1 Depression and management Guidelines Prof. Dr. Momtaz AbdEl Wahab Prof. of psychiatry Cairo...
90
1 Depression and management Guidelines Prof. Dr. Momtaz AbdEl Wahab Prof. of psychiatry Cairo University
-
Upload
lionel-houston -
Category
Documents
-
view
220 -
download
0
Transcript of 1 Depression and management Guidelines Prof. Dr. Momtaz AbdEl Wahab Prof. of psychiatry Cairo...

1
Depression and management
Guidelines
Depression and management
Guidelines
Prof. Dr. Momtaz AbdEl Wahab
Prof. of psychiatry
Cairo University
Prof. Dr. Momtaz AbdEl Wahab
Prof. of psychiatry
Cairo University

2
Face the FactsFace the Facts
Depression is a Prevalent
Disorder
Depression is a Prevalent
Disorder

3
EpidemiologyEpidemiology

4
EpidemiologyEpidemiology
• The depression research in European society (DEPRES) study found that almost 16% of total population had suffered from depression in their life time. (lepin jp. etal 1979).
• The incidence is almost identical in USA 17%(kessler R.C.etal 1994).
• The depression research in European society (DEPRES) study found that almost 16% of total population had suffered from depression in their life time. (lepin jp. etal 1979).
• The incidence is almost identical in USA 17%(kessler R.C.etal 1994).

5
121 Million People Suffer From Depression
121 Million People Suffer From Depression
ATLAS (WHO 2001)ATLAS (WHO 2001)
Depression is a Prevalent DisorderDepression is a Prevalent Disorder

6
The Prevalence of
Depression is Rising?!
The Prevalence of
Depression is Rising?!
Face the FactsFace the Facts
7
Epidemiology (cont’d)Epidemiology (cont’d)
• The incidence of depression appears to be increasing, although this may be explained by an increasing willingness to report psychological problems.
• The incidence of depression appears to be increasing, although this may be explained by an increasing willingness to report psychological problems.

8
STRESSSTRESS
OVERLOADOVERLOAD
Anxiety
Depression
(DALYS, 2020)
Anxiety
Depression
(DALYS, 2020)
WARSWARS
Disasters
Globalization
Massive information
Techno stress
Individualization
Disasters
Globalization
Massive information
Techno stress
Individualization
EVERYDAY LIFEEVERYDAY LIFE
Lack of supportLack of support
NoisesNoises
Time pressureTime pressure
PollutionPollutionAnticipation
of dangerAnticipation
of danger
EconomicEconomic
RecessionRecession
OthersOthersSpoucesSpouces
BossBossExcessive
respondents Excessive
respondents
9
The Burden of Depression
The Burden of Depression

10
Face the FactsFace the Facts
Depression is a BurdenDepression is a Burden

11
The burden of depressionThe burden of depression
• Disability associated with depression is reportedly greater than that for chronic illnesses such as arthritis, back pain, diabetes gastrointestinal disease, hypertension and long diseases.
• Disability associated with depression is reportedly greater than that for chronic illnesses such as arthritis, back pain, diabetes gastrointestinal disease, hypertension and long diseases.

12
Leading causes of disability worldwide in years of life lived with disability
Leading causes of disability worldwide in years of life lived with disability
Cause %
Unipolor major depression 10.07
Iron deficiency anemia 4.7
Falls 4.6
Alcohol use 3.3
Chronic obstructive pulmonary disease
3.1
Bipolar disorder 3
Congenital anomalies 2.9
Osteoarthritis 2.8
Schizophrenia 2.6
13
World Bank Reports World Bank Reports
Year
2000 is the world
2020 will be the
Anxiety Depression
4th greatest health problem
2nd greatest health problem
causing disability

14
Depression in an Expensive Disorder
Depression in an Expensive Disorder
Face the FactsFace the Facts

15
The burden of depressionThe burden of depression
• The disorder tends to become recurrent or chronic with time.
• 50% of the life of depressed patients life span will be clouded by the illness.
• The depressed patient is often isolated, the dysfunction has repercussion on:
- family member - friends - colleaguesTheir relationships frequently being shattered
• The disorder tends to become recurrent or chronic with time.
• 50% of the life of depressed patients life span will be clouded by the illness.
• The depressed patient is often isolated, the dysfunction has repercussion on:
- family member - friends - colleaguesTheir relationships frequently being shattered

16
The burden of depressionThe burden of depression
• Behavioral changes are common: - increased drinking - initiation drug abuse • Unfortunately, the patients
themselves are often not aware of being clinically depressed, and thus will not actively seek help or treatment.
• Behavioral changes are common: - increased drinking - initiation drug abuse • Unfortunately, the patients
themselves are often not aware of being clinically depressed, and thus will not actively seek help or treatment.

17
The burden of depressionThe burden of depression
• Several studies has shown higher mortality risk in depressed individual:
-suicidal risk is high 15%-19%-cardiovascular deaths• Depressive symptoms seem to be
risk factors for mortality in pulmonary disorders and stroke.
• Several studies has shown higher mortality risk in depressed individual:
-suicidal risk is high 15%-19%-cardiovascular deaths• Depressive symptoms seem to be
risk factors for mortality in pulmonary disorders and stroke.

18
The burden of depressionThe burden of depression
• Depressed patient is less likely to sustain a demanding job or career or to achieve his or her potential.
• If the depression arises during the
formative years, an in evitable consequence is diminished performance at school, college, or educational training with life long consequences.
• Depressed patient is less likely to sustain a demanding job or career or to achieve his or her potential.
• If the depression arises during the
formative years, an in evitable consequence is diminished performance at school, college, or educational training with life long consequences.

19
Economic implications for society Economic implications for society
• Reduced and lost productivity - absenteeism - wasted training• The increased strain and demands
on health services.• The increased direct cost of
treatment, particularly caused by hospital admissions.
• Reduced and lost productivity - absenteeism - wasted training• The increased strain and demands
on health services.• The increased direct cost of
treatment, particularly caused by hospital admissions.

20
COSTCOST
Direct
• Recurrence
• Treatment
• Hospitalization
Direct
• Recurrence
• Treatment
• Hospitalization
Indirect
• Disability in work
• Poor social function
• Associated behavioral
problems
• Increase self destructive
behaviors
Indirect
• Disability in work
• Poor social function
• Associated behavioral
problems
• Increase self destructive
behaviors

21
Face the FactsFace the Facts
Depression is a Recurrent Disorder
Depression is a Recurrent Disorder

22
• Depression is too painful to be
ignored.
• Depression is unrecognized!!
• Depression has many faces.
• Depression is too painful to be
ignored.
• Depression is unrecognized!!
• Depression has many faces.
Face the FactsFace the Facts

23
20% of those with major depression
have symptoms that persist beyond
2 years
20% of those with major depression
have symptoms that persist beyond
2 years
Keller et al., (1992) & Scot & Dicky (2003), B. J. Psychiat.Keller et al., (1992) & Scot & Dicky (2003), B. J. Psychiat.

24
The need for treatment The need for treatment
• Depression continue to be a silent epidemic because so few people with depression receive treatment.
• 50% of depressed patients had not consulted physician.
• Of those who had 70% had been given no medication for depression.
• Less than 10% of those with major depressive disorder had been prescribed an antidepressant.
• Depression continue to be a silent epidemic because so few people with depression receive treatment.
• 50% of depressed patients had not consulted physician.
• Of those who had 70% had been given no medication for depression.
• Less than 10% of those with major depressive disorder had been prescribed an antidepressant.

25
Face the FactsDepression is an
Under-recognized Disorder
Face the FactsDepression is an
Under-recognized Disorder
Stigma.
Masked depression.
Comorbid medical illness.
Time constraints.
Inadequate medical education.
Stigma.
Masked depression.
Comorbid medical illness.
Time constraints.
Inadequate medical education.

26
The need for treatmentThe need for treatment
• In addition, when antidepressants are prescript, dosage and duration of treatment are often mostly inadequate to achieve a response or maintain remission.
• In addition, when antidepressants are prescript, dosage and duration of treatment are often mostly inadequate to achieve a response or maintain remission.
27
Reasons for under recognition/ under treatment of depression
Reasons for under recognition/ under treatment of depression
Provider • Inadequate training. • Depression not a real disorder
(preoccupied with organicity ).• Time- consuming to evaluate (failure to
elicit symptoms).• Restricted access to treatment options.• Failure to refer from G.P. when indicated.
Provider • Inadequate training. • Depression not a real disorder
(preoccupied with organicity ).• Time- consuming to evaluate (failure to
elicit symptoms).• Restricted access to treatment options.• Failure to refer from G.P. when indicated.

28
Patient
• Stigma.
• Ignorance.
• Effect of the symptoms.
• Poor compliance.
• Poor insurance coverage.
• Presentation: somatization.
Patient
• Stigma.
• Ignorance.
• Effect of the symptoms.
• Poor compliance.
• Poor insurance coverage.
• Presentation: somatization.
Reasons for under recognition/ under treatment of depression
Reasons for under recognition/ under treatment of depression

29
Why is it important to recognize depression?
Why is it important to recognize depression?
• High costs.
• Suicide and other mortality.
• Risk factor for co morbidity.
• Very treatable.
• High costs.
• Suicide and other mortality.
• Risk factor for co morbidity.
• Very treatable.

30
Diagnosis and SymptomsDiagnosis and Symptoms

31
Depressive symptoms Background
Somatic symptoms Foreground
Depressive symptoms Background
Somatic symptoms Foreground
Many Faces of DepressionMany Faces of Depression

32
Depression is recorded in up to 30% of patients seen by other specialties
• Oncology• Dermatology• GIT• CNS• C.V.S.• Others
Depression is recorded in up to 30% of patients seen by other specialties
• Oncology• Dermatology• GIT• CNS• C.V.S.• Others
Face the FactsFace the Facts
33
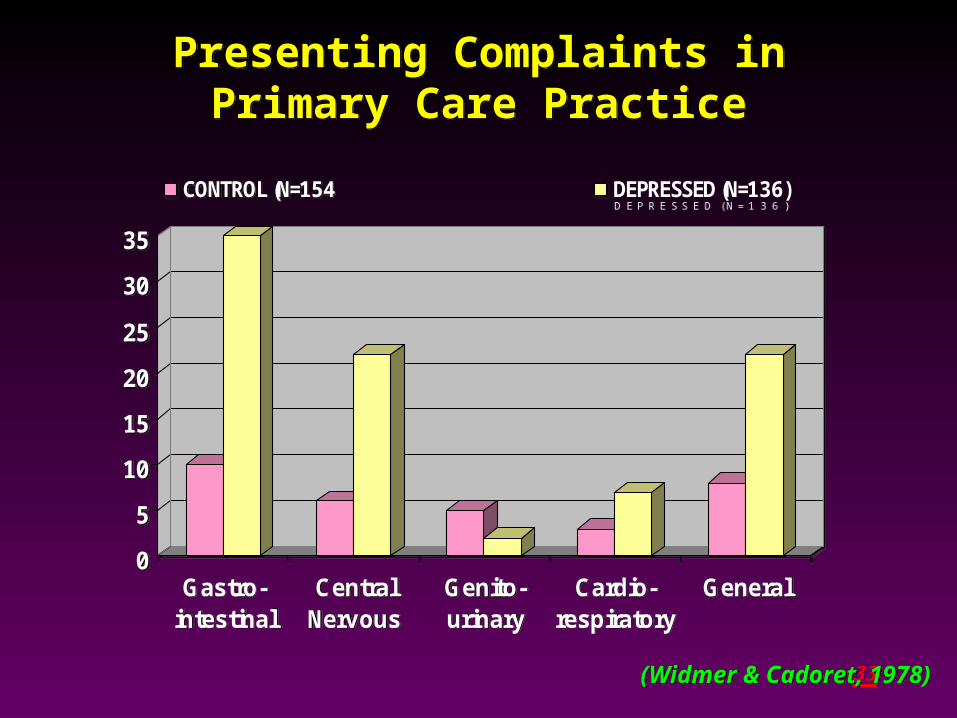
Presenting Complaints inPrimary Care Practice
Presenting Complaints inPrimary Care Practice
0
5
10
15
20
25
30
35
Gastro-intestinal
CentralNervous
Genito-urinary
Cardio-respiratory
General
CONTROL (N=1 5 4 DEPRESSED (N=1 3 6 )
0
5
10
15
20
25
30
35
Gastro-intestinal
CentralNervous
Genito-urinary
Cardio-respiratory
General
CONTROL (N=1 5 4 DEPRESSED (N=1 3 6 )
(Widmer & Cadoret, 1978)(Widmer & Cadoret, 1978)

34
Depression in Primary CareDepression in Primary Care
52%
48%
Not recognized Recognized
52%
48%
Not recognized Recognized

35
“ICEBERG” PHENOMENON“ICEBERG” PHENOMENON
Depressed patients seen by
psychiatrists
Depressed patients seen by
psychiatrists
Depressed patients seen in primary care
practice
Depressed patients seen in primary care
practice
Okasha, 2003Okasha, 2003

36
Many Faces of DepressionMany Faces of Depression
Why there is a Tendency for
depression to manifest itself in the
somatization sphere
Why there is a Tendency for
depression to manifest itself in the
somatization sphere

37
Only about ½ of patients with MD are explicitly
recognized as being depressed.
Only about ½ of all depressed patients
receive some form of therapy for their illness (Lepine et al 1997)
Only about ¼ of depressed patient receive an
adequate dose and duration of AD treatment
(Katon et al 1992)
Only about ½ of patients with MD are explicitly
recognized as being depressed.
Only about ½ of all depressed patients
receive some form of therapy for their illness (Lepine et al 1997)
Only about ¼ of depressed patient receive an
adequate dose and duration of AD treatment
(Katon et al 1992)

38
• The understanding of the underlying
neurobiology and neurochemical dysfunction
in depression is an essential issue for the
proper management
• The understanding of the underlying
neurobiology and neurochemical dysfunction
in depression is an essential issue for the
proper management

39
Neuro circuittary
Immunesystem
Neurotransmitters5HT, NE, DA
Others
Circadian rhythm
Neurohormones
Neuropeptides
HPAAxis
Dysfunctionin
Neuobiology of DepressionNeuobiology of Depression
Khalia M (2005): Metabolism Clinical & experimental54 Suppl(1).; 24-27Khalia M (2005): Metabolism Clinical & experimental54 Suppl(1).; 24-27

40
Neuro circuits
Neurotransmitters5HT, NE, DA
Dysfunctionin
Linking Neurotransmitters and neurocirciuts with Symptoms of Depression
Linking Neurotransmitters and neurocirciuts with Symptoms of Depression

41
Neuroanatomical & Neurochemical Basis of Symptoms of Depression
Neuroanatomical & Neurochemical Basis of Symptoms of Depression
EMOTIONAL SOMATIC COGNITIVE
Loss of pleasure, interest &
motivation
Sadness & suicide
Fatigue loss of energy
Sleep
appetite
Libido
etc.
Attention
Concentration
Problem solving
Dorso-lateral
PFC
Ventro-medial
PFC
DA
NE
5HT
Nucleus accumbens & hypothalamus
Dorso-lateral
PFC
DA 5HT
NE
DA
5HT
NE
DA
DA (D1)
Ach.
5HT
NE
GABA
Histamine
Malhi GS, et al., (2005): Acta Psychiatr. Scand.; 111:94-105Malhi GS, et al., (2005): Acta Psychiatr. Scand.; 111:94-105

42
Functional Roles of Brain Monoamines
Norepinephrine Serotonin
Dopamine
AnxietyIrritability
Mood,Emotion,Cognitive function
Sex & appetite Aggression
EnergyInterestSocial functionMemory
MotivationAttention
ImpulseControl
DriveRewardExecutive function
Modified from Healy & McMonagle. J Psychopharmacol 1997; 11 (suppl 4): S25-S31.
43
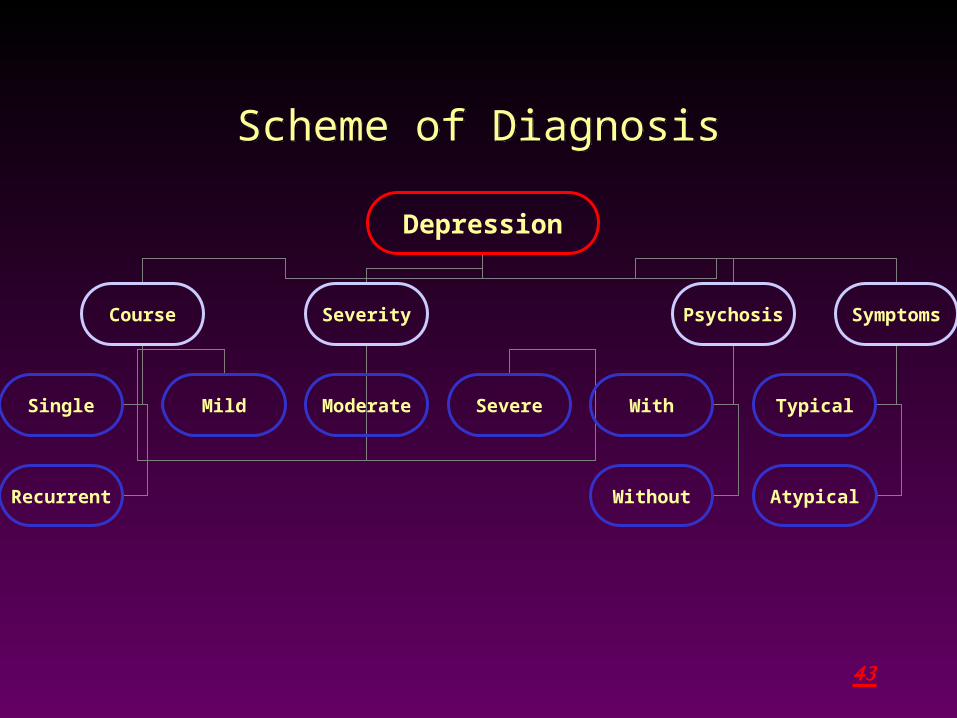
Scheme of DiagnosisScheme of Diagnosis
Depression
Course Severity Psychosis Symptoms
Single
Recurrent
With
Without
Mild Moderate Severe Typical
Atypical
44
SymptomsSymptoms
Pattern of Symptoms:
• Typical.
• Atypical.
• With melancholic.
Pattern of Symptoms:
• Typical.
• Atypical.
• With melancholic.

45
Diagnostic Process Diagnostic Process
1) Common Presentations
Usually the patient presents either of the
following symptoms:
1- Multiple Somatic complaints.
2- Lack of Concentration and/or forgetfullness.
3- Increased fatigability.
1) Common Presentations
Usually the patient presents either of the
following symptoms:
1- Multiple Somatic complaints.
2- Lack of Concentration and/or forgetfullness.
3- Increased fatigability.

46
2) Signs suggesting a depressive disorder:2) Signs suggesting a depressive disorder:
1. The patient has multiple and excessive complaints,
involving more than one system in the body.
2. The complaints are vague and ill defined and
cannot be categorized as one identifiably disease.
3. The patient is easily predictable, giving yes as an
answer to any question.
4. On physical examination, there are not enough
signs to explain the symptoms described by the
patient.
5. Results of investigations are always within the
normal ranges.

47
3) Diagnostic Criteria3) Diagnostic Criteria
A. At least one on the following symptoms has to
prevail for at least two weeks.
1- Depressed mood for most of the day and
almost every day.
2- loss of interest or pleasure in doing the
activities that were normally pleasurable.

48
B) At least four of the following symptoms:1- change in appetite.
2- Sleep Disturbance.
3- Psychomotor disturbance.
4- Increased fatigability or loss of energy.
5- Feeling of worthlessness as well as
excessive inappropriate guilt.
6- Diminished ability to think and concentrate.
7- a state of indecisiveness.
8- Recurrent thoughts of death.
9- Pessimistic views of the future.

49
C) The symptoms lead to significant distress or
impairment in social, occupational or other
important functional areas.

50
Atypical symptoms include: Atypical symptoms include:
1-vegetative symptoms of reserved polarity as:-
-hypersomnia
-increased appetite
-weight gain.
2-marked mood reactivity.
3-sensitivity to emotional rejection.
1-vegetative symptoms of reserved polarity as:-
-hypersomnia
-increased appetite
-weight gain.
2-marked mood reactivity.
3-sensitivity to emotional rejection.

51
severityseverity
1. Mild episode characterized by:• Minimum diagnostic requirements• Minor function impairment 2. Moderate episode• The symptoms present exceed the
bare diagnostic requirements • Greater degrees of functional
impairment
1. Mild episode characterized by:• Minimum diagnostic requirements• Minor function impairment 2. Moderate episode• The symptoms present exceed the
bare diagnostic requirements • Greater degrees of functional
impairment

52
Severe EpisodeSevere Episode
• Presence of several symptoms beyond the minimum required to make diagnoses.
• Marked interference with social and/or occupational functioning.
• Presence of several symptoms beyond the minimum required to make diagnoses.
• Marked interference with social and/or occupational functioning.

53
Severe EpisodeSevere Episode
In extreme cases,individuals might be
unavailable to function socially, occupationally,
un-able to feed and clothe themselves, or to
maintain minimal personal hygiene.
•Presence of suicidal ideation and attempt.
•Presence of psychotic symptoms.
•Presence of catatonic symptoms.
•Presence melancholic symptoms.
In extreme cases,individuals might be
unavailable to function socially, occupationally,
un-able to feed and clothe themselves, or to
maintain minimal personal hygiene.
•Presence of suicidal ideation and attempt.
•Presence of psychotic symptoms.
•Presence of catatonic symptoms.
•Presence melancholic symptoms.

54
Psychosis Psychosis
• Psychosis is considered when there is:
1. Delusions
2. Hallucinations
3. Catatonic symptoms
• Psychosis is considered when there is:
1. Delusions
2. Hallucinations
3. Catatonic symptoms

55
Catatonic symptomsCatatonic symptoms
Characterized by at least two of the following:
1. Motor immobility (catalepsy or stupor)
2. Extreme agitation
3. Extreme negativism
4. Posturing
5. Stereotyped movements, mannerisms or grimacing
6. Echolalia or echopraxia
Characterized by at least two of the following:
1. Motor immobility (catalepsy or stupor)
2. Extreme agitation
3. Extreme negativism
4. Posturing
5. Stereotyped movements, mannerisms or grimacing
6. Echolalia or echopraxia

56
Melancholic SymptomsMelancholic Symptoms1- Loss of pleasure in all, or almost all activities.
2-Lack of reactivity to pleasurable stimuli (anhedonia).
3- Distinct quality of depressed mood.
4- Diurnal variation (depression regularly worse in the morning).
1- Loss of pleasure in all, or almost all activities.
2-Lack of reactivity to pleasurable stimuli (anhedonia).
3- Distinct quality of depressed mood.
4- Diurnal variation (depression regularly worse in the morning).

57
Melancholic SymptomsMelancholic Symptoms
5-Early morning awakening.
6- Marked psychomotor retardation or agitation.
7- Significant anorexia or weight loss.
8- Excessive or inappropriate guilt.
5-Early morning awakening.
6- Marked psychomotor retardation or agitation.
7- Significant anorexia or weight loss.
8- Excessive or inappropriate guilt.

58
• Dysthymia
• Postpartum depression
• Recurrent brief depression
• Mixed anxiety-depression syndrome
• Sub-threshold depression
• Premenstrual Dysphoric Disorder
• Post menopausal Depression
• Dysthymia
• Postpartum depression
• Recurrent brief depression
• Mixed anxiety-depression syndrome
• Sub-threshold depression
• Premenstrual Dysphoric Disorder
• Post menopausal Depression
OTHER FORMS OF DEPRESSIVE DISORDERS
OTHER FORMS OF DEPRESSIVE DISORDERS

59
• Psychotic depression
• Somatic depression
• Atypical depression
• Psychotic depression
• Somatic depression
• Atypical depression
SPECIAL FORMS OF DEPRESSIVE DISORDERS
SPECIAL FORMS OF DEPRESSIVE DISORDERS

60
• Seasonal depressive disorder.
• Rapid-cycling bipolar disorder,
depressive episode.
• Secondary depressive disorder.
• Seasonal depressive disorder.
• Rapid-cycling bipolar disorder,
depressive episode.
• Secondary depressive disorder.
SPECIAL FORMS OF DEPRESSIVE DISORDERS (cont’d)
SPECIAL FORMS OF DEPRESSIVE DISORDERS (cont’d)
61
Depression Due to a General Medical Conditions
Depression Due to a General Medical Conditions
1- Depression due to general medical condition
Endocrine disorders (D.M., hypothyroidism, Cushing's disease).
Diseases of CNS, CVS, chest disease.
Collagen disease ( Rheumatoid arthritis, SLE)
Chronic infections ( hepatitis, T.B.)
Neurological diseases ( Parkinsonism, CVS)
Neoplasm( cancer lung, cancer GIT).
2- Depression secondary to other nonpsycho-active drugs (steroids, & reserpine).
1- Depression due to general medical condition
Endocrine disorders (D.M., hypothyroidism, Cushing's disease).
Diseases of CNS, CVS, chest disease.
Collagen disease ( Rheumatoid arthritis, SLE)
Chronic infections ( hepatitis, T.B.)
Neurological diseases ( Parkinsonism, CVS)
Neoplasm( cancer lung, cancer GIT).
2- Depression secondary to other nonpsycho-active drugs (steroids, & reserpine).

62
Prevalence
*There is a range of percentages depending on the study.
Prevalence
*There is a range of percentages depending on the study.
39 % 45 % 47 % 42 % 33 % 36 % 33 %
9 %6 %
0%5%
10%15%20%25%30%35%40%45%50%
Prevalence of Depressive Disorders
In Different Patient Populations*

63
Play a role in:
Exacerbation.
Delayed recovery.
Prolonged course.
Poor outcome.
Prolonged
Hospitalization.
Play a role in:
Exacerbation.
Delayed recovery.
Prolonged course.
Poor outcome.
Prolonged
Hospitalization.
Depression Adversely Affects Medical Diseases
Depression Adversely Affects Medical Diseases

64
MYTH
Depression is obvious
and easily recognized and expressed by the
patient
MYTH
Depression is obvious
and easily recognized and expressed by the
patient
REALITY
Depression disorders are
overlapping, hardly expressed by the
patient and constitute a major
problem in symptom exaggeration
REALITY
Depression disorders are
overlapping, hardly expressed by the
patient and constitute a major
problem in symptom exaggeration
65
MYTH
Depression is Secondary to GMD
activityTreatment of the medical
disorder will relief Depression.
MYTH
Depression is Secondary to GMD
activityTreatment of the medical
disorder will relief Depression.
REALITY
DEPRESSION DEPRESSION REQUIRES TREATMENT intervention and do not
remit with relieve of symptoms
REALITY
DEPRESSION DEPRESSION REQUIRES TREATMENT intervention and do not
remit with relieve of symptoms

66
DIAGNOSIS: THE CLINICAL INTERVIEW
DIAGNOSIS: THE CLINICAL INTERVIEW
• Listen• Facilitate
– “Go on.”– “What else?”
• Demonstrate concern• Summarize
• Listen• Facilitate
– “Go on.”– “What else?”
• Demonstrate concern• Summarize• Try to put the patient at ease• Begin with open-ended questions• Probe for symptoms, e.g.
– “Any trouble with your nerves?”– “How have you been sleeping?”– “What do you do to enjoy yourself?”
• Try to put the patient at ease• Begin with open-ended questions• Probe for symptoms, e.g.
– “Any trouble with your nerves?”– “How have you been sleeping?”– “What do you do to enjoy yourself?”

67
MINI INTERNATIONAL NEUROPSYCHIATRIC INTERVIEW
• The MINI is a brief structured interview for the major Axis I psychiatric diorders in DSM-IV & ICD-10.
• Compared to the SCID-P (structured interview developed by the WHO ), the MINI has acceptably high validation and reliability scores, but can be administered in a much shorter time.
MINI INTERNATIONAL NEUROPSYCHIATRIC INTERVIEW
• The MINI is a brief structured interview for the major Axis I psychiatric diorders in DSM-IV & ICD-10.
• Compared to the SCID-P (structured interview developed by the WHO ), the MINI has acceptably high validation and reliability scores, but can be administered in a much shorter time.
MM II NN II
68
Depressed mood or loss of feeling? Depressed mood or loss of feeling?
النفسية هل هل • حالتك أن أو باألكتئاب النفسية أحسست حالتك أن أو باألكتئاب أحسست
متكررة بصورة و اليوم أوقات معظم فى متكررة سيئة بصورة و اليوم أوقات معظم فى سيئة
الماضيين األسبوعين الماضيين خالل األسبوعين ؟؟خالل
األسبوعين • األسبوعين خالل اهتماما خالل أقل كنت هل اهتماما الماضيين أقل كنت هل الماضيين
بها تتمتع كنت التى باألشياء استمتاعا أقل بها أو تتمتع كنت التى باألشياء استمتاعا أقل أو
الوقت الوقت أغلب ؟ ؟ أغلب
النفسية هل هل • حالتك أن أو باألكتئاب النفسية أحسست حالتك أن أو باألكتئاب أحسست
متكررة بصورة و اليوم أوقات معظم فى متكررة سيئة بصورة و اليوم أوقات معظم فى سيئة
الماضيين األسبوعين الماضيين خالل األسبوعين ؟؟خالل
األسبوعين • األسبوعين خالل اهتماما خالل أقل كنت هل اهتماما الماضيين أقل كنت هل الماضيين
بها تتمتع كنت التى باألشياء استمتاعا أقل بها أو تتمتع كنت التى باألشياء استمتاعا أقل أو
الوقت الوقت أغلب ؟ ؟ أغلب

69
Markedly diminished interest or pleasure or enjoyment or anhedonia? Markedly diminished interest or pleasure or enjoyment or anhedonia?
حاجة 1. أى في نفس ملكش إن حسيت عمرك هل
كده قبل كنت حلو شيء بأي تتمتع قادر أومش
به قر( بـتتمتع ، التلفزيون على الفرجة ة اءمثال
أو ، بتمارسها كنت هواية أو حد، زيارة أو الجريدة
( حلوة أكلة حتى أو ، األصحاب مع الخروج
فى 2. تقريبا اليوم معظم االحساس هذا استمر هل
أسبوعين عن تقل ال ولمدة األسبوع أيام معظم
كاملين؟
حاجة 1. أى في نفس ملكش إن حسيت عمرك هل
كده قبل كنت حلو شيء بأي تتمتع قادر أومش
به قر( بـتتمتع ، التلفزيون على الفرجة ة اءمثال
أو ، بتمارسها كنت هواية أو حد، زيارة أو الجريدة
( حلوة أكلة حتى أو ، األصحاب مع الخروج
فى 2. تقريبا اليوم معظم االحساس هذا استمر هل
أسبوعين عن تقل ال ولمدة األسبوع أيام معظم
كاملين؟

70
من أى على األجابة كانت اذا “ فى ” استمر بنعم السؤالين: التالية األسئلة على االجابة
أو. 3 مكتئب أنك شعرت عندماخالل حزين أو مهموم: الماضيين األسبوعين
من أى على األجابة كانت اذا “ فى ” استمر بنعم السؤالين: التالية األسئلة على االجابة
أو. 3 مكتئب أنك شعرت عندماخالل حزين أو مهموم: الماضيين األسبوعين

71
Weight loss – gain; decreased / increased appetite? Weight loss – gain; decreased / increased appetite?
زاد • أو جامد خسيت إنك الحظت هل
ملحوظة؟ زيادة وزنك
أو • زادت لألكل شهيتك أن الحظت هل
ذلك كان و الطبيعي عن نقصت
أيام معظم تقريبا اليوم لمعظم
.األسبوع
زاد • أو جامد خسيت إنك الحظت هل
ملحوظة؟ زيادة وزنك
أو • زادت لألكل شهيتك أن الحظت هل
ذلك كان و الطبيعي عن نقصت
أيام معظم تقريبا اليوم لمعظم
.األسبوع
3) أ.)

72
Insomnia or hypersomnia, sleep disturbances? Insomnia or hypersomnia, sleep disturbances?
النوم • في صعوبة هناك أن الحظت هل
كذا( تصحى أو النوم إلي الدخول في صعوبة
( ؟ الطبيعي عن قوي بدري تقوم أو بالليل مرة
الطبيعي • من بكثير أكثر بتنام أنك الحظت هل
الفترة؟ هذه خالل في األيام معظم بتاعك
النوم • في صعوبة هناك أن الحظت هل
كذا( تصحى أو النوم إلي الدخول في صعوبة
( ؟ الطبيعي عن قوي بدري تقوم أو بالليل مرة
الطبيعي • من بكثير أكثر بتنام أنك الحظت هل
الفترة؟ هذه خالل في األيام معظم بتاعك
3) ب.)

73
Psychomotor agitation or retardation Psychomotor agitation or retardation
قادر • ومش متململ انك الحظت هل
في األيام معظم واحد مكان في تقعد
الفترة؟ هذه
الحركة • في بطئ عندك ان الحظت هل
الفترة؟ هذه في األيام معظم الكالم و
قادر • ومش متململ انك الحظت هل
في األيام معظم واحد مكان في تقعد
الفترة؟ هذه
الحركة • في بطئ عندك ان الحظت هل
الفترة؟ هذه في األيام معظم الكالم و
3) ج.)

74
Fatigue or loss of energy Fatigue or loss of energy
على • وتعبان مرهق أنك حسيت هل
حاجة أى عمل على قادر مش و طول
معظم حيوية وال طاقة وماعندكش
الفترة؟ هذه في األيام
على • وتعبان مرهق أنك حسيت هل
حاجة أى عمل على قادر مش و طول
معظم حيوية وال طاقة وماعندكش
الفترة؟ هذه في األيام
3) د.)

75
Feeling of worthlessness or excessive or inappropriate guilt, self blame and reproach, Feeling of worthlessness or excessive or inappropriate guilt, self blame and reproach,
روحك • إن داخلي إحساس بيجيلك كان هلوانك الناس من أقل انك أو منخفضة المعنوية
الفترة هذه في األيام معظم في قيمة ؟مالكش
تأنيب • و بالذنب داخلي إحساس بيجيلك كان هل
في األيام معظم في واضح سبب بدون الضمير
الفترة؟ هذه
انت • حاجات على نفسك تلوم إنك بتميل هل
فيها؟ فكرت أو عملتها
روحك • إن داخلي إحساس بيجيلك كان هلوانك الناس من أقل انك أو منخفضة المعنوية
الفترة هذه في األيام معظم في قيمة ؟مالكش
تأنيب • و بالذنب داخلي إحساس بيجيلك كان هل
في األيام معظم في واضح سبب بدون الضمير
الفترة؟ هذه
انت • حاجات على نفسك تلوم إنك بتميل هل
فيها؟ فكرت أو عملتها
3) ه.)
76
Diminished ability to think and concentrate, indecisiveness Diminished ability to think and concentrate, indecisiveness
قادر • غير الفترة هذه في كنت هل
أنك أو بوضوح والتفكير التركيز على
التردد؟ كثير
قادر • غير الفترة هذه في كنت هل
أنك أو بوضوح والتفكير التركيز على
التردد؟ كثير
3) و.)

77
Thoughts of death, catastrophe, suicidal ideation, attempt, plan or self harm Thoughts of death, catastrophe, suicidal ideation, attempt, plan or self harm
يعيش • الواحد تستهلش ما الحياة أن حسيت هلتصحاش ما انك معاك حايفرق مش أنه أو فيها
الصبح؟ يوم تانى
بأي • نفسك تؤذى أن الفترة هذه في فكرت هل؟ طريقة
الموت • في كثير بتفكر الفترة هذه في كنت هل؟ االنتحار عن أفكار بيجيلك أو تتمناه أو
ممكن • مصايب فى تفكر تقعد انك ميال أنت هلكارثة؟ أي أو البيوت خراب أو الموت زى تحصل
يعيش • الواحد تستهلش ما الحياة أن حسيت هلتصحاش ما انك معاك حايفرق مش أنه أو فيها
الصبح؟ يوم تانى
بأي • نفسك تؤذى أن الفترة هذه في فكرت هل؟ طريقة
الموت • في كثير بتفكر الفترة هذه في كنت هل؟ االنتحار عن أفكار بيجيلك أو تتمناه أو
ممكن • مصايب فى تفكر تقعد انك ميال أنت هلكارثة؟ أي أو البيوت خراب أو الموت زى تحصل
3) ز.)

78
Diagnosis:Diagnosis:
على حصلت “ 5اذا بنعم ” أكثر أو اجاباتمن األسئلة الى. 3على ز.3أ
من يعانى فالمريض اذا
حالية اكتئاب نوبة
على حصلت “ 5اذا بنعم ” أكثر أو اجاباتمن األسئلة الى. 3على ز.3أ
من يعانى فالمريض اذا
حالية اكتئاب نوبة
Current Depressive EpisodeCurrent Depressive Episode

79
Check for Recurrent EpisodesCheck for Recurrent Episodes
4 ( هل. ( الماضية حياتك سنوات خالل أأو ( أسبوعين مدتها أخرى بفترات مررت
أنك) أو باالكتئاب خاللها أحسست أكثرخاللها عانيت أو األشياء بمعظم مهتم غير
ذكرها؟ السالف األعراض بنفس4 ( عن.( تقل ال مدة عليك مرت هل ب
بعدم احساس أو اكتئاب بدون شهريننوبتين بين ما فترة فى االهتمام
لالكتئاب؟
4 ( هل. ( الماضية حياتك سنوات خالل أأو ( أسبوعين مدتها أخرى بفترات مررت
أنك) أو باالكتئاب خاللها أحسست أكثرخاللها عانيت أو األشياء بمعظم مهتم غير
ذكرها؟ السالف األعراض بنفس4 ( عن.( تقل ال مدة عليك مرت هل ب
بعدم احساس أو اكتئاب بدون شهريننوبتين بين ما فترة فى االهتمام
متكررة لالكتئاب؟ اكتئاب متكررة نوبة اكتئاب نوبة

80
Not due to a substance or a general medical condition Not due to a substance or a general medical condition
أو • مرض بأي مريض كنت األعراض هذه قبل هل
تانيين؟ دكاترة على اتعرضت
هل أخذت أي أدوية أو عالجات قبل هذه •
األعراض ؟
هل قبل هذه األعراض أخذت مكيفات أو كحوليات؟•
أو • مرض بأي مريض كنت األعراض هذه قبل هل
تانيين؟ دكاترة على اتعرضت
هل أخذت أي أدوية أو عالجات قبل هذه •
األعراض ؟
هل قبل هذه األعراض أخذت مكيفات أو كحوليات؟•
QuestionsQuestions
1- The DSM-IV classification of mood disorders encompasses all of the following except1. Bipolar disorders
2. Dysthymia
3. Posttraumatic stress disorder
4. Cyclothemia
5. Major depression
1- The DSM-IV classification of mood disorders encompasses all of the following except1. Bipolar disorders
2. Dysthymia
3. Posttraumatic stress disorder
4. Cyclothemia
5. Major depression
2- which of the following statements is true of dysthymic disorders?1. Symptoms less intense and invasive than
major depression.
2. Symptoms have both characteristics of both depressive and manic syndromes.
3. Hypomanic features must be of at least two years duration.
4. It’s a variety of bipolar disorder.
5. None of the above is true.
2- which of the following statements is true of dysthymic disorders?1. Symptoms less intense and invasive than
major depression.
2. Symptoms have both characteristics of both depressive and manic syndromes.
3. Hypomanic features must be of at least two years duration.
4. It’s a variety of bipolar disorder.
5. None of the above is true.

3- Which of the following statements isn’t true of bipolar disorders?1. It occurs in 0.4% to 1.2% of the adult population
2. It has a familial pattern associated with it
3. The first episode usually occurs between 20 & 40 years of age
4. Depression occurs more frequently than mania
5. Forty percent of patient with typical bipolar disorder respond to lithium.
3- Which of the following statements isn’t true of bipolar disorders?1. It occurs in 0.4% to 1.2% of the adult population
2. It has a familial pattern associated with it
3. The first episode usually occurs between 20 & 40 years of age
4. Depression occurs more frequently than mania
5. Forty percent of patient with typical bipolar disorder respond to lithium.

4- The concept of uncomplicated bereavement includes all of the following except1. It isn’t a mental disorder under DSM-IV
2. It isn’t categorized as a major depressive episode under DSM-IV
3. It’s a normal reaction
4. It’s of varied duration among different cultural groups
5. It’s an exacerbation of a previous mental disorder
4- The concept of uncomplicated bereavement includes all of the following except1. It isn’t a mental disorder under DSM-IV
2. It isn’t categorized as a major depressive episode under DSM-IV
3. It’s a normal reaction
4. It’s of varied duration among different cultural groups
5. It’s an exacerbation of a previous mental disorder

5- All of the following are characteristics of melancholia except1. Loss of interest or pleasure in all or
almost all activities.
2. Lack of reactivity to pleasure stimuli
3. Depression regularly worse in morning
4. Endogenous origin
5. Consistent early morning awakening
5- All of the following are characteristics of melancholia except1. Loss of interest or pleasure in all or
almost all activities.
2. Lack of reactivity to pleasure stimuli
3. Depression regularly worse in morning
4. Endogenous origin
5. Consistent early morning awakening

6- an individual whose symptomatology fulfills the criteria for dysthymic disorder , but who have intermittent periods of normal mood which last more than a few months is BEST classified as having 1. Depressive disorder, otherwise not classified.
2. Dysthymic disorder
3. Cyclothemic disorder
4. Major depressive disorder
5. None of the above
6- an individual whose symptomatology fulfills the criteria for dysthymic disorder , but who have intermittent periods of normal mood which last more than a few months is BEST classified as having 1. Depressive disorder, otherwise not classified.
2. Dysthymic disorder
3. Cyclothemic disorder
4. Major depressive disorder
5. None of the above

7- All of the following are symptoms of a major depression except :1. disorientation to time .
2. Delusions involving concern of AIDS.
3. Failure to care to personnel hygiene.
4. Overemphasis on the bad things of life.
5. Thought blocking .
7- All of the following are symptoms of a major depression except :1. disorientation to time .
2. Delusions involving concern of AIDS.
3. Failure to care to personnel hygiene.
4. Overemphasis on the bad things of life.
5. Thought blocking .
8- The following statements are true regarding atypical depression.
1. Increase in food intake and sleeping is common.
2. Mood is unreactive.
3. Personality issues are prominent.
4. Delusions are systematized.
8- The following statements are true regarding atypical depression.
1. Increase in food intake and sleeping is common.
2. Mood is unreactive.
3. Personality issues are prominent.
4. Delusions are systematized.

9- sleep disturbance in depression.1. Is most typically early awaking.
2. Not important sign.
3. Nightmare aren’t common.
4. Sleep is refreshing.
9- sleep disturbance in depression.1. Is most typically early awaking.
2. Not important sign.
3. Nightmare aren’t common.
4. Sleep is refreshing.

10- treatment with SSRIs :1. Not associated with sleep disturbance.
2. Not associated with nausea and vomiting.
3. Can result in orgasmic impotence.
4. Complicated dosing regimen.
10- treatment with SSRIs :1. Not associated with sleep disturbance.
2. Not associated with nausea and vomiting.
3. Can result in orgasmic impotence.
4. Complicated dosing regimen.