
1 ANTIFUNGAL THERAPY IN FEBRILE NEUTROPENIC PATIENTS REVIEW OF TREATMENT CHOICES AND STRATEGIES Jean...
56
1 ANTIFUNGAL THERAPY IN ANTIFUNGAL THERAPY IN FEBRILE NEUTROPENIC FEBRILE NEUTROPENIC PATIENTS PATIENTS REVIEW OF TREATMENT REVIEW OF TREATMENT CHOICES CHOICES AND STRATEGIES AND STRATEGIES Jean KLASTERSKY, M.D., Ph. D. Institut Jules Bordet, Brussels, Belgium
-
Upload
sheldon-hackman -
Category
Documents
-
view
216 -
download
1
Transcript of 1 ANTIFUNGAL THERAPY IN FEBRILE NEUTROPENIC PATIENTS REVIEW OF TREATMENT CHOICES AND STRATEGIES Jean...

1
ANTIFUNGAL THERAPY IN ANTIFUNGAL THERAPY IN FEBRILE NEUTROPENIC FEBRILE NEUTROPENIC
PATIENTS PATIENTS REVIEW OF TREATMENT REVIEW OF TREATMENT
CHOICESCHOICES AND STRATEGIES AND STRATEGIES
Jean KLASTERSKY, M.D., Ph. D.
Institut Jules Bordet, Brussels, Belgium

2G.S. MARTIN et al., NEJM 2003

3
Mc Neil M, CID 2001;13:;641-647

4
Frequency of non-Aspergillus mould infections at Fred-Hutchinson Cancer Research Center (Seattle). The number of patients who developed proven or probable infection with Fusarium species, Zygomycetes and Scedosporium species from 1985 through 1999 are shown
0
2
4
6
8
10
12
14
16
1985-1989 1990-1994 1995-1999
Scedosporium speciesZygomycetesFusarium species

5
0
10
20
30
40
50
60
70
C.alb C.trop C.glab C.krus C.parap C.guil C.lusit other
Est OuestPathogenic Candida species in BMT recipients : Candida species that caused candidemia arecompared over 2 decades at the Fred Hutchinson Cancer Research Center. The incidence ofcandidemia decreased from 11.4 % in 1980-1986 (72) compared to 4.6 % after adoption offluconazole for prophylaxis (1984-1997).
Marr K & Bowden R, Transplant Infectious Diseases 1999;1:237-246.

6
Antifungal prophylaxis in leukemia patients :
ECIL recommendations

7
Comparative trials of antifungal agents in candidemia and invasive candidasis
Response rate Overall mortality
Fluconazole vs amphotericin B 70 % vs 79 % 33 % vs 40 %
Itraconazole vs amphotericin B 35 % vs 41 % 40 %
ABLC vs amphotericin B 63 % vs 68 % 41 % vs 39 %
Caspofungin vs amphotericin B 73 % vs 62 % 30 % vs 34 %
Voriconazole vs amphotericin B 41 % vs 41 % 36 % vs 42 %
Micafungin vs Ambisome 89 % vs 89 %
Anidulafungin vs fluconazole 75 % vs 60 % 26 % vs 31 %

8
Why does the frequency of fungal infection increase ?
I.V. devices Immunosuppression Neutropenia Broad spectrum antibiotics Diabetes

9
Rational for Empirical Antifungal Therapy inRational for Empirical Antifungal Therapy inNeutropenic Patients with Persistent FeverNeutropenic Patients with Persistent Fever
Early diagnosis of many fungal infections is difficult
Delayed treatment increasesmortality
Success of antibacterialempirical therapy

An Algorithm for Therapy of Febrile Neutropenia after Initial An Algorithm for Therapy of Febrile Neutropenia after Initial Empirical Therapy with Broad Spectrum AntibioticsEmpirical Therapy with Broad Spectrum Antibiotics
Follow Daily And Reassess After 72 Hours
Clinical response
Yes No
Pathogen isolated
Adjust to sensitivity
Look for localized infection
Use G/GM-CSF?
Continue for 7 days
Repeat cultures and serologyPerform chest CT and BAL
Add amphotericin, and possibly metronidazole, antivirals and/or G/GM-CSF as indicatedLook for non infectious causes of fever
Yes No
10

11
Possible Causes of Persistent FeverPossible Causes of Persistent FeverApproximate Approximate frequency in frequency in high risk high risk patients (%)patients (%)
Fungal infections susceptible to empirical therapy 40
Fungal infections resistant to empirical antifungal therapy 5
Bacterial infections (with cryptic foci and resistant organisms) 10
Toxoplasma gondii, mycobacteria, or fastidious pathogens (legionella, mycoplasma, chlamydia, bartonella)
5
Viral infections (cytomegalovirus, Epstein-Barr virus, human herpes virus 6, varicella-zoster virus, herpes simplex virus) and respiratory pathogens such as parainfluenza virus, respiratory syncytial virus, influenza viruses
5
Graft-versus-host-disease after hematopoietic stem-cell transplantation
10
Undefined (e.g. drug fever, toxic effects of chemotherapy, antitumor responses, undefined pathogens)
25
L. COREY and M. BOECKH, NEJM 2002

12

13

14
Infectious Complications in Each of the Groups Infectious Complications in Each of the Groups Following RandomizationFollowing Randomization
Randomization group
N°Clinically documented
Bacterial FungalViral Protozoal
Shock
Discontinue KGC 16 2 3 1 0 6
Continue KGC alone
16 0 1 5 0 0
KGC + Ampho B 18 0 0 1 1 0
P.A. PIZZO et al, Am J Med 1982KGC : cephalotin (Keflin), gentamicin, carbenicillin
14

15
Clinical Response Clinical Response in Persistently (4 days) Febrile in Persistently (4 days) Febrile Neutropenic PatientsNeutropenic Patients
Ampho B No Ampho B p Value
Overall
All patients 55/80 (68) 39/77 (50) 0.10
Prior antifungal prophylaxis
No 21/27 (78) 9/20 (45) 0.04
Yes 19/31 (61) 24/39 (61) NS
Infection documentation
Clinical 22/29 (75) 14/31 (41) 0.03
Possible 25/39 (64) 20/33 (60) NS
Granulocyte count at Day 4
< 100/µL 31/45 (69) 20/43 (46) 0.06
100-500/µL 16/23 (70) 14/21 (67) NS
EORTC-IATCG, Am J Med 1989
16
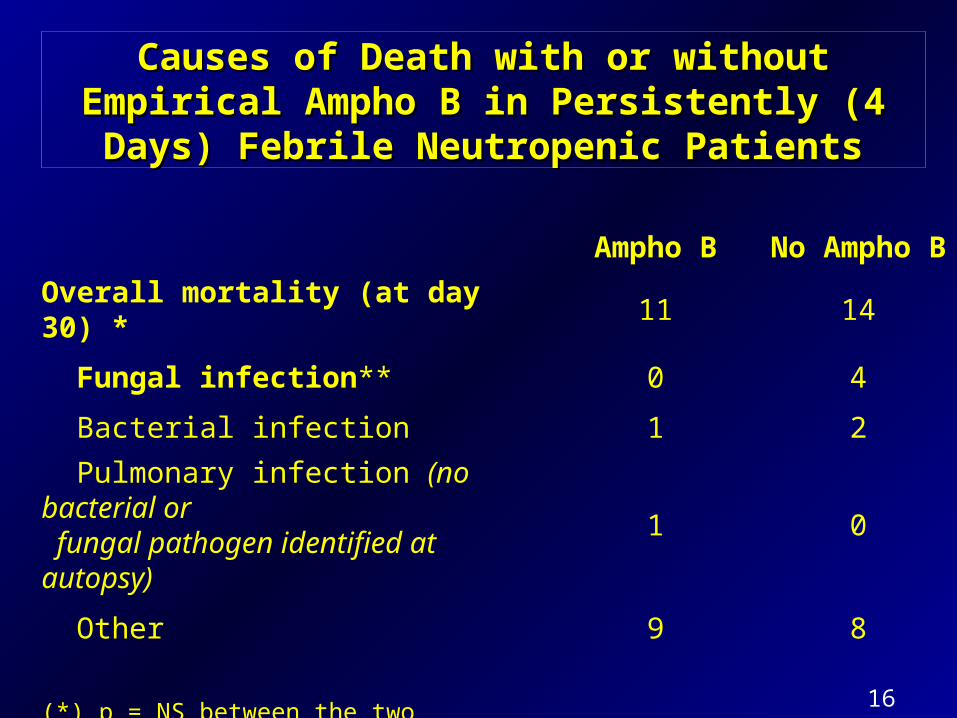
Causes of DeathCauses of Death with or without Empirical Ampho B with or without Empirical Ampho B in Persistently (4 Days) Febrile Neutropenic Patientsin Persistently (4 Days) Febrile Neutropenic Patients
Ampho B No Ampho B
Overall mortality (at day 30) * 11 14
Fungal infection** 0 4
Bacterial infection 1 2
Pulmonary infection (no bacterial or fungal pathogen identified at autopsy)
1 0
Other 9 8
(*) p = NS between the two groups(**) p = 0.05 between the two groups
EORTC-IATCG, Am J Med 1989

17
Randomized Studies Comparing Empirical Treatment with Randomized Studies Comparing Empirical Treatment with Antifungal Agents for Persisting Fever during NeutropeniaAntifungal Agents for Persisting Fever during Neutropenia
YEAR STUDY ANTIFUNGAL AGENTS COMPARED
1982
1989
1996
1998
1998
1999
2000
2000
2001
2002
2004
Pizzo et al
EORTC
Viscoli et al.
Malik et al.
White et al..
Walsh et al.
Winston et al.
Wingard et al.
Boogaerts et al.
Walsh et al.
Walsh et al.
Conventional ampho B vs no antifungal therapy
Conventional ampho B vs no antifungal therapy
Conventional ampho B vs fluconazole
Conventional ampho B vs fluconazole
Conventional ampho B vs ampho B colloidal dispersion
Conventional ampho B vs liposomal ampho B
Conventional ampho B vs fluconazole
Liposomal ampho B vs ampho B lipid complex
Conventional ampho B vs itraconazole
Liposomal ampho B vs voriconazole
Liposomal ampho B vs caspofungin

18
Measures of the Success (%) of Empirical Antifungal Therapy with Measures of the Success (%) of Empirical Antifungal Therapy with Conventional or Liposomal Amphotericin B, Voriconazole or Conventional or Liposomal Amphotericin B, Voriconazole or
CaspofunginCaspofungin
Ampho B Liposomal Ampho B Voriconazole Caspofungin (Ampho B) (Vori) (Caspo)
N° of patients 344 343 422 539 415 556
Overall success 49.4 50.1 30.6 33.7 26.0 33.9
Resolution of fever 58.1 58.0 36.5 41.4 32.5 41.2
No breakthroughfungal infection 89.2 90.1 95.0 95.5 98.1 94.8
Resolution ofbaseline infection 72.7 81.8 66.7 25.9 46.2 51.9
Survival for 7 day 89.5 92.7 94.1 89.2 92.0 92.6
No discontinuationNo discontinuationfor toxic effectsfor toxic effects 81.481.4 85.7 93.4 85.5 85.7 93.4 85.5 90.1 89.7 90.1 89.7 or lack of efficacyor lack of efficacy
J. KLASTERSKY, NEJM 2004

19
Comments on the Walsh’s studies
Large prospective controlled trials Composite score : « common language » BUT
– Survival and fever can be influenced by many other factors than just the nature of the empirical regimen
– What is the difference between « baseline » FI (<72h) and « breakthrough » FI (>72h) ?
– Discontinuation for toxicity or lack of efficacy :
« mixing apples and pears » ?

20
Toxicity of Empirical Antifungal Therapy %
Conventional amphotericin
Liposomal amphotericin
Voriconazole Caspofungin
Total n° patients 344 1312 415 564
Chills
Nephrotoxicity*
54
34
24
13
13
7
14
3
Discontinuation for toxicity
18 9 5** 5
* Creatinine increase 2 x base line ** Visual hallucinations more frequent with voriconazole (4.3 % vs 0.5 %)

21
Measures of the Success (%) of Empirical Antifungal Therapy with Measures of the Success (%) of Empirical Antifungal Therapy with Conventional or Liposomal Amphotericin B, Voriconazole or Conventional or Liposomal Amphotericin B, Voriconazole or
CaspofunginCaspofungin Ampho B Liposomal Ampho B Voriconazole
Caspofungin (Ampho B) (Vorico) (Caspo)
N° of patients 344 343 422 539 415 556
Overall success 49.4 50.1 30.6 33.7 26.0 33.9
Resolution of fever 58.1 58.0 36.5 41.4 32.5 41.2
No breakthroughNo breakthroughfungal infectionfungal infection 89.2 90.1 95.0 95.5 89.2 90.1 95.0 95.5 98.1 98.1 94.8 94.8
Resolution ofResolution ofbaseline infectionbaseline infection 72.772.7 81.8 66.7 25.9 81.8 66.7 25.9 46.2 46.2 51.9 51.9
Survival for 7 day 89.5 92.7 94.1 89.2 92.0 92.6
No discontinuationfor toxic effects 81.4 85.7 93.4 85.5 90.1 89.7 or lack of efficacy
J. KLASTERSKY, NEJM 2004

22
Cure of Base Line Fungal InfectionCure of Base Line Fungal Infection
Conventional ampho B
Liposomal ampho B
Voriconazole Caspofungin
Total n° of patients
344 961* 415 556
Response/n° (%)
8/11
(72.7)
20/44 (45.4)**
6/13
(46.2)
14/27
(51.9)
* 2 studies**Outcome in the study comparing conventional ampho B to liposomal ampho B was 9/11 (81.8)

23
Choice of a suitable denominator for the evaluation of empirical therapy based on microbiological results
(T. Walsh) (J. Klastersky)
Success of therapy Failure of therapy
No breakthrough FI Total n° patients -
Cure of baseline FI N° of baseline FI -
Breakthrough FI - Total of n° of patients
No cure of baseline FI - Total of n° of patients

24
Outcome of Empirical Antifungal Therapy in Outcome of Empirical Antifungal Therapy in Microbiologically Demonstrated Fungal InfectionsMicrobiologically Demonstrated Fungal Infections (FI) (FI)
Ampho B Liposomal ampho B
Voriconazole Caspofungin
(344) (961) (415) (556)
Breakthrough FI 37 (10.8) 45 (4.6) 8 (1.9) 29 (5.2)
No cure of base line FI 3 (0.8) 22 (2.2) 7 (1.6) 13 (2.3)
Total failures* 40 (11.6) 67 (6.9 %) 15 (3.6 %) 42 (7.7 %)
*p = 0.03

25
Summary of trials of empirical antifungal therapy that evaluated alternatives to amphotericin B
Study drugs % of invasive fungal infections
n Arm 1 Arm 2 Arm 1 Arm 2
687 AmB L-Amb 8.7 5.0
384 AmB Itraconazole 2.7 2.7
837 L-AmB Voriconazole 5.0 1.9*
1095 L-AmB Caspofungin 4.3 5.2
* p< 0.5J.R. Wingard, CID, 2004

2626

27Aspergillus fumigatus

28

29
Galatomannan detection for the diagnosis of Galatomannan detection for the diagnosis of invasive aspergillosisinvasive aspergillosis
Approved by FDA; standard : optical density index > 0.5 in 2 consecutive samples ?
Positivity can preceed radiological findings In probable or proven cases levels are often higher and
increase within days 81 % sensitivity; 89 % specificity; NPV:98 %; PPV:7-94 % False negatives : prophylactic use of mold-active
azoles, early antifungal therapy and others ? False positives : use of piperacillin-tazobactam and others ?

30
AspergillusAspergillus Infections (AI) in Empirical Therapy Infections (AI) in Empirical Therapy
Liposomal ampho B
Voriconazole Caspofungin
(961) (415) (556)
Breakthrough AI 21 4 10
No cure of base line AI° 13* 4** 7
Total failures 24 (2.4 %) 8 (1.9 %) 17 (3.0 %)
° Assuming that 1/2 infections in the liposomal ampho B arm (*) and4/7 infections in the voriconazole arm (**) were caused by Aspergillus

31R. Herbrecht et al, N Engl J Med, 2002

32T.J. Walsh et al, N Engl J Med 2002 1.9 % 4.9 % (p = 0.02)

33T.J. Walsh et al, N Engl J Med 2004

34T.J.Walsh et al, N Engl J Med 2004
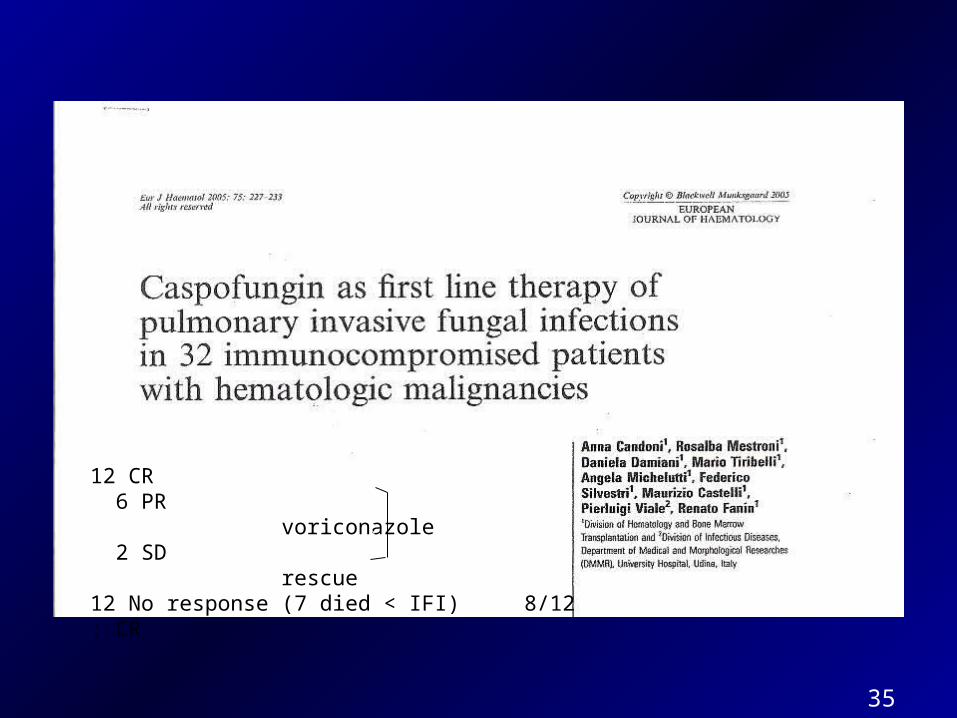
35
12 CR 6 PR voriconazole 2 SD rescue12 No response (7 died < IFI) 8/12 : CR

36K.A. MARR et al, CID 2004

37N. Singh, Transplantation, 2006

38
The prevalence of fungal infections in patients receiving empirical therapy is 4-8 %

39
Prevalence of fungal infections in persistently neutropenic patients not receiving empirical therapy
Pizzo et al. (1982) 18
EORTC (1989) 28 *
Guiot et al. (1993) 26*
Corey and Boeckh (2002) 45
Maertens et al. (2005) 21
* Autopsy-based data

40

41
CID, 2005

42
The preemptive approach(adapted from Maertens et al.)
« Possible IFI »
Diagnostic evaluation for IFI
Reasons Procedures
. FN refractory for 5 days
. FUO relapsing after 48 h with N
. Signs or/and symptoms suggestive of IFI
. Isolation of molds/hypae in URT
. Galactomannan assays positive (> 0.5)
. HRCT of the chest (+ sinuses)
. Bronchoscopy +BAL - Smears + cultures for bacteria, fungi, mycobacteria, Legionella
- PCR for CMV, HSV, VZV, Toxoplasma, Pneumocystis, Mycoplasma, Chlamydia
43
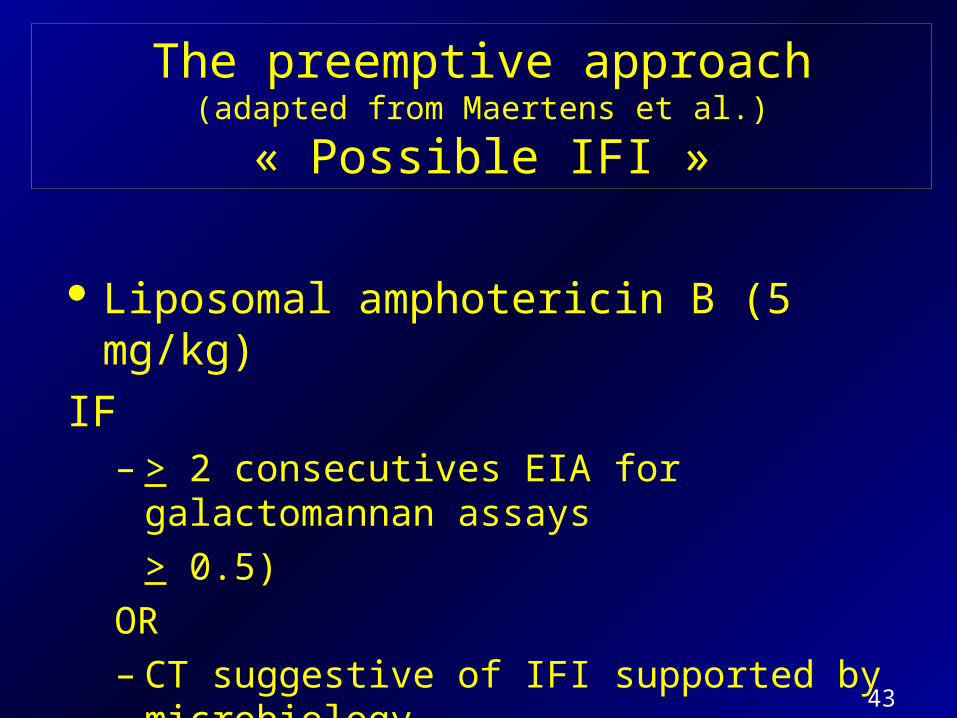
The preemptive approach(adapted from Maertens et al.)
« Possible IFI »
Liposomal amphotericin B (5 mg/kg)
IF– > 2 consecutives EIA for galactomannan assays
> 0.5)
OR– CT suggestive of IFI supported by microbiology

44
The preemptive approach of persistent febrile neutropenia in 88 patients(adapted from Maertens et al.)
Persistent fever 35/117 (29 %) episodes Prevalence of IFI : 22 % (mortality 36 %) No aspergillar infection was missed Early therapy could be initiated in clinically not
suspected cases Significant (78 %) reduction in use of
antifungals

45CID, 2005

46
Empirical versus preemptive therapy (liposomal amphotericin B) in patients with persisting fever
and neutropenia
Adapted from Maertens’ study 35 patients with persistent fever
EMPIRICAL APPROACH * PREEMPTIVE APPROACH
1 episode of IA (2.4 %) 10 episodes of IA (28 %)
? Death 2 deaths (20 %)
need of a controlled study
* Estimation from J. Klastersky, NEJM 2004

47
Blood, 2006

48
Empirical (E ) vs pre-emptive approach (PE)
Design
293 patients c hematological malignancies
R
Antifungal therapy
E
. Persistent or recurrent fever
PE
. Persistent or recurrent fever +. pneumonia. mucositis. septic shock. sinusitis. skin lesions. aspergillus colonisation. + gamacto-mannan

49
Empirical (E ) vs pre-emptive approach (PE)
Results
E
150 patients
PE
143 patients
Diagnosed IFI 4 (2.6 %) 13 (9.0) p < 0.02
Overall survival 147 (98 %) 136 (95 %) NS
IFI related mortality 0 (0 %) 3 (2.1 %) p = 0.12
Mean cost (euros) 3595 3595 NS

50
Estimated prevalence of invasive fungal infection (IFI) in neutropenic patients according to the management strategy
in exemplative studies
N° patients N° IFI Prevalence %
Controls ¹ 341 14 26.0
Prophylaxis ² (posaconazole)
291 7 2.4
Empirical therapy ³
(voriconazole)
415 15 3.6
Pre-emptive therapy (polyenes) 4
143 13 9.0
1 Guiot, CID, 19942 Ullmann, NEJM, 20073 Walsh, NEJM, 20024 Cordonnier, Blood, 2006

51
Which Antifungal Drug is Best for the Which Antifungal Drug is Best for the Empirical Empirical Treatment of Treatment of Patients with Febrile Neutropenia?Patients with Febrile Neutropenia?
Few adverse effects
(amphotericin B < lipid preparations < voriconazole = caspo)
Superiority of action :
– conventional amphotericin looks to be the least effective
– voriconazole might be superior in reducing microbiologically proven
failures
– Cost
Resistance

52
Average Daily Cost of Antifungal Therapy (Jules Bordet Bruxelles)
Dose Euros
Conventional Amphotericin B 1 mg/kg 8
Liposomal amphotericin B 3 mg/kg 629
Voriconazole 400 mg IV 407
Voriconazole 400 mg PO 84
Caspofungin 70 mg IV 644

53
Sensitivity of common pathogenic fungi
Amphotericin B Voriconazole Caspofungin
Candida sp. S S S
C. lusitaniae R S S
C. krusei S S** S
C. glabrata S S** S
Trichosporon sp. R S S
Aspergillus sp.* S S S
Fusarium sp. R S R
Mucorales S R R
C. neoformans S S R
*Except terreus**MIC are higher than for C. albicans but still < 3 ng/ml

54
Antifungal therapy in persistently febrile neutropenic patients
Voriconazole is presently the optimal choice for therapy and empirical therapy of suspected aspergillar infections
Early therapy (empirical) is needed since mortality remains high (30-50 %)
Empirical therapy reduces the incidence of IFI from + 25 % to + 3.5 %; the corresponding figures for liposomal ampho B and caspofungin being + 7 %
Experience with the preemptive approach is still limited; it is demanding in terms of diagnostic procedures but it reduces the rate of overtreatment.
There is evidence so far that pre-emptive therapy is inferior in efficacy and not more cost effective than the empirical approach
Conclusions

55
Needs for Improvement Needs for Improvement of Neutropenic Febrile Patients with of Neutropenic Febrile Patients with Persistent Fever to Avoid OvertreatmentPersistent Fever to Avoid Overtreatment
1. Better diagnostic tools for EARLIER microbiological and
clinical diagnosis : galactomannan, PCR, those caused by
Aspergillus sp.
1. More accurate IDENTIFICATION OF PATIENTS at high
risk of fungal infections (cf MASCC score)

56
Thank you foryour kind attention
and« Au revoir »


















