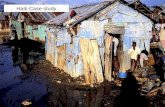
1 Crisis or Opportunity? Alcon Sponsored Haiti Ophthalmology Symposia Karibe Hotel, May 18 th - 19...
36
1 Crisis or Opportunity? Alcon Sponsored Haiti Ophthalmology Symposia Karibe Hotel, May 18 th - 19 th , 2012 Port au Prince, Haiti John Barrows, IEF Raheem Rahmathullah, IEF
-
Upload
sibyl-warner -
Category
Documents
-
view
221 -
download
2
Transcript of 1 Crisis or Opportunity? Alcon Sponsored Haiti Ophthalmology Symposia Karibe Hotel, May 18 th - 19...

1
Crisis or Opportunity?
Alcon Sponsored
Haiti Ophthalmology Symposia Karibe Hotel, May 18th - 19th, 2012
Port au Prince, Haiti
John Barrows, IEFRaheem Rahmathullah, IEF

2
Situation Before and After
Incidence 10,000
Prevalence & backlog
50,000
3,500
(2005)
• Number of blind growing– CSR is - 400 per million?– 50% of blind in
Caribbean • Services divided by private,
government, NGO, missions, Cubans
• Quality, productivity, efficiency, do we have data
• Dependence on external
resources

3
Problems Different Than Before?• Why don't people use our services?• Can we be more productive?• Why is there a brain drain?• Why do costs escalate?• Why is equipment poorly maintained?• Do we rely too much on external resources?• What are the opportunities and options we
need to know about to make positive change?• How can we get consensus to move ahead?

4
Objectives• Review principles of sustainable eye care• Provide a model to consider, inspire a vision, challenge
you about processes, enable you to take action• Self reflection on
– what are the (+) things that can happen if action is taken
– what would make it easier to take action– who will approve and support these actions
• What we are/ would like to do in Haiti• Gain honest feedback and learn from you• Relax and listen; note questions/ thoughts on handout

5
Which Way?
When you get to the fork in the road – take it.

6
Redefine the Problem
"A stable but inherently unjust equilibrium exist in eye care in developing countries causing exclusion marginalization and suffering of both patients with eye disease and eye care providers who lack the authority, autonomy, resources or political will to change the situation. Patient choices include an unaffordable private sector or an inherently inefficient public system."
"Transforming Eye Clinics and Hospitals to Sustainability – The International Eye Foundation's Social Enterprise Model" European Ophthalmic Review, 2008

7
ProblemPrivate Eye Hospitals
• Few patients at high cost• Private practitioners volunteer in charity
services• Are not willing to treat the poor within
their private practice.
You mean I’m going to start treating patients for FREE?

8
Problem Government Eye Hospitals
• Dependent on limited budgets and donor funds
• Inefficient, unproductive, not patient-focused• Lack incentives to improve services
You mean I’m going to start charging POOR people?

9
Social Enterprise SolutionCombine the best of clinical eye care practices w/ business planning & management systems to create a different approach to eye care delivery
• Public/government AND private eye hospitals choose to have a private side for paying patients and a social side for poor patients offering the same quality of clinical care.– Private clinics see paying patients and subsidize
poor patients.– Public hospitals have special facilities for private
patients and treat poor patients as well.• Patients choose where they access quality services.• Clinics achieve financial sustainability by offering a
range of services, and amenities at multi-tiered pricing including “zero cost”.

10
What Are We Trying to Achieve?
Investment in the eye hospital/clinic’s
• Ability to grow, continue meeting the needs of patients, and accept doing this beyond donor funding (traditional charitable investments).
• Services that produce benefits valued by patients and stakeholders ensuring continued demand for services for long-term.

11
Governance & Leadership
Financial Resources
Management
Service DeliveryTargets population, Building,
Comprehensive services,Equipment, Procedures,
Quality standards,Community Outreach
Dimensions and Components
Human Resources
LocationPopulationStakeholders Policies

12
Leadership
“Leading is enabling others to face challenges and achieve results in complex conditions”
Sandra Dratler DrPh, SEVA and UC, Berkley, School of Public Health
FROM… TO…
Individual heroics Collaborative actions
Despair and cynicism Hope and possibility
Blaming others for problems Taking responsibility for challenges
Scattered, disconnected activities Purposeful, interconnected actions
Self absorption Generosity and concern for common good
Governance & Leadership

13
Leadership
Personal Values• Integrity/ commitment• Respect/ trust• Courage to take
calculated risk• Openness to learning
Leadership in practice• Model way• Inspire shared vision• Challenge process• Enable others to act• Encourage the heart
Sandra Dratler DrPh, SEVA and UC, Berkley, School of Public Health

14
Attractive and Functional Space
• Patients want an attractive, convenient, clean, safe place– Would you want to go there? – Build, rent and renovate or
expand. – Efficient space to create patient
flow? (OPD)– Can you reconfigure/ renovate
space to grow?
• Operating theatre a must…– Equipped and safe

15
Appropriate Equipment & Supplies
• Careful selection of technology reduces cost
• Microscope + 2 tables• Cataract sets (4-5 per
surgeon)• Supplies (simplify, bulk
buy to avoid stock outs)
Factor Increase in productivity
% of eye units with
these factors in
place
2+ cataract surgical sets
2.65 X 46%
Operating microscope
2.44 X 78%
Community outreach program
2.13 X 20%
3+ support from nurses
2.00 X 33%
Source: Study by Kilimanjaro Centre for Community Ophthalmology for Sight Savers International

16
Quality Service for Everyone
Patients want:• Quality and choice drives services and attracts
patients• Convenient
– Scheduling, waiting time, return visits, family members, amenities, information, reputation
• Differentiate services using multi-tiered pricing – Private - service, value, cost, price above cost– Social - service, value, cost, price at cost– Free - service, value, cost, price below cost– Package to reduce confusion and inconvenience

17
Economic Distribution & Targets
• Modify for Haiti• Target middle 70%• Nobody turned away
Very rich 10%
Upper middle 10%
Middle 10%
Lower middle
30%Lower middle
Lower middle
Poor20%
Poor
Very poor20%
Very poor
70%
private
public

18
Understand Patient Population
• Realistic catchment area – Epidemiology/ gender/ age– Competition
• Characteristics of population and patients– Household income of lowest 60% population
• Behavior detriments– External/environmental detriments - distance,
knowledge, – Internal detriments - behaviors - why some
accept and others do not accept services
LocationPopulation
Stakeholders Policies

19
Ancillary Services
• Optical services – Shop/workshop; Concession or own– Need excellent refraction
• Pharmacy
• Cafeteria, coffee dispenser, kiosk
• Accommodation (for outreach patients)

20
Trained Staff
• Ophthalmologists FT + PT
• Technicians 4:1
• New staff - Manager, Accountant, Counselor, Outreach, Stores, Maintenance
• On-job training
• Clarify structure &lines of authority

21
Manager and Systems
• Relieves ophthalmologist of administrative responsibilities
• “Line manager” monitors systems/patient flow daily– Registration, VA, refraction, diagnostic studies,
exam, treatment, surgery, optical sales, discharge, administration etc.
• Only when monitor can you expect improvement

22
Demand - Find More Patients
• Purpose of Outreach – Stimulates demand for services and
provides visibility – Reach hard to reach populations
• Balance between Services and Outreach
– Develop services first and use outreach to benefit the clinic

23
Diversify Financial Sources
• Self-earned revenue enhances independence – reinvest into practice
• Explore options - fees, optical, pharmacy, cafeteria, community support for outreach
• Manage donors, government, business

24
Efficiencies & Reduce Costs
• “Increase volume, lower cost”– Reduce price, lower cost to lower 60% – Evaluate cost effectiveness
• Standardized practices improve efficiency– Surgery and patient flow through– Equipment, medical supplies, outreach
• Focus on services done well, e.g., cataract and avoid distractive projects

25
Does this work? Regional Examples
• Peru – 5 year incr. surg. 655 to 2,229 (240%); revenue incr. 290%
• Mexico – reduced waiting time 44% by reorganized flow 1 day
• Rapidly growing experience– Asia, Egypt, Africa– Mexico, Guatemala, Honduras, El Salvador,
Nicaragua, Peru, Equator, Paraguay, Brazil
• Guatemala – 6 year incr. surg. 464 to 5,680 (1,124%)

26
Surgery
-
1,000
2,000
3,000
4,000
5,000
6,000
2006 2007 2008 2009 2010 2011
Cataract Surgery All Surgery
DNJ, Peru

27
Patient Choice – Simplified Pricing
0 500 1000 1500 2000 2500
2008
2009
2010
2011
Free Subsidized Paying
DNJ, Peru

28
Diversify Revenue
0 200000 400000 600000 800000
2006
2007
2008
2009
2010
2012
OPD Surgery Optical Other
DNJ, Peru

29
Financial Self-sufficiency
0
100000
200000
300000
400000
500000
600000
700000
800000
2006 2007 2008 2009 2010 2012
Income Expense
DNJ, Peru

30
Managed Change Process
• Starts with an ending/ manage transition
• Are there problems implementing this? SURE
• What is worst case scenario? IMPROVEMENTS
• Will this work in Haiti? LETS FIND OUT

31
What About Haiti
• Cap Haitien experience “Vision Plus”
• Private and social clinic/ 3-4 lanes
• Operating theatre
• Optical sale P & S
• Coordinated with government service and medical missions
• Vision for the Poor, IEF, Deseret Fnd, Visualiza, room for others…

32
Challenges
• Funding • Shipping and customs• Establishing duty free/ Foundation status • Multiple demands on too few people
(missions, projects, meetings etc)• Test market assumptions
– Patient population - paying, subsidized, free– Other providers– Enabling policies

33
Future Plans?
• What we would like… might do…• Demonstrate sustainability planning• Evaluate capacity and feasibility of 5
clinics with ORs• Conduct sustainability workshops• Develop sustainability plans w/financial
and productivity projections• Facilitate technical intervention and
exchange training

34
Crisis or Opportunity?
Have I?
• Modeled a way?
• Inspired a shared vision?
• Challenged the process?
• Enable you to act?
• Encouraged from the heart?

35
FeedbackWhat (+) things might happen if I apply this approach?
What (-) things might happen if I apply this approach?
What will make it easier for me to apply this approach?
What will make it more difficult to apply this approach?
Who will approve/support me to apply this approach?
Who will disapprove/hinder me from applying this approach?
I believe I can apply this approach.
I don't believe I can apply this approach.

36
"The burgeoning rates of blindness, 90% of which is in developing countries, can only be addressed when the quality of eye care is that which patients will seek, accept, and for those who can afford, be willing to pay for. While training more eye care professionals is a piece of a larger puzzle, the root causes of current inefficiencies, poor quality, and under-utilization of services lie in the poor management and the lack of financial sustainability of existing services."
International eye foundation monograph 2005
Thank You





![Barrows Visit Dexfield2[1]](https://static.fdocuments.in/doc/165x107/577ccfd91a28ab9e7890c044/barrows-visit-dexfield21.jpg)