
1 BPA and conjugated -BPA: Pharmacokinetics across species Pierre-Louis Toutain National Veterinary...
76
1 BPA and conjugated -BPA: Pharmacokinetics across species Pierre-Louis Toutain National Veterinary School of Toulouse, France NIEHS BPA Grantee research Meeting January 28-29,2013 Research Triangle Park, North Carolina, USA.
-
Upload
buck-glenn -
Category
Documents
-
view
214 -
download
0
Transcript of 1 BPA and conjugated -BPA: Pharmacokinetics across species Pierre-Louis Toutain National Veterinary...

1
BPA and conjugated -BPA: Pharmacokinetics across species
Pierre-Louis ToutainNational Veterinary School of Toulouse, France
NIEHS BPA Grantee research MeetingJanuary 28-29,2013
Research Triangle Park, North Carolina, USA.

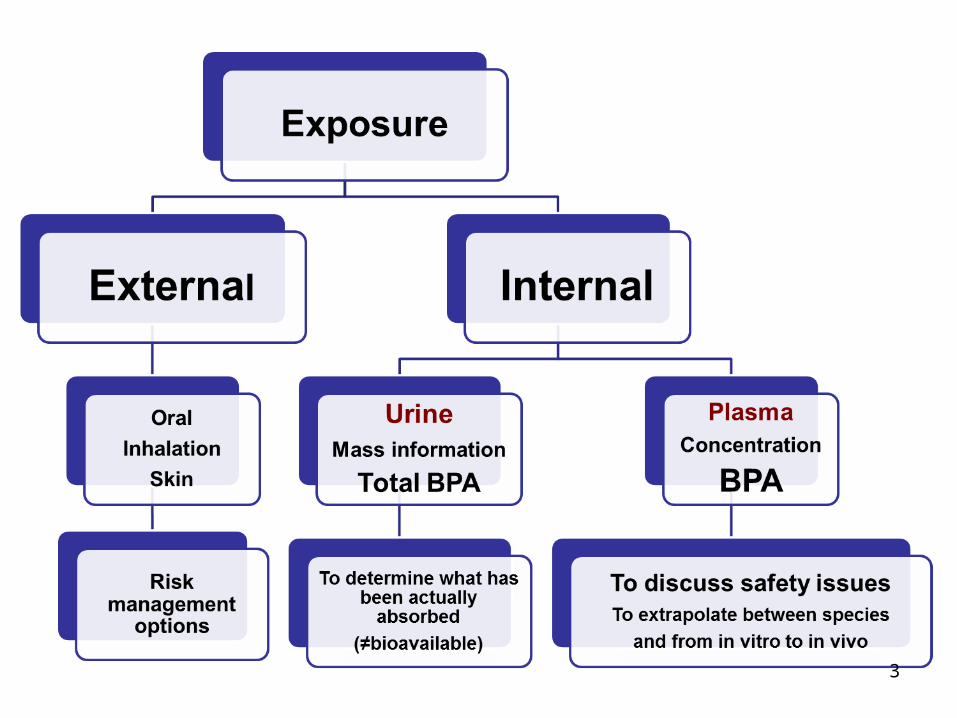
Goal of the presentation
• How PK data across different animal species can contribute to predict and understand the internal exposure to the bioactive form of BPA in humans
2
3

4
A fundamental relationship
• This relationship is not a model but results of definitions:– For a linear kinetic , clearance is a scaling parameter
between a dose and plasma concentration
• This relationship is not a model but results of definitions:– For a linear kinetic , clearance is a scaling parameter
between a dose and plasma concentration

Body (plasma, blood) clearance
• The most important PK parameter
• Unknown in man
• Should be estimated by a modeling approach
5

6
The most simple model for Interspecies extrapolation
The most simple model for Interspecies extrapolation
Allometric relationshipL
og
par
amet
er
Log BWLogBWbaLogY

Allometric estimation of plasma clearance in man
7Cho et al 2002 Xenobiotica 32 925-934
30mL/kg/min30mL/kg/min
Doerge et al 2012 Tox letters
About 23.8 mL/kg/minAbout 23.8 mL/kg/min

Man
ClBPA = 24.7 mL/(kg.min)
or 103L/h for a 70kg BW
Prediction interval [9.3-66.0]
Allometric estimation of plasma clearance in man
0.0001
0.001
0.01
0.1
1
10
0.01 0.1 1 10 100 1000
Body weight (kg)
BP
A c
lear
ance
(L/
min
)
ClBPA (L/min)=0.0440 x BW0.8645
8Collet et al Unpublished results

An order of magnitude for BPA plasma clearance in man is of 25ml/kg/min
9
• Q2: is it a high or low clearance?

10
Physiological Interpretation of BPA body clearance
• Interpretation of body clearance consists of calculating an overall extraction ratio

11
Physiological Interpretation of BPA body clearance
• Interpretation of body clearance consists of calculating an extraction ratio
An extraction ratio of 0.31 is high(typical value for drugs is <0.05)
An extraction ratio of 0.31 is high(typical value for drugs is <0.05)
What is the origin of this high plasma clearance and why this
question?
• High Hepatic or high renal clearance?
• If BPA has a high hepatic clearance, a low bioavailability is expected for the oral route (gavage)
12

Clearances are additive
• Theoretically very easy to determine without BPA administration;
Negligible
To predict the maximal oral bioavailabilityTo predict the maximal oral bioavailability

Renal clearance of BPA is very low
Renal clearance was less than 1% in the 5 investigated species after an IV
administration
Renal clearance was less than 1% in the 5 investigated species after an IV
administration

Hepatic BPA clearance in man: in vitro estimation
Clh was estimated at 22 mL/kg/min in humans i.e. to exactly the same value as
from allometry.

Interpretation of a high hepatic clearance to predict
the extent of an hepatic first-pass effect and of a maximal possible oral bioavailability
16

The hepatic portal system
17

GutLumen
Gut WallPortalvein
To site of measurement
BPA Gut wall Metabolism: BPA Gut wall Metabolism:
Hepatic Metabolism
To feces
Presystemic metabolismFirst pass effect
(oral route)
LiverLiver
YESYESNONO

Fmax = 1 - EhFmax = 1 - Eh
Liver
Fmax = 1 - Eh
Fraction of the dose that is absorbed
Fraction of the dose that is absorbed
Eh
Fraction eliminated by a first pass effect
BPA absorption, first pass effect and bioavailability for the oral route
Fraction non absorbed
GIT
BPA

Maximal oral bioavailability (Fmax)
Hepatic first-pass effect

Bioavailability of BPA across species
• BPA IV: 5mg/kg; BPA oral: 100 mg/kg• Simultaneous BPA and BPA-G quantification in plasma and in urine samples were
performed with an Acquity ultra performance liquid chromatography (UPLC®) coupled to a Xevo triple quadrupole mass spectrometer (Waters, Milford, MA, USA) (Lacroix et al 2011).
• LOQ of BPA from 1 10 ng/mL in plasma and 10 to 25 ng/mL in urine• Data analysis: NCA
21
4.1% 1.3%0.6%0.9%
Collet et al unpublished results

Estimation the oral bioavailability of BPA in rhesus monkey (data from Doerge et al 2010)
22
Both IV and oral data
F%=0.9±0.58%F%=0.9±0.58%

BPA bioavailability vs. absorption

Bioavailability vs. absorption
• Absorption: movement of drug from the site of administration into the blood which drains the site of administration
• Bioavailability refers to the amount of drug which actually gains the access to the systemic (arterial) circulation

Why it is important to assess the extent of oral BPA absorption?
• To validate that the urinary data can be used to estimate the BPA daily intake of BPA

Computation of the absorbed fraction vs. the bioavailability
26
Assuming that the drug is only eliminated hepatically (i.e. that there is no or minimal renal elimination of the parent substance as for BPA) the fraction of drug that is absorbed is uniquely determined by the AUC ratio of metabolite

Absorbed fraction of BPA after an oral administration across species
• BPA IV: 5mg/kg; BPA oral: 100 mg/kg• Simultaneous BPA and BPA-G quantification in plasma and in urine samples were
performed with an Acquity ultra performance liquid chromatography (UPLC®) coupled to a Xevo triple quadrupole mass spectrometer (Waters, Milford, MA, USA) (Lacroix et al 2011).
• LOQ of BPA-G from 20 to 50 ng/mL in plasma and of 1000ng/mLin urine• Non Comp analysis (sheep, pig, dog) and comp modeling (rat, mouse)
27
98 75.6763.798.4
Collet et al unpublished results

Absorbed fraction of BPA after an oral administration in man
• Human subjects were orally administered d-6-bisphenol A (5 mg in toto).
• d16-Bisphenol A glucuronide was the only metabolite of d16-bisphenol A detected in urine and blood samples, and concentrations of free d16-bisphenol A were below the limit of detection both in urine (6 nM) and blood samples (10 nM).
• The applied doses were completely recovered in urine as d16-bisphenol A glucuronide.
What are the predicted plasma concentrations of BPA in the general
population: a Monte Carlo Simulation
29

30
What are the plasma concentrations of BPA in the general population

Pg/mL
31Average daily intake: about 0.05µg/kg/dayAverage daily intake: about 0.05µg/kg/day

• From allometry: 24.7±4.94ml/kg/min
F from 1 to 5%
The 2005–2006 National Health andNutrition Examination Survey (NHANES) were used to estimate daily BPA intakes

Plasma BPA concentrations (pg/ml)Monte Carlo Simulation
33Average plasma concentration: 0.12pg/mL; percentile 90: 0.26pg/mL or 1.1pM Average plasma concentration: 0.12pg/mL; percentile 90: 0.26pg/mL or 1.1pM

Predicted plasma BPA concentrations in the US population: a sensitivity analysis
• Daily intake is the most influential variable in the prediction of plasma BPA level.
• And Plasma clearance the less influential
34

IV Plasma clearance variability
• Many possible factors of variability
• No population information but intersubject variability cannot generate a difference of several order of magnitude between subjects
– An example: effect of obesity
35
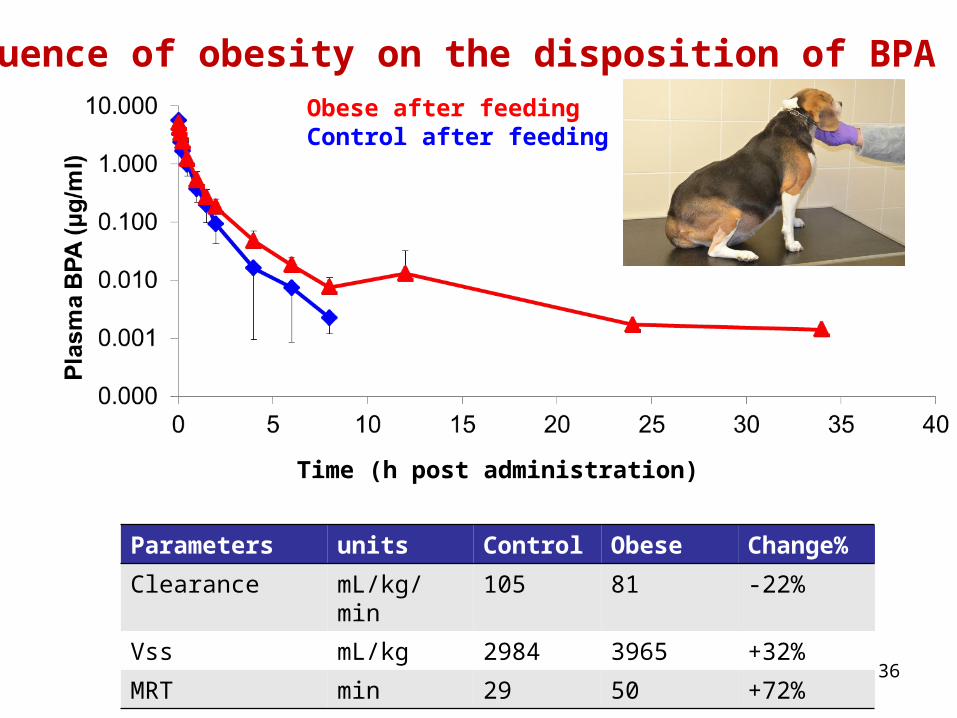
Time (h post administration)
Influence of obesity on the disposition of BPA
36
Obese after feedingControl after feeding
Parameters units Control Obese Change%
Clearance mL/kg/min 105 81 -22%
Vss mL/kg 2984 3965 +32%
MRT min 29 50 +72%

Are we sure of a systematic low oral bioavailability in man?
• A low oral bioavailability has been actually measured in all investigated species
• But BPA is generally administered by gavage allowing a full first-pass effect .
• A low oral bioavailability has been actually measured in all investigated species
• But BPA is generally administered by gavage allowing a full first-pass effect .
37
• This is the first report of serum BPA concentrations in an animal model exposed to BPA via the diet.
• Bolus administration underestimates bioavailable serum BPA concentrations in animals—and presumably humans—than would result from dietary exposure.
• Exposure via diet is a more natural continuous exposure route than oral bolus exposure and is thus a better predictor of BPA concentrations in chronically exposed animals and humans.
Environ Health Perspect 119:1260–1265 (2011).

The 3 segments of the digestive tract in terms of first-pass effect
38
Buccal cavityNo
first-passeffect
Small intestine/large bowelFull First pass-effect
Rectal Limited first-pass effect
Rectal Limited first-pass effect

Buccal/Sublingual administration to bypass the
hepatic first-pass effect?

Buccal/Sublingual absorption
• sublingual (SL) = under tongue
The surface area of the oral mucosa (200 cm2) is relatively small compared with the gastrointestinal tract (350 000 cm2) and skin (20 000 cm2).

• Scintigraphic imaging revealed that clearance of the formulation from the oral cavity was rapid, with a mean T50% clearance of 0.86±0.46 min, and T80% clearance of 2.75±1.52 min
41

42

Selection of an animal model:Keratinized vs. non-keratinized oral mucosa
• Non keratinized oral mucosa:– dogs, rabbits, pigs, and Rhesus monkeys are
acceptable models, yielding permeability values similar to those found for humans.
• Keratinized oral mucosa– Pose a significant barrier to intra-oral absorption that
impact its correlation to that in humans. – the heavily keratinized rat or hamster oral mucosa tends
to underestimate absorption from the non-keratinized human oral mucosa.
43
No
Yes

The dog was selected as a model• 6 beagle dogs • Routes of administration: IV, sublingual and gavage• Dose tested: high (5mg/kg) in ethanol and low (50µg/kg)
with water as vehicle delivered over 10 mins towards the floor of the mouth
• Sampling at the jugular vein
44

BPA 0.05mg/kgBPA 5mg/kg
Time (min post administration)
Results for a representative dog
45Sublingual # IVSublingual # IV

Time post administration (min)
Pla
sma
BP
A (
ng
/ml)
46
Results for the 6 dogs
Sampling at the jugular vein
For a dose of 1µg/kg, plasma concentration should be about 1ng/mLFor a dose of 1µg/kg, plasma concentration should be about 1ng/mL

Bioavailability of BPA by sublingual administration
Oral20mg/kg
Sublingual5mg/kg
Sublingual50µg/kg
Bioavailability %(from BPA AUCs)
0.72±0.28
81± 29
>100%
Absorption%(From BPA-gluc
AUCs)
54±19
81±18
90±26
47

The concentration ratio of BPAG to BPA in plasma:
IV, sublingual or oral administration
• The concentration ratio of BPAG to BPA in plasma was approximately 100-fold lower following sublingual administration than after oral dosing allowing to easily distinguishing the two pathway of absorption.
48
IV
SL
ORAL
30 min post ad30 min post ad

Buccal exposure
49
Crown restoration of a molar may release 13µg BPA in the average case scenario or 30mg BPA in the worst case scenario both after 24h
Crown restoration of a molar may release 13µg BPA in the average case scenario or 30mg BPA in the worst case scenario both after 24h
BPA was found in all paper currencies at concentration ranging up to 82.7µg/g
BPA was found in all paper currencies at concentration ranging up to 82.7µg/g

Hand-to-Mouth exposure
• Average indoor hand-to-mouth behavior ranged from 6.7 to 28.0 contacts/hour,
– with the lowest value corresponding to the 6 to <11 year olds and the highest value corresponding to the 3 to <6 month olds.
• Average outdoor hand-to-mouth frequency ranged from 2.9 to 14.5 contacts/hour,
– with the lowest value corresponding to the 6 to <11 year olds and the highest value corresponding to the 6 to<12 month olds.
50

51
Half-life
BPA Systemic exposure
BPA Systemic exposure
ClearanceVolume of distribution
bioavailability
Absorption
BPA accumulation
BPA accumulation

60 daily SQ administrations of BPA to pregnant ewes (5mg/kg/day does not lead to BPA or BPA-Gluc accumulation
BPA and BPA-gluc disposition : Time dependency
Viguie et al
No evidence of accumulation

53
The case of the very late terminal phase: an issue for the question of a possible BPA
bioaccumulation in a (small) deep compartment
In case of a very late terminal phase , bioaccumulation can occur in a deep compartment while plasma concentration
profile remains unchanged
In case of a very late terminal phase , bioaccumulation can occur in a deep compartment while plasma concentration
profile remains unchanged
Very late terminal phase Very late terminal phase
Bioaccumulation due to the very late terminal phase
Bioaccumulation due to the very late terminal phase

BPA distribution: the case of fetus
54
24 IV infusion of BPA 2 mg/(kg.d)
Analytical technic measuring selectively BPA, BPA-G and BPA-S

PLACENTAPLACENTA
Materno-fetal transfer of BPA
2%
98%98%
BPA-G and BPA-S trapped in amniotic fluid
BPA Internal (blood) Exposure:
40 ng/mL
BPA Internal (blood) Exposure:
6 ng/mL
24 IV infusion of BPA 2 mg/(kg.d)
Fetal CompartmentMaternal Compartment
As in man, BPA exposure lower in fetus than in mother but higher exposure for BPA-G in the fetus

PLACENTAPLACENTA
Feto-maternal transfer of BPA
91%
9%
BPA-G and BPA-S trapped in amniotic fluid
Total BPA Clearance :
250 mL/(kg.min)
BPA Internal Exposure: 4 ng/mL
BPA Internal Exposure: 25 ng/mL
24 IV infusion of BPA 5 mg/(kg.d)
Fetal CompartmentMaternal Compartment
Placenta eliminated 90% of fetal BPAPlacenta eliminated 90% of fetal BPA

PLACENTAPLACENTA
Feto-maternal transfer of BPA-G (120 days)
BPA-G Internal Exposure: 4530 ng/mL
IV infusion of BPA-G 3.54 mg/(kg.d)
BPA-G?
Fetal CompartmentMaternal Compartment
BPA was never detected (LOQ=1ng/mL)
BPA and BPA-G never detected
No reactivation of BPA-G into BPA observed despite a very high dose
of infused BPA-G in the fetus

Principles to extrapolate results (effects) between species
58

The question of the safe dose in man should be established and discussed through the determination
of a safe plasma concentration
59
Toxicokinetics (satellite groups) is in orderToxicokinetics (satellite groups) is in order
Range1/1000Range1/1000 Range1/2Range1/2

60
Same profile (CL/F similar) but both plasma clearance and F are higher in mouse than in monkey (X3-4)

Comparison of effective plasma concentrations in different species
• Only free plasma concentration is active
• Plasma protein binding is a factor of confusion
61Fu is the confounding factor (0.06 in man; 0.05 in sheep; 0.1 in lamb fetus) Fu is the confounding factor (0.06 in man; 0.05 in sheep; 0.1 in lamb fetus)

The dose effect relationship and PKPD consideration
62

What is the shape of the dose-effect relationship for BPA?
• [Drug] 63
Res
po
nse

What is the shape of the dose-effect relationship
64

Conclusion
65

Thanks for your attentionThe BPA team
V.Gayrard
N Hagen C Viguié M. Lacroix & S.Puel
S.Collet & T.Corbel

Answers to 10 questions
67

Q1:what we really know and don’t know: Plasma clearance
– We have no direct measurement of plasma BPA clearance but only indirect estimates (allometry).
– BPA body clearance is (very) high.• We ignore population distribution of this parameter
(subpopulations?)
– We know that the renal BPA clearance is very low
– BPA clearance is mainly hepatic• Thus a high first-pass effect is expected for the
oral route (gavage)
68

Q2:what we really know and don’t know:
Absorption & bioavailability
• Extent of oral absorption is high but bioavailability (different of absorption) for oral route (gavage) is (very) low– Sublingual route of BPA absorption escape to
a the hepatic first-pass effect and can lead to relevant BPA plasma concentrations
– Rodents are not a good model for sublingual absorption
69

Q3:what we really know and don’t know:
half-life • Currently, reported BPA half-life is short thus no
accumulation possible – No experimental evidence of BPA accumulation in sheep
• However a very late terminal phase cannot be exclude (it is a question of LOQ) with an accumulation in a deep compartment without alteration of BPA plasma concentration
70

Q4:what we really know and don’t know:
linearity
• BPA and BPA-gluc disposition are linear (dose proportionality)– Possibility to extrapolate between doses for
exposure
• No time dependency
71

Q5:what we really know and don’t know: Plasma concentration
• Plasma concentration is the driving force controlling biophase (receptors) concentrations
• With the current available data (a high plasma clearance, a low oral bioavailability and a low daily intake), predicted plasma concentration should be very low (less than 1pg/mL).
72
If plasma concentration can actually reach few ng/mL (no contamination) , one or several of the aforementioned statements is (are) totally wrong
If plasma concentration can actually reach few ng/mL (no contamination) , one or several of the aforementioned statements is (are) totally wrong

Q6: Are humans really different from other species (rodents) with regard to pharmacokinetics and
metabolism
• No qualitative relevant differences– Allometric law apply
– The case of enterohepatic recycling in rodents
• Some quantitative differences
73
All species and all route of BPA administration can provide relevant results to discuss systemic effects in man as long as plasma concentrations
in the test system are monitored and used to bridge results with the human plasma exposure
All species and all route of BPA administration can provide relevant results to discuss systemic effects in man as long as plasma concentrations
in the test system are monitored and used to bridge results with the human plasma exposure

Q8: Can one really use a urine measurement to develop a PK model of
what the human exposure is?
• Yes.
• Urine is the main pathway of BPA-conjugates elimination in man
• Urine information is a mass information and mass balance concepts apply (determination of the daily BPA absorbed (not bioavailable) dose.
74

Q9:Value of biomonitoring data
• How to explain that several studies using a variety of different analytical technique have measured free, unconjugated BPA concentration in humam serum at levels ranging from 0.2 to 20ng/mL?– Analytical bias that overestimate BPA in
plasma ?– Biomonitoring (sampling conditions) bias that
underestimate total BPA in urine?
75

Q10: If data doesn’t match the model which do you throw out…the data or
the model?
• The model should be rejected
• But– A sound model can help to detect flawed data
(bad analytical technics), unplausible results etc
• Quotes by Box: ‘all models are wrong; the practical question is how wrong do they have to be to not be useful’.
76


















