1 Creating Trauma Informed Systems of Care Overview of National Initiative to Promote Recovery,...
64
1 Creating Trauma Informed Systems of Care Overview of National Initiative to Promote Recovery, Resiliency & Trauma Informed Care Developed by Kevin Huckshorn, Director, NASMHPD Office of Technical Assistance, 2007 Adapted by Beth Caldwell for January 2008 Training Program
-
Upload
cecil-gallagher -
Category
Documents
-
view
215 -
download
0
Transcript of 1 Creating Trauma Informed Systems of Care Overview of National Initiative to Promote Recovery,...

1
Creating Trauma Informed Systems of Care
Overview of National Initiative to Promote
Recovery, Resiliency & Trauma Informed Care
Developed by Kevin Huckshorn, Director, NASMHPD Office of Technical Assistance, 2007
Adapted by Beth Caldwell for January 2008 Training Program

2
INTRODUCE YOURSELF TO SOMEONE YOU DO NOT KNOW
SHARE
Your Name
What You Do
A Strength You Have in Working with Children

3
ACKNOWLEDGEMENTS
Kevin Ann Huckshorn National Association of State
Mental Health Program Directors (703) 739-9333
Dr. Janice LeBelMA Department of Mental Health
Funded by the Substance Abuse and Mental Health Services Administration

4
Brief Historical Overview National S/R Reduction Initiative
1998: Hartford Courant Series
1999: GAO Report (Congress) - NASMHPD MD S/R Report
- CMS Rule changes
2001: CMS Rule Changes (one-hour)
2002: NASMHPD Training Curriculum
created

5
Restraint and SeclusionAre Not Treatment
In 1999, the NASMHPD Medical DirectorsCouncil debated the challenge of R/Sreduction/elimination.
They determined and declared:
Restraint and seclusion are not therapeutic and reflect a failure in treatment.

6
Brief Historical Overview National S/R Reduction Initiative
2003: - NTAC Training starts
- New Freedom Commission Report –
Transformation
- Independent projects support core strategies identified
2006: CMS Final Rules (disappointing)
(NAPHS Success Stories 2003; Colton, 2004; Murphy/Davis, 2005; CWLA; 2003)

7
Brief Historical Overview National S/R Reduction Initiative(s)
2004-2010Previous S/R CMHS SIG Activities
2004: 8 State Incentive Grants to identify alternatives to reduce use (HI, IL, KY, LA, MA, MD, MO, WA)Three year grants included large scale evaluation project with research center in Cambridge (HSRI) and best practice applicationsThis data are currently being analyzed by HSRI and a group of consumer expert researchersData available in next few months

8
Brief Historical Overview National S/R Reduction Initiative(s)
2004-2010
New SIG Project2007-10: New round of grants, 8 states (CT, IN NJ, NY, OK, TX, VA, VT)
NTAC remains the S/R SIG Coordinating Center under auspices of CMHS and NASMHPD
Using lessons learned we are proposing a comprehensive training on S/R reduction strategies ‘early on’ and a consultant visit model that includes peers, over the next 3 years.

9
What We Know at this Point:
Started with adult hospital programs
Moved to child mental health, child welfare and juvenile justice residential programs
Significant + outcomes related to reduction in staff & child injuries; child, family & staff satisfaction; agency functioning
Still evolving and young initiative - yet constructs & strategies resonate with best and evidence-based practices

10
We (NTAC & faculty) know what helps to reduce S/R…, at this point…
We know that the reduction of S/R is possible in all mental health settings
We know that facilities throughout the U.S. have reduced use considerably without additional resources
We know that this effort takes tremendous leadership, commitment, and motivation

11
Framing the Issue
The reduction of seclusion, restraint and coercive practices requires a CULTURE CHANGE in our mental health treatment settings that results in far more than just prevention S/R (Huckshorn, 2006).
This ‘Culture Change’ must be congruent with recovery and transformation principles
Best practice core strategies have been identified
However, practice and system change is slow and difficult… for many reasons…

12
Needed Healthcare System Changes? …not just about mental health or reducing
violence….
Healthcare systems including Behavioral Health continue to be fragmented
Not customer friendly or person-centered
Not outcome-oriented
Waste resources
Poor communication between providers
Practices not based on evidence(USDHHS, 1999; IOM, 2001)

13
Facilitating Culture Change in U.S. Healthcare Organizations: The IOM
ReportsThe U.S. Institute of Medicine described new rules to transition the redesign and improvement in health care (IOM, 2001, 2005)
Continuous healing relationships
Customized to individual needs/values
Consumer is source of control
Free flow of information/transparency
Use of Best Practices

14
Facilitating Culture Change in Mental Health: The U.S MH New
Freedom Commission Report
A Call for System TransformationSystem Goal = Recovery for everyoneServices/supports are consumer-centeredFocus of care must increase consumers’ ability to self manage illness and build resiliencyIndividualized Plans of Care criticalConsumers and Families are full partners
(New Freedom Commission, 2003)

15
A Vision of Mental Health:The Future in the U.S…?
Service users are employed in every setting, up to 30-50% of staff
Treatment planning is directed by the consumer, and family, whenever possible
Language used is “person-centered and non-discriminatory”
Evidence-based practices (EBP) are the norm, including non-coercion, effective use of meds, family education, and a treatment focus on illness self- management

16
Preventing violence, coercion, seclusion and restraint (S/R) fits these calls for
action and changeWe have come to believe that this work is a fundamental cornerstone in transforming our systems of careEffective Leadership is criticalNew staff knowledge and practice changes will set a foundationChanges include using evidence-based practices, including meds; creating treatment activities that teach illness management; person-directed planning; workforce development; and preventing coercion and discrimination

17
Development of the Curriculum to Reduce the Use of S/R
Ongoing Review of LiteratureQualitative Reports emerged from personal experiences (self and colleagues) with direct experiences in successful reduction projects across the countryQualitative Reports emerged from service users and staff (ongoing)Core strategies emerged in themes over time Expert Meeting(s) held in DC in 2001, 2002, 2003, and 2007 to refine

18
What are the Main Change Constructs in Preventing Conflict, Violence and S/R use?
Leadership Principles in effective changeThe Public Health Prevention approachUse of Recovery/Resiliency PrinciplesValuing Consumer/Staff Self ReportsTrauma Knowledge operationalizedStaying true to CQI Principles (the ability to take risks to assure individualized treatment occurs)

19
The Public Health Prevention Model
The Public Health approach is a model of disease prevention and health promotion and is a logical fit with a practice issue such as S/R
This approach identifies contributing factors and creates remedies to prevent, minimize and/or mitigate the problem if it occurs
It refocused us on prevention while maintaining safe use

2020
Public Health Prevention ModelPublic Health Prevention Model
Tertiary
Primary
Seco
ndar
y

21
The Public Health Prevention Model applied to S/R Reduction
Primary Prevention (Universal Precautions)Early interventions designed to prevent conflict from occurring at all by anticipating risk factors & addressing
Secondary Prevention (Selective Interventions)Early interventions to minimize and resolve conflicts when they occur to prevent S/R use
Tertiary Prevention (Indicated Interventions)Post S/R interventions designed to mitigate effects, analyze events, take corrective actions, and avoid reoccurrences.

22
Recovery/Resiliency Principles
New Freedom Commission Goal: Build Resiliency
Facilitate Recovery
The use of S/R is counter-intuitive
Coercive or traumatizing settings do NOT foster hope, healthy relationships, pro-social behaviors or trust
(New Freedom Commission, 2003; Onken et al, 2002)

23
Trauma-Informed CareEmerging science based on high prevalence of traumatic life experiences in people we serve - up to 98% (Muesar et al, 1998)
Says that traumatic life experiences cause mental health or other problems or seriously complicate these, including treatment resistance
(NETI, 2005; Felitti et al, 1998)
Systems of care that are trauma informed recognize that coercive or violent interventions cause trauma and are to be avoidedUniversal precautions required (NETI, 2005)

24
Consumer/Staff self-reports
“The first time that I helped with a restraint, a four-point restraint, I walked out of the room in tears because it was one of the most horrible things I
had ever seen.” (female direct care staff)
"The seclusion made me feel even more angry because it hurt me and made me worse. I would like staff to respond in a different way such as
give you more options during the step before they act too quickly."
(Samantha Jones, age 41)

25
First Steps? Develop a Written Facility Plan!
TO START: Leaders Must Develop a S/R Reduction Action Plan that is specific to their settings
Action Plan Framework Prevention-Based Approach Continuous Quality Improvement Principles Individualized for the Facility or Agency Adopt/adapt Six Core Strategies ©

26
The Six Core Strategies© to Prevent Violence and S/R
1) Leadership Toward Organizational Change
2) Use Data To Inform Practices
3) Develop Your Workforce
4) Implement S/R Prevention Tools
5) Actively recruit and include service users and families in all activities
6) Make Debriefing rigorous

27
Core Strategy #1Leadership in Organizational ChangeThe most important component in successful prevention and culture change projects.
Only Leadership has the authority to make the changes that are necessary for success:
To make violence prevention a high priorityTo assure for an organized Plan To reduce/eliminate organizational barriersTo provide or re-allocate the necessary resourcesTo hold people accountable for their actions

28
Core Strategy #1Leadership in Organizational Change
Create A Vision
Live Key Values
Develop your Human Technology
Monitor Staff Performance
Elevate Oversight of Untoward EventsAssure Violence/S/R Prevention Plan Development (Anthony, 2004; Huckshorn, 2004)

29
Core Strategy #2Using Data to Inform Practice
Leaders and staff must use information to drive change; to start:
Identify your definitions of violent events, S/R, imminent danger, reportable injuries, stat med useGather historical data by event/hours (6 months to 1 year) to use as baselineSet realistic goals or 100% reductionPost reports on units monthlyMandate data collection on S/R events, hours, stat meds, and consumer and staff injuries

30
Core Strategy #2Using Data to Inform Practice
Use Data To Identify &Analyze Events:Unit/Day/Shift/Time of day
Age/Gender/Race
Date of admission/Diagnosis
Attending Physician
Pattern of staff involved in events
Number of Grievances

31
Core Strategy # 2Using Data to Inform Practice
Use Data To:
Monitor Progress
Discover new best practices
Identify emerging staff champions
Target certain units/staff for training
Create healthy competition
Assure that everyone knows what is going on

32
Core Strategy #3 Workforce Development
Integrate S/R Reduction & Violence
Prevention in Human Resource & Staff Development Activities
In New Hire procedures
In revising Job Descriptions and Competencies
In doing Performance Evaluations
In New Employee Orientation
In Annual Reviews

33
Core Strategy #3 Workforce Development
Leadership and staff will require education on key concepts, including:
The Public Health Prevention Approach
Common Assumptions about S/R
Experiences of staff and adults/kids with S/R
The Neurobiological/psychological effects of Trauma
Roles of Consumers, Families and Advocates
Negotiation and Problem-solving skills

34
Core Strategy #3 Workforce Development
Creating Trauma-Informed Systems and Services
Principles of Recovery/Building Resiliency
Matching Interventions with Behaviors
Use of Prevention Tools (violence, death/injury, trauma, de-escalation, safety plans, environmental changes, language)
Roles in rigorous debriefing

35
Core Strategy #4Use Violence/S/R Prevention Tools
Choose and Implement Violence and S/R Prevention Tools
Assess risk factors for violence and S/R use
Assess risk factors for death and injury
Implement Universal Trauma Assessment
Use Safety Plans/Crisis Plans/Advance Directives to identify triggers/preferences
(NETI, 2005)

36
Core Strategy #4Use Violence/S/R Prevention Tools
Use of comfort rooms Implement sensory rooms and sensory interventionsIncorporate Person First LanguageMonitor Training Guidelines (De-escalation models)Effective Treatment Activities Manage overcrowding
(NETI, 2005)

37
Core Strategy #5 Full Customer/Advocate Inclusion
Hire peers in recovery, family members/community advocates as staff members, use volunteers
Make information available
Use to interview service user post-event
Attend meetings - all levels
Empower and support participation

38
Core Strategy #5 Full Customer/Advocate Inclusion
Common roles for adult peersDirector of Drop-in CenterDirector of Consumer Affairs OfficeMental health technicianRecovery specialistDebriefing specialistTreatment Team AdvocateStaff in QI DepartmentTrainer

39
Core Strategy #6Make Debriefing Rigorous
Definition of Debriefing
A stepwise tool designed to:rigorously analyze a critical event,
examine what occurred and
facilitate an improved outcome next time (manage events better or avoid event)
(Scholtes et al, 1998)

40
Debriefing Goals
To prevent the future use of seclusion and restraint
(Cook et al, 2002; Hardenstine, 2001)
To minimize the negative effects of the use of seclusion and restraint
(Massachusetts DMH, 2001; Huckshorn, 2001; Cook et al, 2002; Hardenstine, 2001; Goetz, 2000)
To address organizational issues and make appropriate changes.
(Huckshorn, 2007; Duxbury, 2002; Richter & Whittington, 2006)

41
Debriefing SpecificsDevelop or revise your policy
Implement two types of Debriefing Activities Acute - immediate post event response
to gather info, manage milieu, assure safety
Formal - rigorous problem solving event with treatment team and consumer input, usually 24 hours later
R

42
New Research on Violence Causality and Role of the Environment
Violence in mental health settings has been blamed on the “patient” for years
Hundreds of studies done on patient demographics and characteristics
Findings are completely variable and inconclusiveMore recently, studies have looked at the role of the environment in violence, including staff (Richter & Whittington, 2006; Johnstone & Cooke, 2007)

43
Promoting Risk Interventions by Situational Management (Johnstone & Cooke, 2007)
Past research has focused on evaluation the ‘patient’ for risk factors due to mental illness and criminogenic factors (p. 8)
However, this focus has been judged to be severely limited as it ignored environmental factors. Conflict and violence in inpatient MH settings is believed to be complicated and multi-factorial. “Human behavior does not occur in a vacuum…” (p. 9).

44
Promoting Risk Interventions by Situational Management (Johnstone & Cooke, 2007)
Situational factors refer to features or characteristics of the environment in which they occur.
These can include the physical setting, personal comfort, staff issues and attitudes, physical space, privacy, noise levels, unit activity levels, individual needs for freedom & other issues
This is not a new concept, just one that has been ignored for years and may be a function of discrimination and its most ugly consequences.

45
Exercise
1) Please think for two minutes about what is important for you to do when you get home from work. Do you make phone calls, take a shower, turn on the news, get something to eat, go work out, walk? Write this activity down on paper.
2) How would you handle being told that you could not do this as the rules do not permit it; that your request is “not allowed” and unavailable to you? And not for one day but for many days? And perhaps while you see others being able to do your requested activity?

46
Promoting Risk Interventions by Situational Management (Johnstone & Cooke, 2007)
Your over-arching goal here is to manage the risk of conflict and violence, as without that, neither seclusion or restraint are likely to occur.
As leaders in this effort it is going to be your challenge to investigate these issues and come up with strategies to help your staff to do this prevention work.

47
Promoting Risk Interventions by Situational Management (Johnstone & Cooke, 2007)
Our role (NTAC& faculty) is simply to help you. We will be hosting a training, supported by CMHS, to train your facilities leaders in this work. Your “role” is to identify and involve your CEO’s, Directors, Nurse leaders, Medical Directors, QI Directors, staff trainers, and any other staff that have the formal and informal power to make these changes in your facilities unfold.

48
SUCCESSFUL OUTCOMES
Yes – in a variety of settings

49
Variety of Types of Programs
Adult FacilitiesSalem Hospital -100%No. VA MH Institute - 99%Worcester State Hospital - 98%Western State Hospital - 79%
Child & Adolescent FacilitiesCambridge Child Assmnt Unit -100%Boston Medical Center IRTP -100%
Holston United Methodist Home - 95%
Natchaug Hospital - 93%

50
Variety of Types of Programs
Intellectual & DD FacilitiesMillcreek in MS (225 beds) - 100%Siffrin in OH (300 beds) - 100%Lutheran in WI (1,000 beds) - 100%LifeShare in NH, ME & FL - 100%
(Ohio, 2005)
Forensic FacilitiesTaylor Hardin Secure Medical Ctr. - 99%North Texas State Hospital - 50%+Treasure Coast Forensic Tx Center

51
NTAC S/R Training Pre/Post Data(NRI, 2003)
The data showed that S/R hours were reduced by as much as 79%, the proportion of consumers in S/R was reduced by as much as 62%, and the incidents of S/R events in a month were reduced by as much as 68%.
(HSRI Fast Facts, 2004)

52
EXAMPLES OF OUTCOMES FROM CHILD PROGRAMS THAT HAVE
REDUCED S/R
Southern Oregon Adolescent Study & Treatment Center (R/S < 85% in 18 months: Avg CAFAS score at discharge from 40 to 78; < staff turnover; < runaways)

5353
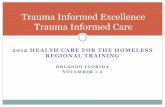
MA R/S Episodes Decreased Dramatically
Child - 79.7%Adolescent - 59.8%Mixed C/A - 81.5%
C/A DMH Acute and Continuing Care FacilitiesTotal R/S Episodes per 1000 Patient Days
84.0
27.98
72.2
29.04
73.4
24.33
0
10
20
30
40
50
60
70
80
90
100
11/1/99 - 10/31/00 9/1/01 - 12/31/04
Significant Periods
# E
pis
od
es p
er
1000 P
ati
en
t D
ays
Child
Adolescent
Mixed C/A
Pre-Intervention
Post-Intervention

5454
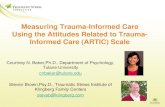
MA R/S Hours Also Reduced
ChildChild - 30.5%- 30.5%AdolescentAdolescent - 58.3%- 58.3%
Mixed C/AMixed C/A -19.2%-19.2%
C/A DMH Licensed and State FacilitiesTotal RS Hours per Episode
0.59
0.41
2.18
0.91
0.520.42
0.00
0.50
1.00
1.50
2.00
2.50
11/1/99 - 10/31/00 9/1/01 - 6/30/04
Significant Periods
# H
ou
rs p
er E
pis
od
e
Child
Adolescent
Mixed C/A
Pre-Intervention
Post-Intervention

5555
MA MedicationRestraint Dropped
ChildChild - 49.5%- 49.5%AdolescentAdolescent - 28.6%- 28.6%Mixed C/AMixed C/A - 77.4%- 77.4%
C/A DMH Acute and Continuing Care FacilitiesInvoluntary Administration of Medication
Episodes per 1000 Patient Days
21.3
10.75
15.9
11.35
32.5
7.34
0
10
20
30
40
11/1/99 - 10/31/00 9/1/01 - 12/31/04
Significant Periods
# E
pis
od
es p
er
1000 P
ati
en
t D
ays
Child
Adolescent
Mixed C/A
Pre-Intervention
Post-Intervention

56
Massachusetts ResultsExamples of Most Successful Units-100% Collaborative Problem-Solving
Approach, close supervision, elevating the role of MHW
-100% Trauma System Treatment Model- 99% Holistic Health Approach
- 91% Fostering Resilience in Children
- 86% Strength Based Approach, threw out mechanical restraints
- 78% Conversion to Relationship Model

5757
Boston Medical Center Intensive Residential Treatment Program
Total Seclusion, Restraint & Injury Episodes09/00 - 05/07
0
10
20
30
40
50
60
70
80S
ep
-00
Jan
-01
Ma
y-0
1
Se
p-0
1
Jan
-02
Ma
y-0
2
Se
p-0
2
Jan
-03
Ma
y-0
3
Se
p-0
3
Jan
-04
Ma
y-0
4
Se
p-0
4
Jan
-05
Ma
y-0
5
Se
p-0
5
Jan
-06
Ma
y-0
6
Se
p-0
6
Jan
-07
Ma
y-0
7
Significant Periods
SR
& I
nju
ry E
pis
od
es
SR Episodes
Kid Injury
Staff Injury
St

5858
Seclusion and Restraint Orders and
Patient Related Employee Injuries
Worcester State Hospital
Q4 FY '00 - Q1 FY '05
0
200
400
600
800
1000
1200
Q4 FY00
Q1 FY01
Q2 FY01
Q3 FY01
Q4 FY01
Q1 FY02
Q2 FY02
Q3 FY02
Q4 FY02
Q1 FY03
Q2 FY03
Q3 FY03
Q4 FY03
Q1 FY04
Q2 FY04
Q3 FY04
Q4 FY04
Q1 FY05
S/R
Ord
ers
0
5
10
15
20
25
30
35
40
45
50
Pat
ien
t R
elat
ed E
mp
loye
e In
juri
es # S/R Orders
# PatientRelatedEmployeeInjuries

59
Strategies MA/Oregon Programs Began to Address
Strength-based Approach (e.g., strength-based assessments, daily focus on strengths, environment plastered with strengths, 5 or 8-1 use of praise, respectful interactions, both children and families)
Family PartnershipsSelf-Esteem Building Activities Sensitive Listening and Questioning

60
Strategies MA/Oregon Programs Began to Address
Child/Parent Identifying and Learning to Recognize/Use Triggers, Warning Signs Coping Strategies & Regular Updates /Reviews (i.e., risk assessments, use of safety plans)
Skill Building Focus Staff Expertise in a Range of Negotiation
& De-escalation Techniques

61
Strategies MA/Oregon Programs Began to Address
Trauma Informed CareIdentifying and Implementing Distinct
Models of Care Eliminating/Revamping Motivation
Systems Involving and Empowering Staff (i.e.
communication, sharing of data, not constricted by ‘rules’)
Letting Go of Control Issues/Choices

62
Strategies MA/Oregon Programs Employed
Warmth of Décor Proactive/Varied Activity Schedule Focus on Holistic Activities (e.g., yoga, dog
therapy) Interviewing for, Hiring, Evaluating for:
Caring & Compassionate Staff Use of Touch Sensory/Calming Rooms Variety of Sensory Tools

63
Final Thought to Ponder…
Martin Luther King JR. said that:
“Violence is the language of the unheard”
Seems to be a particularly germane statement regarding our settings.
Let’s give these findings the attention they
deserve, for our children and adolescents, their families and our staff …

64
Contact Information
Beth Caldwell Caldwell Management Associates
413-644-9319 [email protected]
Dr. Janice Le BelMA Department of Mental Health
Kevin Ann Huckshorn or Sarah CallahanNational Association of State
Mental Health Program Directors (703) 739-9333