Regulation of Pay on Imposition of Penalty Under Ccs Cca Rules
Upload
elizabeth-mcelroyCategory
view
234download
2
1
Centre for Market and Public Organisation
Evidence on the impact of pay regulation on hospital quality and productivity
or Can pay regulation kill?Emma Hall, Carol Propper John Van Reenen
(Preliminary)

2
Motivation
• Unintended consequences of wage regulation– Pay setting (e.g. public sector) often has
“geographical equity” despite different local labor markets. Implies problems of labor supply and poor hospital performance when outside labor mkts strong
• How do labor markets affect firm performance?– Hard to identify as wages reflect equilibrium outcomes
of demand and supply shocks. Regulated pay helps identification.
• Policy issue in hospital performance– What are causes of large performance variation (note
also large productivity dispersion in other industries).

3
Large spread in death rates from AMI between hospitals (Fig 2)
• Improvements over time (cf. TECH Investigators) • 1996: 10 percentage point (60%) difference between top and bottom (90th =27%,10th =17%)
Worst 10%
Best 10%

4
Our Design• Wages for nurses (and doctors) in UK National Health
Service centrally set by National Pay Review Body. NPRB “Mandates” wage rates for doctors and nurses by grade. Uprated each year.
• Very little local variation in regulated pay despite substantial local variation in total private sector– E.g. 65% private sector pay gap between North-East
England and Inner London but only 11% in NPRB regulated pay
– Use exogenous variation in “outside wage” and examine impact on hospital outcomes (quality, prody)
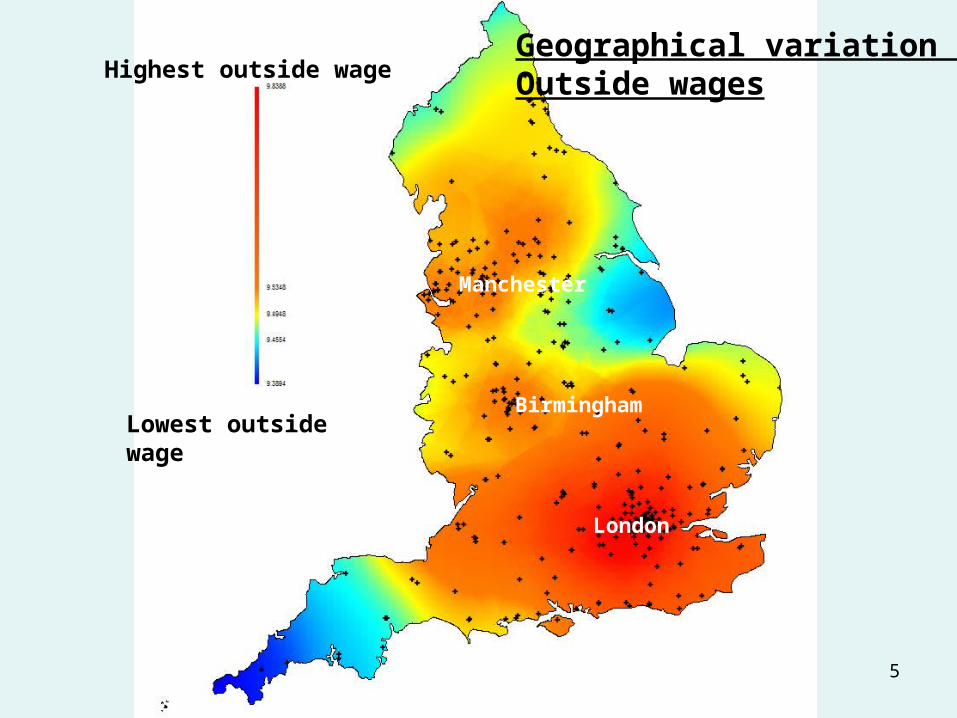
• Main Finding: Hospitals in high outside wage areas have lower hospital quality (higher AMI death rates) and lower output per head. One mechanism: greater reliance on lower quality temporary/agency staff.
5
Highest outside wage
Lowest outside wage
Geographical variation inOutside wages
London
Manchester
Birmingham

6
High intensity of agency nurses
Low intensity of agency nurses
Geographical variation in use of agency nurses
London

7
High AMI death rates
Low AMI death rates
Geographical variation in emergency AMI death rates
London

8
1. Models: What is the effect of pay regulation?
2. Empirical models
3. Data
4. Results
5. Conclusions
OUTLINE

9
1. Effects of high outside wage relative to regulated wage
• Employers– try to circumvent by “over-promoting” (grade drift) and increasing
non-wage benefits. Limited by regulation/union enforcement– Substitution to other factors: health care assistants, maybe
capital. But limited due to nature of needed expertise.– Substitute temporary agency staff. Lower job-specific human
capital so less productive/lower quality (cf Autor & Houseman, 2006)
• Employees – Lower participation, higher vacancies for permanent staff– More likely to become agency staff.– Permanent staff also less motivated, lower relative quality
compared to low outside wage areas
Implication: Worse hospital performance in high outside wage areas

10
Simple model
• 2 areas: high outside wage “South” and low outside wage “North”
• Regulated wage the same in both areas
• Regulated wage lower than equilibrium wage

11
Wages
N, employmentNSOUTHNNORTH
Labour Supply, South
Labour Supply,North
Labor Demand
Regulated Wage

12
Wages
N, employmentNSOUTH
Labour Supply, South
Labor Demand
Regulated Wage

13
Wages
N, employmentNPERMANENT
Labour Supply, South
Labor Demand
Regulated Wage
Agency Wage
NTOTAL
Agency staff

14
Implications
• In high outside wage areas– Problems of labor supply for permanent staff
• higher vacancies• lower participation in nursing• Greater reliance on agency nurses
– Worse health outcomes• Lower quality (AMI death rate)• Lower productivity
– What do we see in data?

15
Higher nurse vacancy rates1 in stronger labor markets (fig 4)
mean ln(outside wage)
Vacancy Rates for nurses predicted vacancy rate
9.4 9.6 9.8 10
1
2
3
4
5
North Ea
East MidYorkshirSouth We
West Mid
North We
East of
South Ea
Outer Lo
Inner Lo
1 Percentage of nurse posts that have been vacant for 3 months or more

16
Lower nurse participation rate in stronger labor markets (fig 5)
nurse relative pay premium
nurse participation rate Predicted participation rate
-.3 -.2 -.1 0 .1
.4
.5
.6
.7
.8
Lndon-In
SouthEas
Lndon-Ou
NorthWes
SthWest
Mdlnds-W
E.Anglia
Mdlnds-E
North
Yorks
Note: participation rate is the % of women with nursing qualifications who areworking as nurses

17
Higher use of agency nurses in stronger labor markets (Fig 6)
mean ln(outside wage)
Intensity of using agency nurse predicted Agency rate
9.4 9.6 9.8 10
0
2
4
6
North Ea
East MidYorkshir
South We
West Mid
North We
East of South Ea
Outer LoInner Lo

18
mean ln(outside wage)
AMI Rate AMI = 1.96*W -0.10W2
9.4 9.6 9.8 10
20
21
22
23
North EaEast Mid
Yorkshir
South We
West Mid
North We
East of
South Ea
Outer LoInner Lo
Higher death rate from AMI admissions in stronger labor markets (fig 7)

19
1. Models: What is the effect of pay regulation?
2. Empirical models
3. Data
4. Results
5. Conclusions
OUTLINE

20
2. Empirical Models
dit
di
di
dit
dOit
dit
dNURSESit
dPHYSit
dit zwwSSd 21
1. Hospital quality equation
For hospital i in year t:d = 30 day death rate from emergency AMI admission for 55+ year oldsSPHYS = share of clinical workforce who are physiciansSNURSES= share of clinical workforce who are nurses (and AHPs)(base group is health care assistants)wO = ln(outside wage)Z = controls for casemix, area mortality rates, hospital size, region dummies, etcw = ln(inside wage)η = hospital fixed effectτ = time dummies

21
itiiitOitit
NURSESit
PHYSitit zwwSSLY 21)/ln(
2. Hospital productivity equation
Ln(Y/L) = ln(Finished Consultant Episodes per clinical worker)SPHYS = share of clinical workforce who are physicians SNURSES= share of clinical workforce who are nurses (and AHPs)(base group is health care assistants)wO = ln(outside wage)Z = controls for casemix, area mortality rates, hospital size, area, etcw = ln(inside wage)η = hospital fixed effectτ = time dummies
22
Issues
• Unobserved heterogeneity: compare OLS, long differences and “System GMM”
• Endogeneity: – Outside wage: hospitals are a small % of local
labor market– Skill shares: GMM-SYS (Blundell-Bond,2000;
Bond and Soderbom, 2006)
• Standard errors allow for heteroscedacity, autocorrelation and clustering by region

23
1. Models: What is the effect of pay regulation?
2. Empirical models
3. Data
4. Results
5. Conclusions
OUTLINE

24
3. Data
• New hospital level panel data• 3 groups of clinical workers: Physicians, nurses
(AHPs) and Health Care Assistants. Total employment. From Medical Workforce Statistics
• Agency staff – hospital financial returns• Hospital quality: 30 day in-hospital death rates
for Emergency admissions for Acute Myocardial Infarction (AMI) for over 55 year olds. From HES (Hospital Episode Statistics).
• Productivity: Finished Consultant Episodes (HES) per worker

25
Casemix
• AMI – Do not have co-morbidity– Demographics of those admitted for AMI (14 gender
age-bands)– Control for hospital fixed effects– Mortality rate in area– Drop hospitals with under 150 AMI cases per year
• Productivity– 36 age-gender groups– Type of admission– Control for fixed effects– Experiment with conditioning on relative cost index

26
Wage Data
• Outside wage– New Earnings Survey (NES) 1% sample of all workers– Use travel to work area (100 in England)– Compare results with 9 main regions– Female non-manual wage – Robustness: all females, all non-manuals, average wage,
unemployment rates– Labor Force Survey (like CPS) “corrected” spatial wages taking
nurse characteristics into account
• Inside Wage– Average wage in hospital (but can just reflect grades)– Predicted wage based on NPRB regulation including regional
allowances (Gosling-Van Reenen, 2006)
27
Final Dataset
• 211 hospitals between 1996-2001
• 907 observations

28
1. Models: What is the effect of pay regulation?
2. Empirical models
3. Data
4. Results
5. Conclusions
OUTLINE

29
Dependent variable Ln(AMI Rate) Ln(AMI Rate) Ln(AMI Rate)
Estimation technique OLS Long Differences (3 years)
GMM-SYS
Ln (Area outside pay)
0.303**(0.150)
0.823**(0.381)
0.431**(0.188)
Physicians share -1.107***(0.359)
-2.198**(0.883)
-5.267**(2.753)
Nurses share -0.524*(0.276)
-1.435**(0.638)
-2.194*(1.262)
Hospital fixed effects No No Yes
No of Hospitals 211 211 211
Observations 907 348 907
Table 2: Death Rates from AMI
All columns include controls for area mortality rates, year dummies, casemix control, region dummies, hospital size (employment). HCA (Health Care Assistants) is base skill group

30
Magnitudes (col 3)
• From 90th to 10th percentile of area outside wage difference is a fall of 33%, associated with:– a 14% fall in death rates (a quarter of the 62%
90-10 spread)
• Increase in physician share from 10th to 90th percentile is 7 percentage points. Associated with– 37% fall in AMI death rates (60% of 90-10 diff)

31
Dependent variable Ln(Productivity) Ln(Productivity) Ln(Productivity)
Estimation technique OLS Long Differences (3 years)
GMM-SYS
Ln (Area outside pay)
-0.454***(0.159)
0.241(0.275)
-0.495**(0.230)
Physicians share 5.552***(0.434)
2.869***(0.507)
4.654***(0.905)
Nurses share 0.149(0.225)
1.071***(0.369)
1.523**(0.701)
Hospital fixed effects No No Yes
No of Hospitals 211 211 211
Observations 907 348 907
Table 3: Productivity (FCEs per employee)
All columns include controls for area mortality rates, year dummies, casemix control, region dummies, hospital size (employment). HCA is base skill group
32
Magnitudes
• From 90th to 10th of area outside wage difference is a fall of 33%, associated with:– a 16% increase in productivity (a quarter of
the 90-10 productivity difference)
• Increase in physician share from 90th to 10th is 7 percentage points– 35% increase in productivity (58% of the 90-
10 diff)

33
A possible mechanism: Agency nurses
• High outside wages associated with significantly greater use of agency staff
• Greater use of agency staff associated with lower hospital quality
• Quantitatively, agency staff appear to account for c.70% of the effect of outside wages on AMI death rates
• Agency staff also lowers productivity (maybe 10%+ of outside wage effect)

34
Dependent variable
Ln(Agency) Ln(AMI) Ln(AMI) Ln(AMI)
(1) (2) (3) (4)
Ln (Area outside pay)
2.557***(1.131)
0.423**(0.189)
0.131(0.254)
Ln(Agency) 0.091***(0.028)
0.076**(0.029)
SC(2) p-value
.132 .126 0.239 .180
Hansen-Sargan p-value
.390 .128 0.124 .161
Number of hospitals
177 177 177 177
Observations 523 523 523 523
Figure 5: Agency Nurses, outside wages and AMI death rates
All columns include all controls in Table 2 (skills, year dummies, casemix control, region dummies, area mortality, etc.). Estimation by GMM-SYS.

35
Dependent variable
Ln(Agency) Ln(productivity) Ln(productivity) Ln(productivity)
(1) (5) (6) (7)
Ln (Area outside pay)
2.557***(1.131)
-0.703**(0.232)
-0.622*(0.235)
Ln(Agency) -0.100***(0.031)
-0.046**(0.021)
SC(2) p-value
.132 .126 0.239 .180
Hansen-Sargan p-value
.390 .128 0.124 .161
Number of hospitals
177 177 177 177
Observations 523 523 523 523
Figure 5 – cont.: Agency Nurses, outside wages and Productivity
All columns include all controls in Table 2 (skills, year dummies, casemix control, region dummies, etc.)

36
Robustness (Table 6)
• Internal Market (pre-1997 more flexibility). Row 2• High outside wages implies higher costs (e.g.
rents), financial distress and worse outcomes. Row 3
• Not regulation? Houseman et al (2003) US case studies: (i) buffer, (ii) “hidden” monopsony, (iii) screening. BUT long-run effects in our data (figures and dynamics row 4)
• Model implies effects should be stronger in South – drop London (row 5)

37
Dependent variable Ln(AMI) Ln(Productivity)
1 Baseline 0.431**(0.187)
-0.495**(0.230)
2 “Internal market” period interaction with outside wageLinear outside wage
-0.222*(0.119)0.608***(0.204)
-0.133(0.092)-0.394*(0.229)
3 Include hospital financial surplus 0.397*(0.199)
-0.441**(0.250)
4 Include a lagged dependent variable: long-run effect [p-value]
0.506**[0.02]
-0.487**[0.045]
5 Drop Inner and Outer London 0.314*(0.174)
-0.375*(0.224)
6 Drop big jumps in outside wage 0.488**(0.227)
-0.549**(0.201)
7 Drop Regional Dummies 0.674***(0.207)
-0.428**(0.170)
8 Regional outside wage 1.352(1.104)
-0.429(0.598)
9 Regional outside wage (drop regional dummies)
0.735***(0.224)
-0.390**(0.167)
10 Include alternative total hospital employment measure
0.364**(0.178)
-0.383**(0.184)
Table 6: Robustness Checks

38
1. Models: What is the effect of pay regulation?
2. Empirical models
3. Data
4. Results
5. Conclusions
OUTLINE

39
Conclusions
• Regulated pay costs lives (and productivity) in high outside wage areas– Higher death rates (and lower productivity) in areas where labor
markets are tight– Much of this affect seems to operate through greater reliance on
temporary agency staff
• Also find that skill mix matters for hospital outcomes• Labor markets important for health on supply side of
medical care as well as demand side• Policy solution – allow wages to reflect local labor market
conditions?

40
Back Up Slides

41
Next Steps
• Policy simulations
• What is it about agency staff that is the problem?
• Other explanations – e.g. technology adoption (Acemoglu and Finkelstein, 2006)?

42
Dependent variable Ln(AMI) Ln(AMI) Ln(Productivity) Ln(Productivity)
Estimation technique
GMM-SYS GMM-SYS GMM-SYS GMM-SYS
Average inside wage
-0.240(0.188)
0.249**(0.096)
Predicted ln(inside wage using NPRB IV)
-0.693(1.113)
0.237(0.698)
Ln (Area outside pay)
0.427**(0.210)
0.449**(0.190)
-0.688***(0.216)
-0.476**(0.215)
Physicians share -4.096**(2.228)
-6.046**(2.336)
2.911***(1.008)
5.798**(1.002)
Nurses share -1.945*(1.153)
-2.375**(1.134)
-0.113(0.601)
1.579*(0.610)
No of Hospitals 211 211 211 211
Observations 706 706 706 706
Table 4: Inside Wage controls
All columns include controls for area mortality rates, year dummies, casemix control, region dummies, hospital size (employment). HCA is base skill group

43
Single Regulated Wage in areas of differential outside wage

44
Underlying structural model
• Hospitals choose mix of factors depending on environment and adjustment costs
• Factor with high adjustment costs changed more slowly
• Implies that lagged values predict future values• Empirical identification requires that adjustment
costs be sufficiently different across the factors to avoid weak instruments problems

45
System GMM
itititititit utaaxy ;
1) Difference equation eliminates firm fixed effects
0][ , itsti uxE
Moment conditions allow use of suitably lagged levels of the variables as instruments for the first differences (assuming levels error term serially uncorrelated, see Arellano and Bond, 1991)
Equation of interest
for s > 1 when uit ~ MA(0), and for s > 2 when uit ~ MA(1), etc.
Test assumptions using autocorrelation test and Sargan
Problem of weak instruments with persistence series…..

46
System GMM
2) Use lagged differences as instruments in the levels equationadditional moment conditions (Arellano and Bover, 1998; Blundell and Bond, 2000):
0)]([ , itisti uxE
Requires first moments of x to be time-invariant, conditional on common year dummies
Can test the validity of the additional moment conditions
We combine both sets of moments for difference and levels equations to construct “System GMM” estimator
We assume all firm level variables are endogenous, while industry level variables are exogenous in main specifications (relax in some specifications)
for s = 1 when uit ~ MA(0), and for s = 2 when uit ~ MA(1)
47
Alternative to regulation
• Avoiding permanent pay increases (Houseman et al, 2003)– Pay more observable than in US– Differences in pay and quality across regions
are persistent

48
Dependent variable Ln(Productivity) Ln(Productivity) Ln(Productivity)
Estimation technique GMM-SYS GMM-SYS GMM-SYS
Ln (Area outside pay/inside pay)
-0.586***(0.196)
-0.527*(0.270)
-0.491*(0.261)
Physicians share 3.683***(1.181)
4.107***(1.555)
5.068***(1.168)
Hospital fixed effects yes yes Yes
No of Hospitals 221 168 168
Observations 1013 406 406
Table A: Productivity (FCEs per employee) – Controlling for relative costs index
All columns include controls for nurses share, area mortality rates, year dummies (1999-2002), casemix control, region dummies, hospital size

49
Dependent variable Ln(Productivity) Ln(Productivity) Ln(Productivity)
Estimation technique GMM-SYS GMM-SYS GMM-SYS
Ln (Area outside pay)
-0.545***(0.186)
-0.575***(0.163)
-0.503*(0.143)
Ln (Inside pay) 0.585***(0.115)
0.195*(0.105)
Physicians share 4.252***(0.395)
Nurse share 0.620**(0.205)
No of Hospitals 211 211 211
Observations 706 706 706
Table B: Productivity (FCEs per employee) – Show effect of adding inside wageand skill mix sequentially
All columns include controls for nurses share, area mortality rates, year dummies (1999-2002), casemix control, region dummies, hospital size

50
Big spread in productivity between hospitals (Fig 3)
Note: productivity measured by finished consultant episodes per worker

51
Mean Standard deviation
Min Max
AMI Variables
AMI death rate (55 plus) 21.125 4.520 2.964 36.941
Total AMI deaths (55 plus) 7993.624 3382.425 1100 29400
Total AMI admissions (55 plus) 384.958 160.261 151 1348
Productivity and FCE (finished Consultant Episodes)
Productivity (total FCEs/ total staffing) 30.981 7.718 5.094 65.121
Total FCEs 58,620.82 2,441.15 13,490 138,984
Staffing Variables
Total staffing (physicians+nurses+AHP+Health Care Assistants)
1909.447 774.049 432.9 4269.83
Physicians share of staffing 0.130 0.030 0.047 0.249
Nurses (plus qualified Allied Health Professionals) share of staffing
0.646 0.034 0.493 0.765
Hospital Expenditure Variables
Share of expenditure on Agency staff as a proportion of total expenditure
0.035 0.028 0.001 0.163
Wage Variables
Ln(Area outside wage) 9.602 0.141 9.272 9.987
Ln(Predicted NPRB wage) 9.711 0.088 9.558 9.991
Table 1: Descriptive Statistics