1 Characteristics and risk factors of fall injury in Taiwan in 1999 vs 2007 Yih-Jian Tsai* MD, MSc,...
31
1 Characteristics and risk factors of fall injury in Taiwan in 1999 vs 2007 Yih-Jian Tsai* MD, MSc, PhD candidate LSHTM 140 th APHA 4275.0 International Health and Aging and Healthcare Policy 2:54-3:06 pm, Moscone Convention Center West, San Francisco, CA * Section Chief, Adult and Elderly Health Division, Bureau of Health Promotion, Department of Health, Taiwan, ROC
-
Upload
pauline-hampton -
Category
Documents
-
view
221 -
download
4
Transcript of 1 Characteristics and risk factors of fall injury in Taiwan in 1999 vs 2007 Yih-Jian Tsai* MD, MSc,...

1
Characteristics and risk factors of fall injury in Taiwan in 1999 vs 2007
Yih-Jian Tsai* MD, MSc, PhD candidate LSHTM
140 th APHA
4275.0 International Health and Aging and Healthcare Policy
2:54-3:06 pm, Moscone Convention Center West, San Francisco, CA
* Section Chief, Adult and Elderly Health Division, Bureau of Health Promotion, Department of Health, Taiwan, ROC

2
Outline
Introduction Subjects and Methods Results Discussion Conclusions

3
Introduction
Falls are one of the leading causes of global
burden of disease (Barss et al., 1998)
Fallers are more likely to be admitted into hospitals, nursing homes, and to consume more medical care resources, and to have more functional limitations in ADLs and IADLs (Kiel et al., 1991)
Among fallers of injury fall events, 42.3 % need hospitalization, and 37.0 % of those hospitalised have to move into nursing homes after discharge (Sattin et al., 1990)
Emergency Department Visits
In 2006, 10.5 % of all ED visits among the elderly in the US were claimed by injurious falls, of whichabout seven tenth was released from the ED; the remaining three tenths resulted in hospital
admission. The overall rate of ED visits for injurious falls was
57.4 visits per 1000 person 65 years and older.
112/04/194
Ref: Owens PL, Russo CA, Spector W, Mutter R. Emergency Department Visits for Injurious Falls among the Elderly, 2006: Statistical Brief #80. <http://www.ncbi.nlm.nih.gov/pubmed/21452495> Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Health Care Policy and Research (US); 2006 Feb-.
5
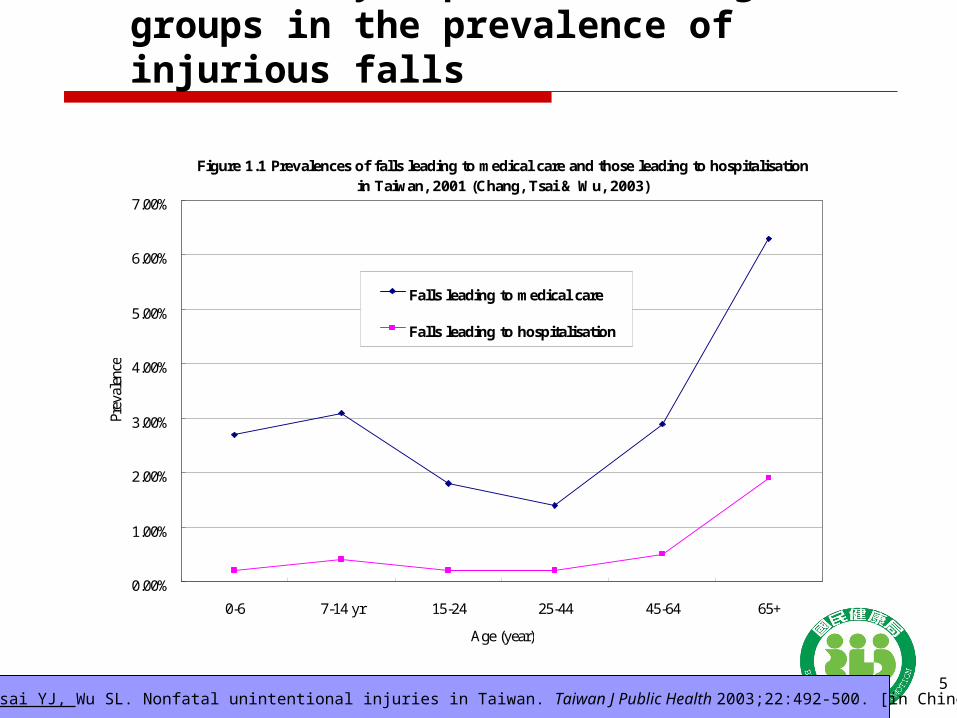
Figure 1.1 Prevalences of falls leading to medical care and those leading to hospitalisationin Taiwan, 2001 (Chang, Tsai & Wu, 2003)
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
0-6 7-14 yr 15-24 25-44 45-64 65+
Age (year)
Prev
alen
ce
Falls leading to medical care
Falls leading to hospitalisation
The elderly top the other age groups in the prevalence of injurious falls
Chang FC, Tsai YJ, Wu SL. Nonfatal unintentional injuries in Taiwan. Taiwan J Public Health 2003;22:492-500. [in Chinese]

6
Questions
What is the difference of injurious falls in terms of induced fall injury, consequent medical care utilization, and risk factors in the elderly in Taiwan between 1999 and 2007?
7
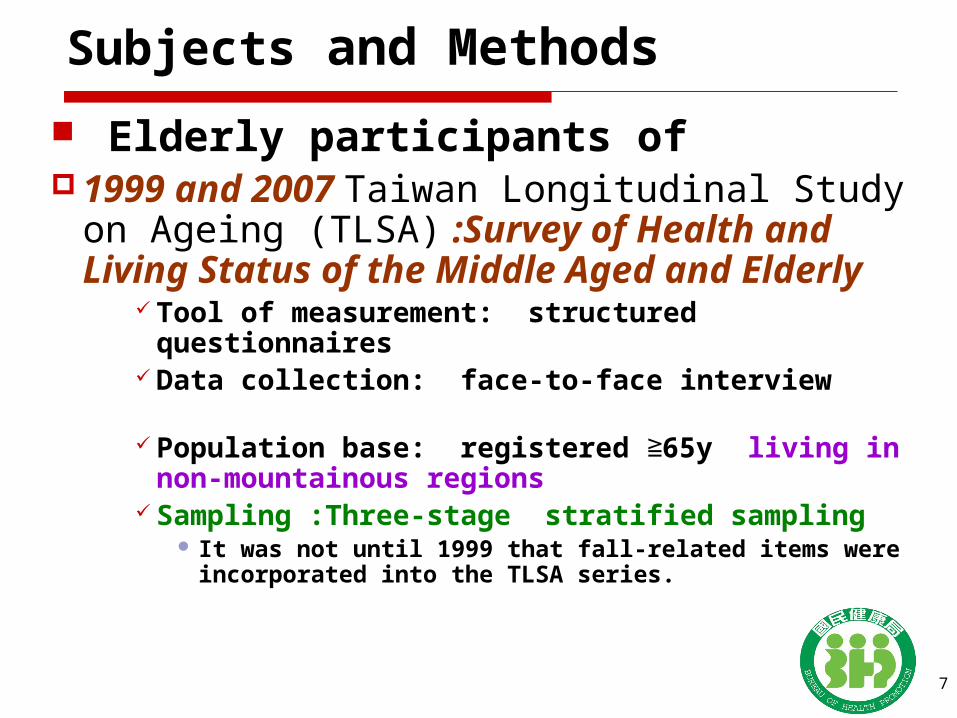
Subjects and Methods
Elderly participants of 1999 and 2007 Taiwan Longitudinal Study on
Ageing (TLSA) :Survey of Health and Living Status of the Middle Aged and Elderly
Tool of measurement: structured questionnaires Data collection: face-to-face interview Population base: registered 65y ≧ living in non-
mountainous regions Sampling :Three-stage stratified sampling
It was not until 1999 that fall-related items were incorporated into the TLSA series.

Year No. of Respondents
Age No. of Non-respondents
Response rate
1989 4049 (B) 60+ 363 91.8%
1993 3155 (B) 64+ 312 91.0%
1996 2669 (B) 67+ 333 88.9%
2462 (A) 50-66 570 81.2%
1999 2310 (B) 70+ 253 90.1%
2130 (A) 53-69 222 90.6%
2003 1743 (B) 74+ 173 91.0%
2035 (A) 57-73 174 92.1%
1599 (C) 50-56 423 79.1%
2007 1268 (B) 78+ 120 91.4%
1864 (A) 61-77 188 90.8%
1402 (C) 54-60 159 89.8%
Chronological sample size of respondents by age

9
Fall
C8. During the past one year, have you fallen down (including falling while walking, due to a slippery surface, while sitting down or standing up, due to fainting, or while trying to lie down, no matter if there was injury or not)?
___ 1 Yes ___0 No [Skip to C13]
10
Injurious falls, Fall Injury
Injurious falls: Did that fall cause a bone fracture or hairline fracture, sprain or dislocation?
___0 No [Skip to C11] ___1 Yes
Fall Injury: Where (i.e., what part of the body) was the fracture, hairline fracture, sprain or dislocation? [Can choose more than one.] Head, Neck, Spine, Lower limb, Upper limb, Hip, Trunk, Other

Medical care utilization
C10b. Where did you go for treatment? [Can choose more than one.]___1 Didn’t go for treatment; respondent treated
it himself/herself (self care)___2 Bone-setting clinic or healing martial arts
center__ 3 Chinese medicine hospital or clinic___4 Western medicine hospital or clinic___5 Other (please explain):_______

Socio-demographic factors:AgeSexADLIADLMedical factors, Physical
and Mental function : Sleeping pills or sedative useVisionWalk aid useExerciseNo. of chronic diseasesIncontinenceBody painDepressive symptomsCognitive function
1999 、 2007 TLSAInjurious falls
Medical care utilization
Body site injured
Study framework

Socio-demographic factors
13
Age (yr) 65-69; 70-74; 75-79; 80-84; 85+
Sex Male; Female
ADL dependency with any dependency in terms of eating, getting in/out of bed (or sitting down in/get up from a chair), walking around the house, getting dressed, bathing, and using the toilet
IADL dependency
with any dependency in terms of light housework- e.g. straightening up the living room, washing dishes, etc.; buying everyday use items; managing finances- e.g. performing calculations, and paying bills; making telephone calls
Medical factors, Physical function
14
Sleeping pills or sedative use
Yes; no
Vision very clear/clear; average; and unclear/very unclear).
Walk aid use Yes; no
Exercise frequency of exercise per week: no, irregular exercise ( 2 times per week), regular exercise (3 or more times ≦per week

Medical factors, Physical function
15
No. of chronic diseases
History of fourteen chronic diseases was taken and total number of chronic diseases were classified into three categories 0; 1; 2≧
Hypertension , diabetes, heart diseases, stroke, cataract, respiratory diseases (bronchitis/respiratory tract infection/other respiratory disorder/asthma), arthritis/rheumatism, gastric ulcer/stomach ailment, liver or gall bladder diseases, hip fracture, cataract, kidney disease, gout, spinal spur.
Incontinence If with trouble of incontinence: either with urination or with defecation, or both.
Body pain categorized into three groups: None/a little; Medium; More or very serious

Mental functionDepressive symptoms
Depressive symptom: measured with ten CES-D scale questions, eight are negative, while two are positive. Each question was scored 0-3 according to the frequency of the feeling. Question scores were summed to provide the depression score, which was dichotomised, with modification to Andresen & Malmgren (1994) as: 0-7, without depressive symptoms; 8, with depressive symptom.
Cognitive impairment
Cognitive function was measured with the SPMSQ. Each question was given 1 score if answered correctly, and 0 if erroneous. Question scores of right answers were summed to provide the cognitive function score, which was divided and modulated according to educational level (Wu & Chang, 1997). For people of primary school level, their cognition were categorised by the cognitive function score as normal if scored 7-10, mildly impaired if 5-6, moderately impaired if 2-4, and severely impaired if 0-1. The corresponding categories are respectively 6-10, 4-5, 1-3, and 0 for those illiterate, and 8-10, 6-7, 3-5 and 0-2 for those of secondary school level or higher.
Data analysis To compare the 1999 with 2007 surveys in terms of:
Prevalence of falls/of injurious falls Type of injury, injury rate Body site injured Consequent medical care utilization Risk factors:
Uni- & bi-variate analyses: chi square test for categorical variables
Multi-variate logistic regression model adjusted for age, sex, IADL dependency, walk aid use, exercise, sleeping pills or sedative use,
vision, No. of chronic conditions, cognitive impairment
112/04/1917
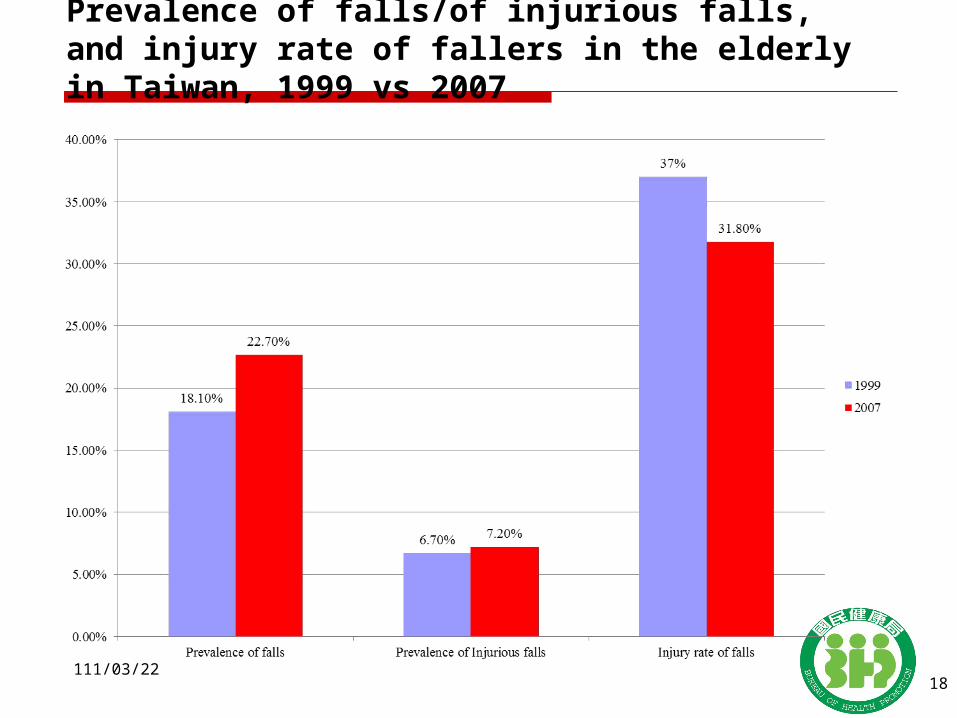
Prevalence of falls/of injurious falls, and injury rate of fallers in the elderly in Taiwan, 1999 vs 2007
112/04/1918

Type of injury among injurious fallers in Taiwan, 1999 vs 2007
112/04/1919

Distribution of injury among injurious fallers by body site in Taiwan, 1999 vs 2007
112/04/1920

Medical care utilized
1999(N=205)
2007(N=189)
n % n %
Western medicine 142 67.56 157 79.99
Chinese medicine 31 16.75 24 13.72
Bone setting clinic/healing martial arts center
42 21.79 30 17.52
Self care 19 10.31 (22*) (12.19)
Other care 5 2.56 1 0.32
*Note: Out of 211 injurious fallers, 22 took self care.
Medical care utilization among injurious fallers in Taiwan, 1999 vs 2007
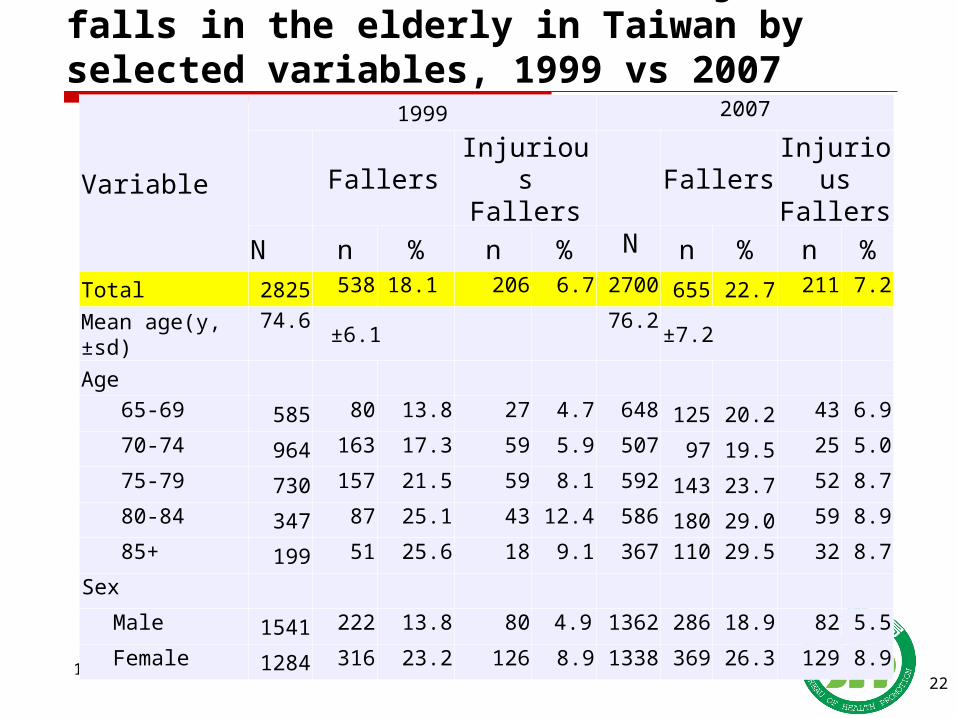
Prevalence of falls and of injurious falls in the elderly in Taiwan by selected variables, 1999 vs 2007
112/04/1922
Variable
1999 2007
FallersInjurious Fallers
Fallers
Injurious Fallers
N n % n % N n % n %
Total 2825 538 18.1 206 6.7 2700 655 22.7 211 7.2
Mean age(y, ±sd)74.6
±6.1
76.2
±7.2
Age
65-69 585 80 13.8 27 4.7 648 125 20.2 43 6.9
70-74 964 163 17.3 59 5.9 507 97 19.5 25 5.0
75-79 730 157 21.5 59 8.1 592 143 23.7 52 8.7
80-84 347 87 25.1 43 12.4 586 180 29.0 59 8.9
85+ 199 51 25.6 18 9.1 367 110 29.5 32 8.7
Sex
Male 1541 222 13.8 80 4.9 1362 286 18.9 82 5.5
Female 1284 316 23.2 126 8.9 1338 369 26.3 129 8.9
112/04/1923
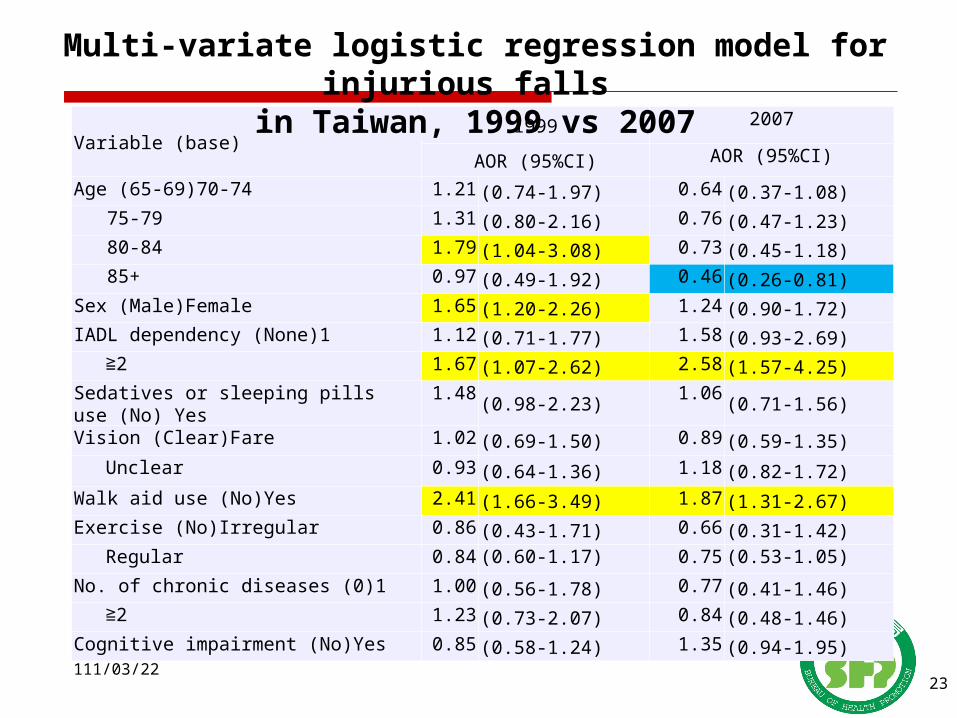
Variable (base)1999 2007
AOR (95%CI) AOR (95%CI)
Age (65-69)70-74 1.21 (0.74-1.97) 0.64 (0.37-1.08)
75-79 1.31 (0.80-2.16) 0.76 (0.47-1.23)80-84 1.79 (1.04-3.08) 0.73 (0.45-1.18)85+ 0.97 (0.49-1.92) 0.46 (0.26-0.81)
Sex (Male)Female 1.65 (1.20-2.26) 1.24 (0.90-1.72)IADL dependency (None)1 1.12 (0.71-1.77) 1.58 (0.93-2.69)
≧ 2 1.67 (1.07-2.62) 2.58 (1.57-4.25)Sedatives or sleeping pills use (No) Yes 1.48 (0.98-2.23) 1.06 (0.71-1.56)
Vision (Clear)Fare 1.02 (0.69-1.50) 0.89 (0.59-1.35)
Unclear 0.93 (0.64-1.36) 1.18 (0.82-1.72)
Walk aid use (No)Yes 2.41 (1.66-3.49) 1.87 (1.31-2.67)Exercise (No)Irregular 0.86 (0.43-1.71) 0.66 (0.31-1.42)
Regular 0.84 (0.60-1.17) 0.75 (0.53-1.05)
No. of chronic diseases (0)1 1.00 (0.56-1.78) 0.77 (0.41-1.46)≧ 2 1.23 (0.73-2.07) 0.84 (0.48-1.46)
Cognitive impairment (No)Yes 0.85 (0.58-1.24) 1.35 (0.94-1.95)
Multi-variate logistic regression model for injurious falls in Taiwan, 1999 vs 2007
Main findings
During 1999 and 2007, prevalence of falls↑ prevalence of injurious falls ↑ injury rate of fallers↓ multiple injuries ↑ a rising utilization rate for Western medicine care↑ a decreasing utilization rate for Chinese medicine care, and
for bone setting clinic/healing martial arts center ↓ The top three body sites injured were lower limb , upper
limb and hip.
112/04/1924
25
Discussion Demographic transition: with a rapidly ageing
population, female elderly will have 1.24 times the population size of male counterpart by 2025, when the share of elderly population will be more than 20% as a whole.
Epidemiologic transition: Prevalence of chronic diseases Morbidity expansion: a selectively beneficial effect on old-age survival
of those who had severe functional limitations (climbing stairs, walking) between 1993-1996-1999* under full coverage of the National Health Insurance program launched in 1995?.
*Zimmer, Martin & Chang. Population Studies 2002;56:265-276
26
Filial piety decayed? Health Inequality? Age-friendly environments?
Toward an Age-friendly society?

From 1999 to 2007, a rising utilization rate for Western medical care was found among injured fallers, Probably due to competitive use of a variety of
medical care, especially since the launch of NHI program.
The risk factors of injurious identified in multiple regression model were compatible with preceding study?
Advanced age: Sattin, Lamber Huber, DeVito et al. 1990, O’Loughlin et al. 1993; Yasumura et al., 1994
Female: weakness quadriceps, indoor stay (Yasumura et al., 1996; Schultz, Ashton-Miller & Alexander, 1997; Lord, Sambrook, Gilbert et al., 1994)
IADL dependency: Nourhashémi, Andrien, Gillette-Guyonnet et al. (2001), Lin et al.(2002)
Walk aid use: Tinetti, Williams, Mayewski et al., 1986b; Stalenhoef et al., 1997
but not for other risk factors: such as taking sleeping pills or sedative, vision, chronic conditions, cognitive impairment, exercise
Probably due to relatively fewer number of injurious fallers
112/04/1928
29
Strength
The 1999 & 2007 TLSA dataNational representativeLarge sample sizeQuality assurance of data collection
Interviewers’ training Questionnaire validity
Stable estimates for prevalence of injurious falls

30
Limitations
Cross-sectional survey on falls Recall bias Just association, instead of causal relationship
No further verification with medical record

Thanks for your attention
31