1 Douglas Carlan, MD Hand and Upper Extremity Eaton Orthopaedics, LLC Carillon Outpatient Center...
47
1 Douglas Carlan, MD Hand and Upper Extremity Eaton Orthopaedics, LLC Carillon Outpatient Center Overcoming Rotator Cuff Injuries
-
Upload
liliana-norman -
Category
Documents
-
view
213 -
download
0
Transcript of 1 Douglas Carlan, MD Hand and Upper Extremity Eaton Orthopaedics, LLC Carillon Outpatient Center...
1
Douglas Carlan, MDHand and Upper Extremity
Eaton Orthopaedics, LLCCarillon Outpatient Center
Overcoming Rotator Cuff Injuries
2
• Anatomy• Impingement• Rotator Cuff Tear• Rehab• Prevention
Overcoming Rotator Cuff Disease

Rotator Cuff Disease
• Common cause of disability in adults• Simple tasks may be painful• 2,000,000 doctor visits• 400,000 Americans/yr - surgery for RC dz• 200,000 Repairs
• Prevalence • Asx adults >60yo - 28% tear• Asx adults >80yo - 51% tear 3

What is the Shoulder?
• Shoulder -• 3 bones• 4 joints• 4 rotator cuff muscles• Multiple tendons, muscles, capsule
structures
4
5
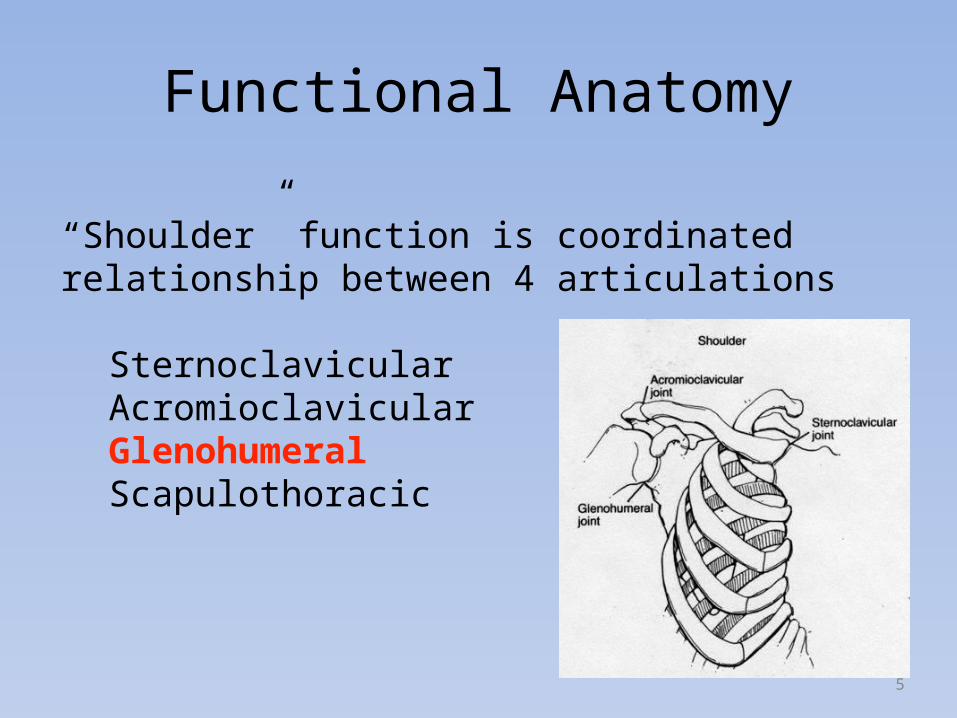
“Shoulder” function is coordinated relationship between 4 articulations
SternoclavicularAcromioclavicularGlenohumeralScapulothoracic
Functional Anatomy
6
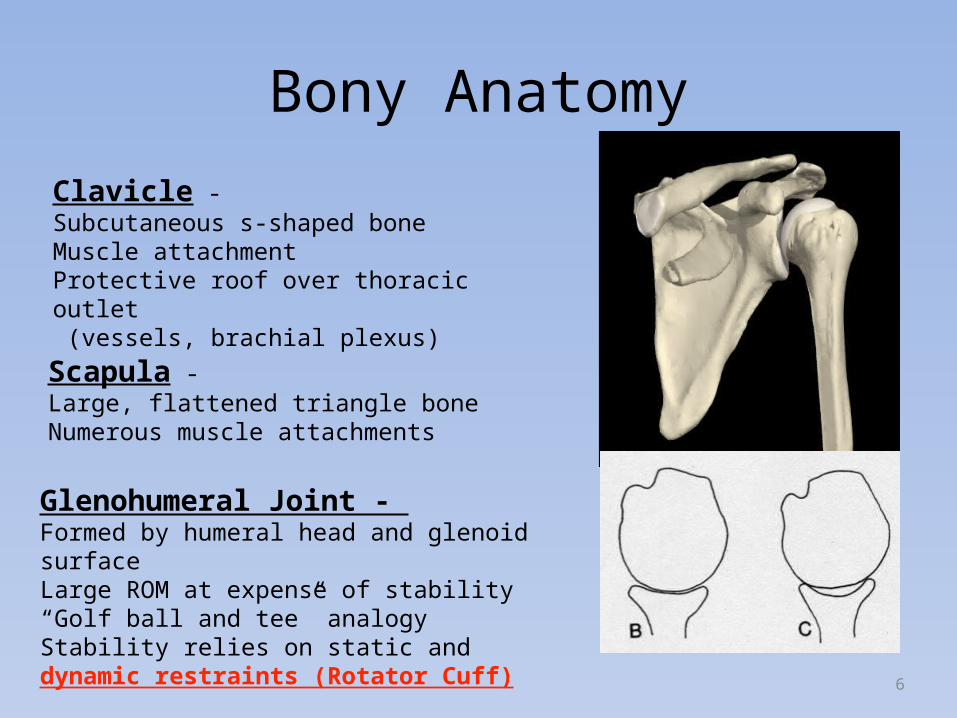
Clavicle - Subcutaneous s-shaped boneMuscle attachmentProtective roof over thoracic outlet (vessels, brachial plexus)
Bony Anatomy
Scapula - Large, flattened triangle boneNumerous muscle attachments
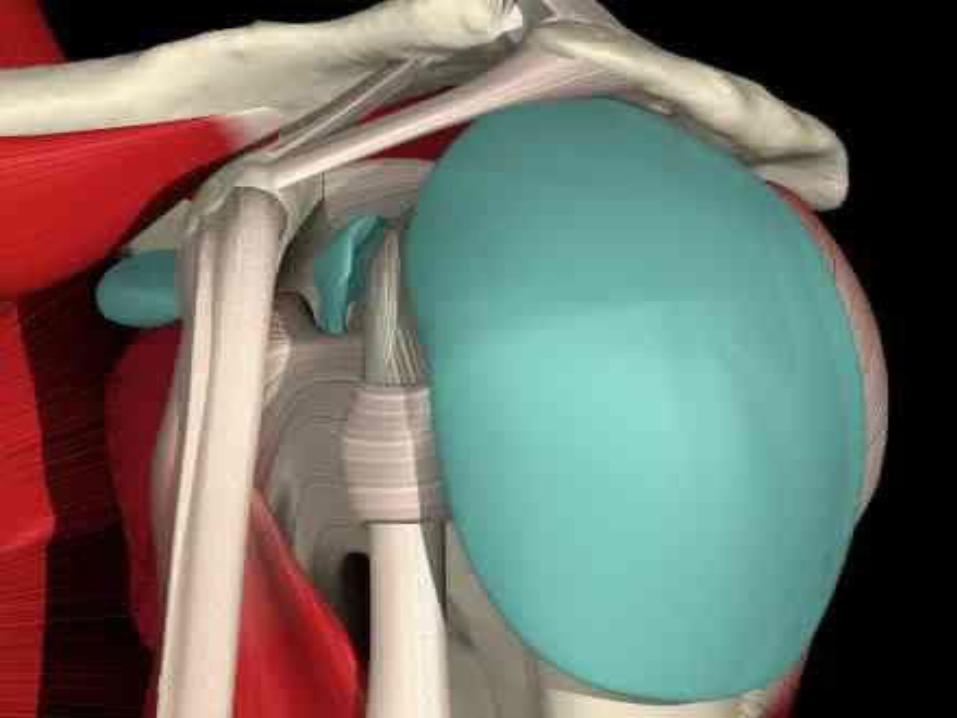
Glenohumeral Joint - Formed by humeral head and glenoid surfaceLarge ROM at expense of stability“Golf ball and tee” analogyStability relies on static and dynamic restraints (Rotator Cuff)

7
Glenohumeral MusclesRotator cuff muscles
Supraspinatus -Abd
Infraspinatus - ER
Teres minor - ER
Subscapularis - IR

8
Glenohumeral MusclesDeltoid
• Large bulky muscle
• Tripennate origin (clavicle, acromion, scapular spine)
• Insertion: deltoid tubercle
• Very important abduction
• Flexion and extension

9

10

11
12

13

14
15
16

17

18
• Impingment• Rotator Cuff Tear
Rotator Cuff Disease

19
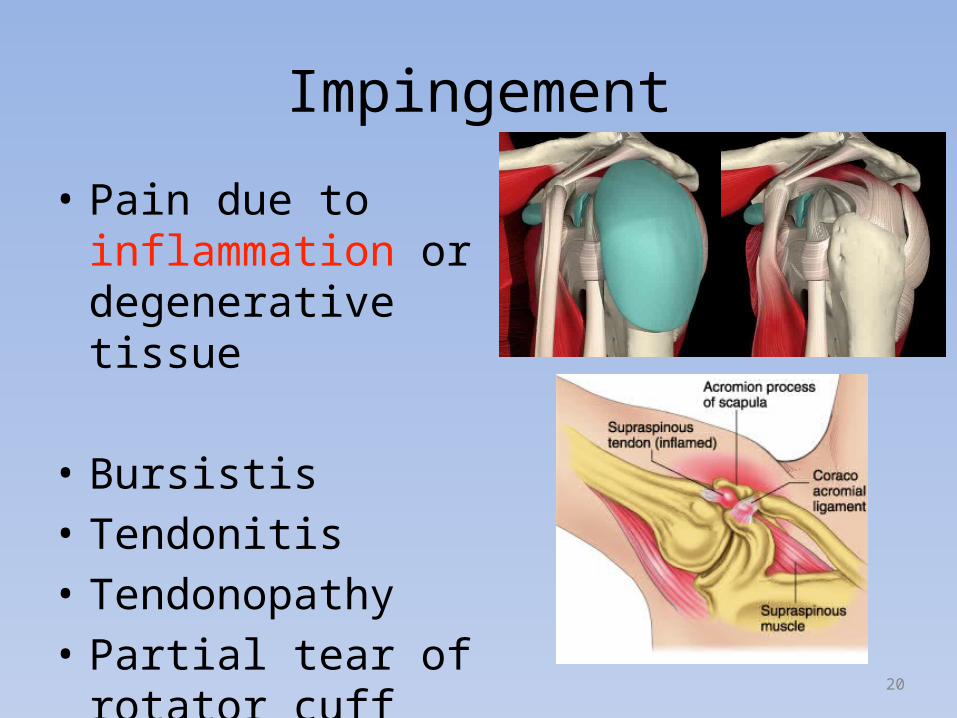
• Most common cause of pain in the adult shoulder
• Imflamed or degerative tissues between humeral head and acromion
• Causes pain and limits movement
Impingement
20
• Pain due to inflammation or degenerative tissue
• Bursistis• Tendonitis• Tendonopathy• Partial tear of rotator cuff
Impingement
21
• Risk Factors
• Idiopathic• Minor Trauma • Athletes in overhead sports– Swimming, baseball, tennis
• Repetitive lifting or overhead work– construction, painting
Impingement

22
• Symptoms• Minor pain – activity and at rest• Pain in anterior and lateral shoulder• Pain with reaching or lifting• Night pain• Pain when lowering arm from elevation• Pain with overhead sports• Tenderness• Loss of Motion
Impingement
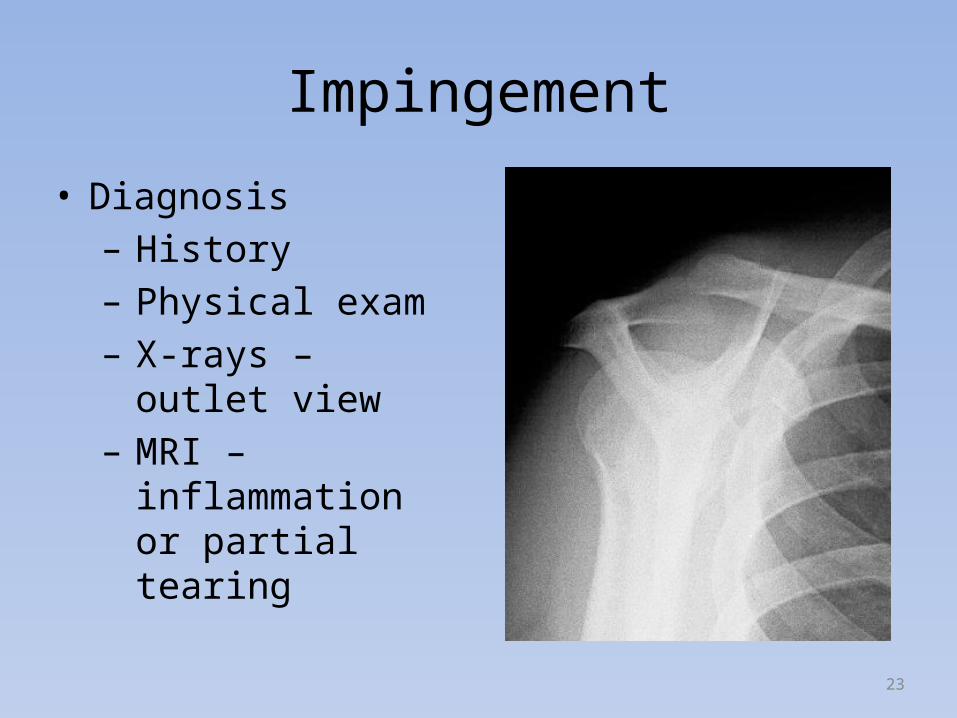
Impingement
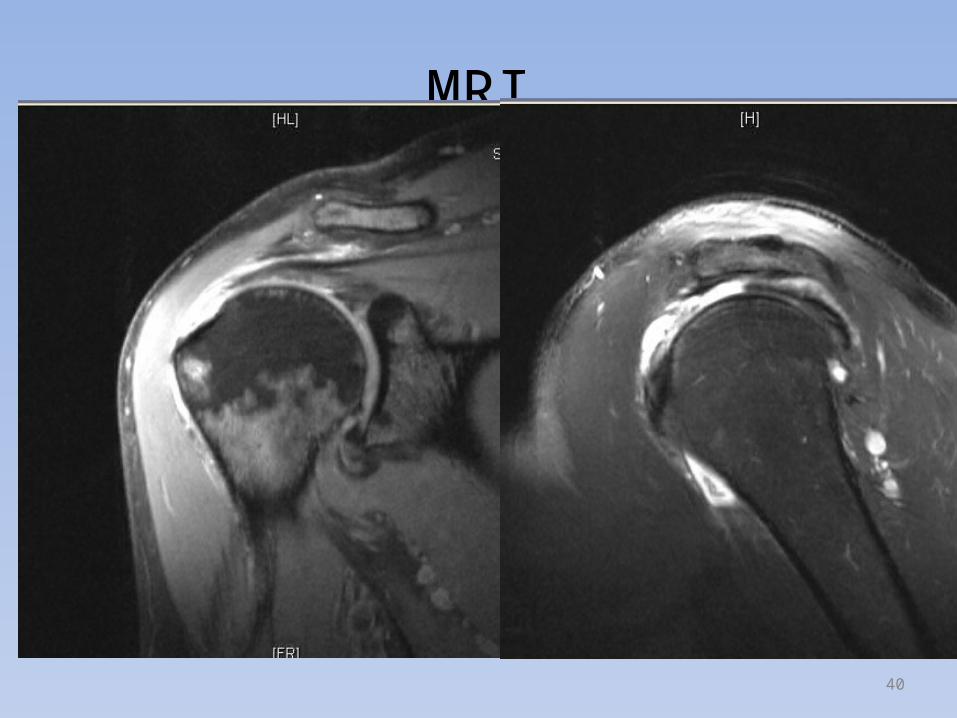
• Diagnosis– History– Physical exam– X-rays – outlet view– MRI – inflammation
or partial tearing
23

24

25
• Treatment – non-surgical– Rest, avoid overhead activity– NSAID’s– RC Strengthening Program– Corticosteroid Injection– Takes several weeks to months to resolve
Impingement
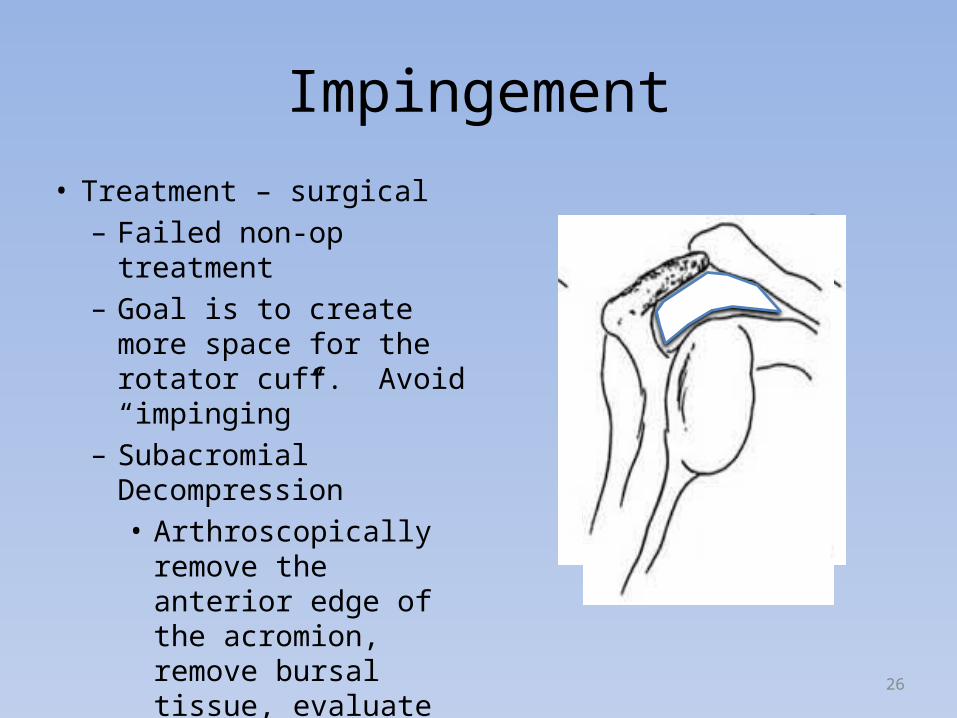
Impingement• Treatment – surgical– Failed non-op treatment– Goal is to create more space
for the rotator cuff. Avoid “impinging”
– Subacromial Decompression• Arthroscopically remove
the anterior edge of the acromion, remove bursal tissue, evaluate the remainder of the shoulder
26

Impingment
• Post-surgical– Sling for 1-2 weeks as
needed– Begin exercises in
first or second week– 2-4 months for
complete relief of pain
– May take up to 1 year
27

Impingement
28

29

30
• Common source of pain• Incidence increases with age 50-60’s• Caused by degeneration of the tendon• Can be caused by acute trauma – usually
younger population• Incidence is up to 50% in people without
symptoms – highest in older population• Can have tear with normal, functioning
shoulder
Rotator Cuff Tear
31
• Extrinic causes• Mechanical wear, scapular dyskinesia
• Intrinsic causes• Tendon hypovascularity, age-related
degeneration, micro or macro trauma
Rotator Cuff Tear

32
• Acute • Event, Younger Patient
• Acute extension of Chronic Tear• Event, Older
• Chronic• insidious
Rotator Cuff Tear
33
Rotator Cuff Tear
• Natural History• A high number of patients over 60 have RCT• Not all symptomatic• 40% of those with tears with enlarge• 80% of enlarging tears become symptomatic• Once symptoms develop, likely to worsen

Treatment
• Repair
• younger age• acute• muscle quality
34
• Nonop
• elderly• chronic• muscle atrophy• comorbidities
• DM, smoking, osteoporosis

35
• Treatment – non-surgical• Activity modification, Gentle therapy• 50% of patients with relief.• Better in pts with shorter duration of
symptoms and small tears.• May become symptomatic in the future, tear
may enlarge• Nonop vs repair study (<3cm)- better
outcome in repair group but small difference
Rotator Cuff Tear
36
• Treatment – surgical• Younger patients• Weakness• Traumatic tears• Large tears• Repair tendon back to humeral head• Many methods, all have shown success
• Open versus Arthroscopic
Rotator Cuff Tear

37
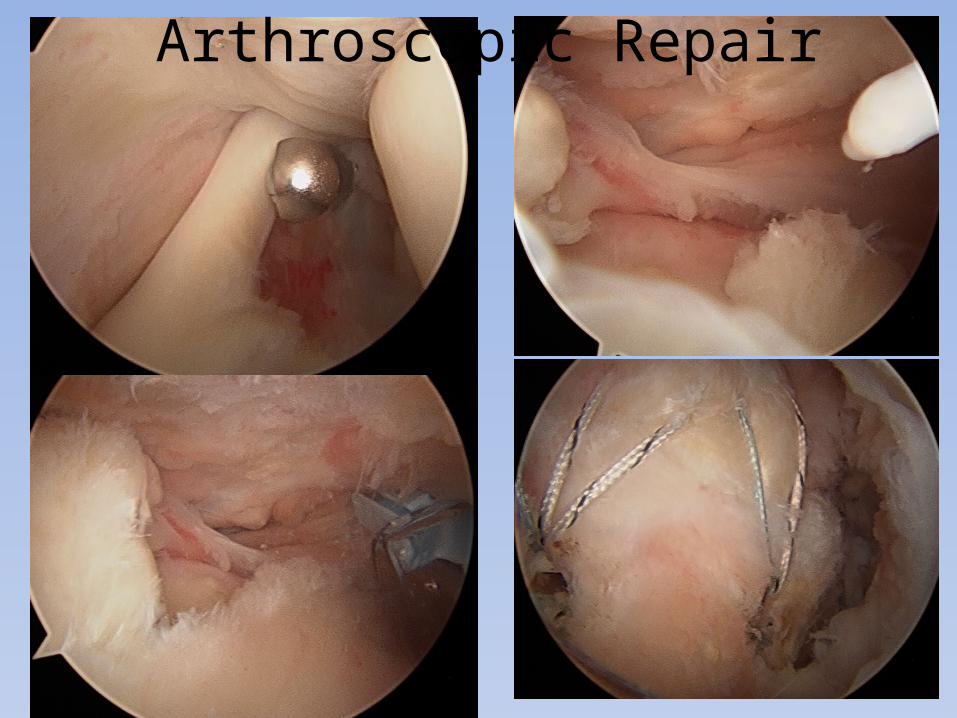
• Arthroscopic Repair• 80-95% satisfactory results – pain relief and
functional gains• Rehab – long and slow
• 6 weeks in sling• 3 months until strengthening• 4-6 months until functional recovery
Rotator Cuff Tear

38

39
40
MRI

41
MRI

42
Arthroscopic Repair
43
Arthroscopic Repair

44
Arthroscopic Repair

45
Arthroscopic Repair
46
• Rehab• Much debate• When?• How much?• Protocol?• Sling duration?
Recovery
47
• Early PT• Better early function, motion, pain level • Equivalent @ 24weeks• Slightly higher retear rate
• Conclusion• Tailor plan to meet individual needs
Rehabilitation