasic Anaphylactic Reactions in Paediatrics
Iincidence :6%
Delayed epinephrine injection
Steroids do not prevent biphasic reactions
The time from the onset of symptoms to the reaction

57
Anaphylaxis in Pregnancy The management of anaphylaxis in pregnancy
consists of
Maternal Resuscitation
Close monitoring of the fetal status
Iimmediate delivery of the fetus if compromised.
AnaphylaxisAnaphylaxis

58
Treatment depends on the severity of the reaction and consists of
Fluid resuscitation Oxygen Epinephrine H1 and H2 blockers Corticosteroids.
Anaphylaxis in Pregnancy
AnaphylaxisAnaphylaxis

59
What are the bad prognostic signs of anaphylaxis?

60
β-Adrenergic blockade
Paradoxical bradycardia
Profound hypotension
Severe bronchospasm.
These agents might impede treatment effectiveness with epinephrine.
AnaphylaxisAnaphylaxis

61
β-Adrenergic blockade
• Glucagon, 1-5 mg (20-30 μg/kg [maximum, 1 mg] in children), IV over 5 minutes,
followed by an infusion of 5-15 μg/min.
(Aspiration precautions should be observed because glucagon may cause n & v.)
TTT:

62
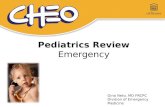
release of epinephrine
from the adrenal cortex
Hypotension
release of ACE leading to the production of angiotensin 2, a
potent vasocontrictor
Vasocontriction &
Decreased
Vascular Permeability
Site of action of
ACE inhibitors &
angiotensin 2 antagonist
Site of action of
ACE inhibitors &
angiotensin 2 antagonist
Persons taking ACEI and/or angiotensin II antagonists
will have a diminished compensatory response
Persons taking ACEI and/or angiotensin II antagonists
will have a diminished compensatory response
ANAPHYLAXIS
and ACE

63
The heart in anaphylaxis
High-dose epinephrine administered iv (ie, rapid progression to high dose).
1-3 mg (1:10,000 dilution) slowly administered iv over 3 minutes
3-5 mg administered iv over 3 minutes
4-10 μg/min infusion.
1
2
33
AnaphylaxisAnaphylaxis

64
OUTCOME
a)RESPIRATORY b)LOC c)CVS
What is the NO. 1 cause of death in anaphylaxis?
AnaphylaxisAnaphylaxis

65
Causes of Death In Anaphylaxis
AnaphylaxisAnaphylaxis


67
PROGNOSIS
Bad prognostic signs
A/W B.Asthma Rapid manifestations after exposure Late epi inj. epi requirement CAD B.B ACEI
be aware & prepared

Questions
68
AnaphylaxisAnaphylaxis

69
Ranitidine 50 mg in adults (1 mg/kg) in children, diluted in
5% dextrose to a total volume of 20 mL and injected IV over 5 minutes
IV Epinephrine***
Diphenhydramine 50 mg of IV/IM
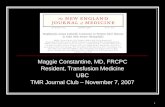
Anaphylaxis Algorithm (Hypotension due to Antigen )
Check ABCs in Monitored bed
Methylprednisolone (Solu-Medrol) 125 mg IV
•100% oxygen administration, establish and maintain a/w
0.3 mL Epinephrine 1:1,000 IM* in lateral aspect of the thigh Repeated dose if still hypotensive in 3-4 minutes
Reassess ABCs
Hypotension YesNO
High Risk Patient**
NO
Observe for 6 hours
• •Airway compromise •Requirement of high doses of epinephrine•History of Cornary Artery Disease •History of B.Asthma•Patient on B.Blockers or ACEI
IV N/S 500—1000ccBolus
For bronchospasm resistant to epinephrine give nebulized (salbutamol)
Stop Administration of Antigen (i.e. blood)
***IV Epinephrine0.1 mg (0.1 ml) of 1:1,000 with 10 ml of n/s .
this is equivalent to a 100 mcg bolus given at 10 mcg/min .a continuous infusion of 0.5 to 5 mcg/min titrated to clinical response .
Epinephrine should not be administered IV to patients with normal BP
Start Glucagon, 1-5 mg (20-30 μg/kg ( maximum, 1 mg in children,)
iv bolus over 5 minutes followed by infusion of 5—15 μg/min.
Still Hypotension
Reassess ABCs
Is the patient on B. Blockers?
ICU Admission
D/C Home with prednisone 50 mg once per day for 5 days
,diphenhydramine 25 – 50 mg po Q 6—8 h for 2 days and consider 0.3 mg epi pen prescription in food allergy induced anaphylaxis
Stable
Unstable
Yes
Low threshold for Intubaion if any one of the following present*
Persistent airway and/or sever tongue swelling Respiratory FailureRespiratory Distress Hypoxia
Reassess ABCs
Prepared by Dr Zohair Alaseri Feb 2006
*Prepare for difficult air way and call anaesthesia for back up
NO
Yes
Yes
NO
**High Risk Patient