
1 An Interactive, Case-Based Approach to Targeted Therapies for GIST An On-Demand Webcast.
50
1 An Interactive, Case- Based Approach to Targeted Therapies for GIST An On-Demand Webcast
-
Upload
phoebe-parsons -
Category
Documents
-
view
213 -
download
0
Transcript of 1 An Interactive, Case-Based Approach to Targeted Therapies for GIST An On-Demand Webcast.

1
An Interactive, Case-Based Approach to Targeted Therapies for GISTAn On-Demand Webcast

2
Case Study
• 64-year-old white woman presents with diffuse abdominal pain
• Previously healthy except for resection of duodenal leiomyoma, 2 decades prior
• CT scan reveals multiple liver and peritoneal masses with no clear primary origin

3
Case Study Continues
• Percutaneous liver biopsy reveals CD117+ (KIT+) gastrointestinal stromal tumor (GIST)
• PET is positive in liver and peritoneum

4
Question 1
This patient’s primary tumor is most likely:
a) A new as-yet undetected GIST, a distinct clinical entity from her previous leiomyoma
b) The “leiomyoma” resected 2 decades priorc) A gastrointestinal adenocarcinoma

5
GIST Background
• Mesenchymal gut neoplasm now recognized as a distinct clinical entity– Formerly misclassified as smooth muscle tumors
(leiomyomas, leiomyoblastomas, leiomyosarcomas) or nerve-sheath tumors
• Most common mesenchymal tumor ofthe gut
• Likely shares a common ancestor with interstitial cells of Cajal
Mietten M, et al. Virchows Arch. 2001;438:1.

6
GIST Epidemiology
• Sites of presentation– Stomach 57%
– Small intestine 33.5%
– Colon/rectum 6.5%
– Retroperitoneum 0.5%
– Omentum/mesentery/other 2.5%
• United States– Annual incidence: 14.5 per million persons—4258
casesa
– Prevalence: 129 per million persons—37,882 cases
aClinically detected and KIT-expressing.Courtesy of Charles D. Blanke, MD.
7
KIT
• KIT: normal cellular homologue of viral oncogene
• Product: KIT, a 145-kd transmembrane glycoprotein, member of tyrosine kinase III
family– Protein normally expressed on heme progenitors, mast and germ cells, interstitial cells of Cajal
– Also expressed in a limited range of human cancers, including GISTs
• Activation stimulates cell growth and survival through MAP kinase and PI-3 kinase signaling cascades
• Nearly universal KIT positivity in GISTFletcher CDM, et al. Hum Pathol. 2002;33:459.
8
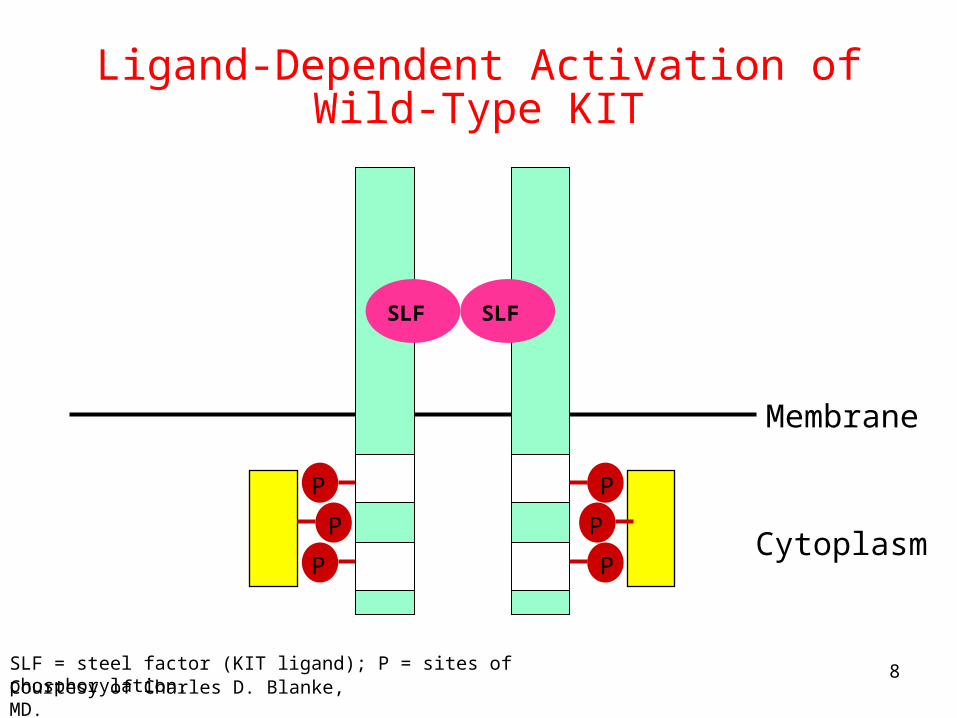
Ligand-Dependent Activation of Wild-Type KIT
Membrane
Cytoplasm
SLF = steel factor (KIT ligand); P = sites of phosphorylation.Courtesy of Charles D. Blanke, MD.
SLFSLF
P
P
P
P
PP

9
• Immunohistochemistry for KIT was positive in46 of 49 GISTs (94%)
• 5 of 6 GISTs had mutations in KIT gene
• Mutant forms of KIT are constitutively active
Hirota S, et al. Science. 1998;28:577.
Role of KIT Mutations in GIST
Development

10
Gain-of-Function Mutations and KIT(Exon 11)
In-frame mutationof exon 11
Membrane
Cytoplasm
Courtesy of Charles D. Blanke, MD.
P
P
P
P
PP

11
Case StudyReview
• Patient has biopsy-confirmed GIST with liver and peritoneal metastases
• The primary tumor was resected 2 decades prior

12
Question 2
How would you treat this patient?
a) Dacarbazine, mitomycin, doxorubicin, cisplatin ((D-MAP)
b) Mesna, doxorubicin, ifosfamide, dacarbazine (MAID), or doxorubicin, ifosfamide, dacarbazine (AID)
c) Imatinibd) Sunitinibe) Surgical resection

13
Case Study Continues
• Patient is started on imatinib mesylate 400 mg/d
– Approved as 1st-line treatment for KIT+ unresectable/metastatic malignant GIST; 2002
Gleevec (Imatinib). Package insert. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.

14
Why Not Chemotherapy?
05
0 0 0
27
5
0
10
20
30
40
50
60
70
80
90
100
Response Rate (%)
Epi/Ifos(N = 6)
HEDa
(N = 21)Pac
(N = ~15)Doxo
(N = ~15)Doce
(N = ~5)MAID
(N = 11)D-MAPa
(N = 21)aDefinitely GISTs
Epi/Ifos = epirubicin/ifosfamide; HED = hydroxyurea, etoposide, dacarbazine;Pac = paclitaxel; Doxo = doxorubicin; Doce = docetaxel; MAID = mesna, doxorubicin, ifosfamide, dacarbazine; D-MAP = dacarbazine, mitomycin, doxorubicin, cisplatin.
Courtesy of Charles D. Blanke, MD.

15
Why Not Surgery?
• Resection of peritoneal recurrence rarely prevents further recurrence
• GIST metastatic to liver tends to be multifocal and diffuse and not amenable to resection– Nearly universal recurrence after partial hepatectomy
• In rare cases of low-volume metastatic disease, primary tumor may be resected followed by use of imatinib
• Surgery may also be considered for imatinib-stabilized disease if all gross disease can be resected
Gold JS, et al. Ann Surg. 2006;244:176.

16
Premise of Targeted Therapy
• A precise understanding of the pathogenesis of a tumor will lead to more effective treatments, because of the unique nature of that process
– Treatment should also be less toxic
Druker B. Oncol Spect. 2001;2:534.

17
Imatinib Mesylate
• Class: 2-phenylaminopyrimidine• Molecular weight: 589.7 g/mol
C29H31N7O•CH4SO3
• CH3SO3H
Gleevec (imatinib). Package insert. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.

18
Rationale for Imatinib in GIST
aAll KIT mutants and many PDGFR mutants inhibited as well.PDGFR = platelet derived growth factor receptor.
Receptors Units (IC50 µM)
v-ABL 0.25
p210Bcr-Abl 0.25
p185Bcr-Abl 0.25
TEL-Abl 0.35
PDGFR 0.1a
TEL-PDGFR 0.15
KIT 0.1a
1. Druker BJ, et al. Nat Med. 1996;2:561. 2. Carroll M, et al. Blood. 1997;90:4947.

19
Phase I/II Studies of Imatinib in Advanced GISTGroup Phase Dose
(mg/d)N ORR
(%)SD (%)
PD (%)
Other
EORTC1 I 400–1000 35 54a 37 5
Wk Grp2 (B2222)
II 400/600 147 67 16 12 Median OS = 57 mo
EORTC3 II 800 27 71a 18 11 73% PFS at 12 mo
aNo responses in non-GIST sarcomas.EORTC = European Organization for Research and Treatment of Cancer; ORR = overall response rate; SD = stable disease; PD = progressive disease; PFS = progression-free survival; OS = overall survival.1. van Oosterom AT, et al. Eur J Cancer. 2002;38:S83. 2. Blanke CD, et al. J Clin Oncol. 2008;26:620. 3. Verweij J, et al. 8th CTOS; October 31-November 2, 2002. Abstract 19.

20
Phase III Studies of Imatinib in GIST
Study N Objectives
Primary Secondary
EORTC 620051
946 PFS ORR, safety,
tolerability
US Intergroup S00332
746 PFS, OS ORR, safety,
tolerability
1. Verweij J, et al. Lancet. 2004;364:1127. 2. Blanke CD, et al. J Clin Oncol. 2008;26:626.
• • Eligibility: metastatic or unresectable KIT+ GIST, measurable or nonmeasurable disease
• Prior chemotherapy allowed

21
Phase III Studies of Imatinib in GIST
Schema of EORTC 62005 and US Intergroup S0033
Low-doseimatinib(400 mg/d)
High-doseimatinibProgression Progression
Off-protocoltreatment
CROSSOVER
High-dose imatinib(800 mg/d)
Progression Off-protocol treatment
RANDOMIZATION
1. Verweij J, et al. Lancet. 2004;364:1127. 2. Blanke CD, et al. J Clin Oncol. 2008;26:626.

22
Phase III Studies of Imatinib in GISTResponse
EORTC 620051 US Intergroup S00332
400-mg Group
(%)
800-mgGroup
(%)
400-mg Group
(%)
800-mg Group
(%)
Complete response
5 6 5 3
Partial response
45 48 40 42
Stable disease
32 32 25 22
Progressive disease
13 9 12 10
1. Verweij J, et al. Lancet. 2004;364:1127. 2. Blanke CD, et al. J Clin Oncol. 2008;26:626.

23
MetaGIST Meta-analysis of Phase III Imatinib Studies
Progression-Free Survival
Van Glabbeke M, et al. 43rd ASCO; June 1-5, 2007. Abstract 10004.
0
5
10
15
20
25
30
35
40
45
50
Med
ian
PF
S (
mo
)
400 mg Imatinib 800 mg Imatinib
19 mo
23 mo
HR = 0.89; P = .04

24
MetaGIST Meta-analysis of Phase III Imatinib Studies
Overall Survival
0
10
20
30
40
50
60
70
Median OS (mo)
400 mg Imatinib 800 mg Imatinib
49 mo 49 mo
HR = 1.00; P = .97
Van Glabbeke M, et al. 43rd ASCO; June 1-5, 2007. Abstract 10004.

25
Case Study Continues
• The patient undergoes mutational analysis, which shows an exon 9 mutation

26
Question 3
Given the exon 9 mutation, the next step would be to:
a) Discontinue all targeted therapiesb) Switch to sunitinibc) Continue imatinib at 400 mgd) Increase imatinib dose to 800 mge) Increase imatinib dose to 1000 mg

27
Imatinib Dosing in Metastatic/Inoperable GIST Based on MetaGIST Project
• 400 mg/d should be the starting dose for most patients
• 800 mg/d is clearly more toxic and a dose most patients cannot tolerate
• Patients with exon 9 mutations may benefit more from 800 mg/d

28
Imatinib Toxicity in Advanced GIST EORTC 62005
Side Effect400 mg 800 mg
Grade 3 (%)
Grade 4 (%)
Grade 3 (%)
Grade 4 (%)
Granulo-cytopenia
4 3 5 2
Edema 3 0.2 9 0.4
Fatigue 6 — 11 0.2
Rash 2 — 5 0.2
Diarrhea 1 0.2 5 —
Bleeding 3 0.2 6 2
Any 26 6 43 8
Verweij J, et al. Lancet. 2004;364:1127.
29
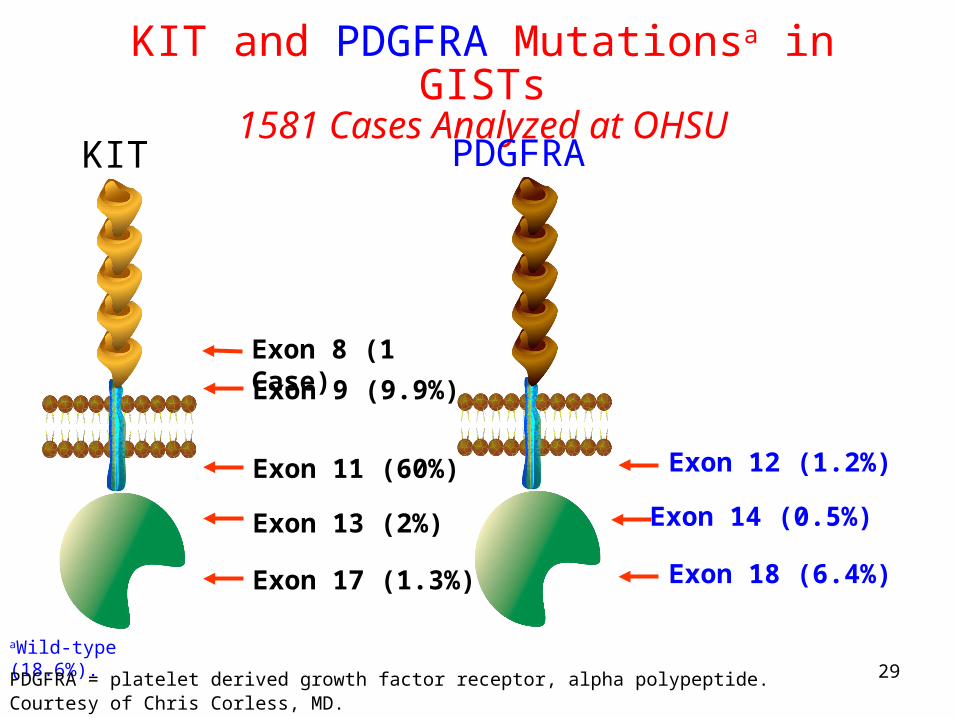
KIT and PDGFRA Mutationsa in GISTs1581 Cases Analyzed at OHSU
Exon 11 (60%)
Exon 9 (9.9%)
Exon 13 (2%)
Exon 17 (1.3%)
KIT
aWild-type (18.6%).
PDGFRA
Exon 12 (1.2%)
Exon 18 (6.4%)
Exon 14 (0.5%)
Exon 8 (1 Case)
Courtesy of Chris Corless, MD.PDGFRA = platelet derived growth factor receptor, alpha polypeptide.

30
MetaGIST Meta-analysis of Phase III Imatinib Studies
PFS in KIT Exon 9 Mutants
0
5
10
15
20
25
30
35
40
45
50
Median PFS (mo)
400 mg Imatinib 800 mg Imatinib
6 mo
19 mo
P = .017
Van Glabbeke M, et al. 43rd ASCO; June 1-5, 2007. Abstract 10004.

31
Rapid and Durable Response to Imatinib in Sample Patient
Pre-imatinib8/16/00
Post-imatinib2/06/01
4/14/05
(2 consistent scans)
Courtesy of Charles D. Blanke, MD.

32
Case Study Continues
• The patient’s imatinib dose is increased to 800 mg

33
Question 4
a) Is the standard of careb) Is not yet FDA approved, but has shown
benefit in a phase III studyc) Has no role due to lack of efficacy in the
adjuvant setting
In primary localized GIST, adjuvant imatinib:

34
Phase III Trial of Adjuvant Imatinib in Resected GIST
ACoSOG Z9001—Study Design
Objectives Primary: recurrence-free survival with imatinib in adjuvant setting relative to placebo
Secondary: overall survival, safety
Treatment Imatinib 400 mg/d or placebo for 1 yUpon recurrence, open-label unblinded phase: placebo cross-over to imatinib, imatinib dose increase to 800 mg if on active treatment or imatinib reinitiated at 400 mg/d if they had previously completed imatinib
Inclusion ≥3 cm, KIT+ GISTSurgery within 70 d prior to registration; NED on postoperative CT/MRINo prior imatinib; no other adjuvant therapy
DeMatteo R, et al. 43rd ASCO; June 1–5, 2007. Abstract 10079.Courtesy of Charles D. Blanke, MD.

35
Phase III Trial of Adjuvant Imatinib in Resected GIST: ACoSOG Z9001
DeMatteo R, et al. 43rd ASCO; June 1–5, 2007. Abstract 10079.Courtesy of Charles D. Blanke, MD.
Imatinib Placebo P value
Recurrence-free survival rates
n=325 21 events97% at 1 y
n=319 62 events83% at 1 y
P<.001; HR .33 (.20-.53)
Overall survival1-year follow-up
n=325 3 events
n=319 4 events
P<.72; HR .76 (.17-3.4)
Projected Recurrence-Free Survival (by tumor size)
3-6 cm n=128 4 events
100% at 1 y
n=13511 events95% at 1 y
P =.15; HR .44 (.14-1.4)
6-10 cm n=112 9 events
96% at 1 y
n=10521 events80% at 1 y
P = .01; HR .37 (.17-.81)
≥10 cm n=828 events
96% at 1 y
n=76 30 events67% at 1 y
P<.001; HR .19 (.09-.41)

36
Other Ongoing Phase III Trials ofAdjuvant Imatinib in GIST
Trial N Regimen Status
EORTC62024
750 Imatinib vs observation,for 24 mo
Active
SSGXVIII 280 Imatinib 400 mg/d,for 12 vs 36 mo
Recruiting
http://www.cancer.gov/clinicaltrials/EORTC-62024. Accessed April 2008.http://clinicaltrials.gov/ct2/show/NCT00116935?term=SSGXVIII&rank=1. Accessed April 2008.
37
Imatinib as Neoadjuvant Therapy Rationale
• Few complete responses with imatinib therapy– Most responding lesions have viable cells
• Cytoreduction may improve surgical outcomes
• Potential to increase resectability or reduce the extent of surgery
Eisenberg BL, et al. Expert Opin Pharmacother. 2003;4:869.Eisenberg BL, et al. Ann Surg Oncol. 2004;11:465.
38
Case Study Continues
• PET at 30 days is cold
• Patient progresses diffusely in the liver20 months later (CT and PET)

39
ImatinibMechanisms of Potential Resistance
• Resistance can be primary or secondary (following initial response)
• Mechanisms1
– Imatinib-resistant mutations in KIT or PDGFRA kinase domain
– KIT or PDGFRA gene amplification
– Activation of alternative kinase
• Resistance may be evidenced as progression of some lesions but not others– Focal vs general vs novel resistance
1. Fletcher JA, et al. Proc Am Soc Clin Oncol. 2003;22:815. Abstract 3275.

40
Question 5
a) Increase imatinib dose
b) Chemotherapy
c) Sunitinib
d) Hospice and supportive care
What is the best option following progression on imatinib?

41
Sunitinib (SU11248)
VEGFR2
VEGFR1
VEGFR3
PDGFR
CSF1RKITFLT3
PDGFR
Sutent (sunitinib). Package insert. New York, NY: Pfizer Labs; 2007.
Courtesy of Dr. Demetri and Dr. Casali.
Approved for treatment of GIST after disease progression or intolerance to imatinib; 2006
NH
O
NH
F
H3C
CH3
NH
O
N
CH3
CH3
Inhibits:
RET

42
Phase III Trial of Sunitinib in Imatinib-Refractory GIST
Time to Tumor ProgressionP
rog
ress
ion
(%
)
Sunitinib 50 mg (4 wk on/2 wk offx 6 cycles) (N = 243)
Median: 28.9 wk
Placebo (N = 118) Median: 7.0 wk
Hazard ratio = 0.28
P < .0001
Blinded phase
Casali PG, et al. Proc Am Soc Clin Oncol. 2006;24:abstract 9513.
Time (weeks)
100
90
80
70
60
50
40
30
20
10
0
0 13 26 39 52 65 78

43
Continuous Daily Dosing of Sunitinib
George S, et al. 43rd ASCO; June 1-5, 2007. Abstract 10015.
aIndependent 3rd-party review (interim analysis).

44
Increased Hematologic Toxicity with Continuous Daily Dosing of Sunitinib
Hematologic Laboratory Abnormalities (Any Grade)
Laboratory Abnormalitya
CDD (N = 60)b1
(Present Study)N (%)
ID (N = 202)2
N (%)
Neutrophils 40 (67) 106 (52)
Hemoglobin 42 (70) 124 (61)
Platelets 25 (42) 81 (40)
aMaximum grade, NCI CTCAE v.3.0.bTo date.CDD = continuous daily dosing; ID = intermittent dosing.
1. George S, et al. 43rd ASCO; June 1-5, 2007. Abstract 10015. 2. Demetri GD, et al. Lancet. 2006;368:1329.

45
Phase II Study of Sunitinib in Imatinib-Resistant GIST:Analysis by KIT and PDGFRA Mutational Status
Mutation Status n(N = 47)
RECIST Response
Benefit (Response + Stable
>6 Months)
Exon 9 KIT mutation 19 37% 63%
Exon 11 KIT mutation 42 5% 36%
Wild-type 9 N/A 56%
PDGFR 4 N/A 25%
Adapted courtesy of Chris Corless, MD.
PDGFRA = platelet derived growth factor receptor; RECIST = Response Evaluation Criteria in Solid Tumors.

46
In vitro Effects of Sunitinib or Imatinib on KIT Exon 11 + Exon 14 or 17 Double Mutants
pKIT = phosphorylated KIT.Heinrich M, et al. 43rd ASCO; June 1-5, 2007. Abstract 10006.

47
In vitro Effects of Sunitinib or Imatinib on Kinase Activity of KIT Mutants
SummaryApproximate IC50 (nM)
Mutation(s) Affected Exon(s) 2nd Exon: Function Sunitinib Imatinib
V560D 11 - <50 100
V560D + V654A 11 + 13 ATP BP <100 5000
V560D + T670I 11 + 14 ATP BP <50 10000
V560D + L783V 11 + 16 Unknown <100 100
V560D + D816H 11 + 17 Act. loop ≥1000 5000
V560D + D820G 11 + 17 Act. loop >1000 5000
V560D + N822K 11 + 17 Act. loop >1000 1000
V560D + Y823D 11 + 17 Act. loop >1000 >1000
V560D + A829P 11 + 18 Ext. act. loop >1000 >1000
Act. loop = activation loop; ATP BP = ATP binding pocket; Ext. act. loop = extended activation loop.Heinrich M, et al. 43rd ASCO; June 1-5, 2007. Abstract 10006.

48
Investigational Drugs/Targets in GIST
Drug Targets
Motesanib (AMG 706) VEGFR, PDGFR, KIT, RET
Midostaurin (PKC412) PKCNilotinib (AMN107) KIT, PDGFRA
Rapamycin (RAD001) mTOR
Sorafenib (BAY 43-9006) RAF, KIT, VEGFR, PDGFRβ, FLT3, RET
Dasatinib (BMS-354825) Src, KIT, PDGFR
Retaspimycin (IPI-504) Heat-shock protein 90
Oblimersen (G3139) Bcl-2

49
Treatment of GISTRemaining Questions
• Is anything better than imatinib up-front?
– Can we test single agents in that setting?
• What can imatinib be combined with?
– Upcoming Intergroup trial will use bevacizumab
• Will we eventually select the best drug(s)
based on mutational analysis?
– We ARE now using mutational status to select the
best dose of imatinib

50
Conclusions
• Surgical resection remains the treatment of choice for localized primary GIST
• Imatinib remains the systemic agent of choice in GIST, despite the emergence of resistance in some patients– Initial dose should be 400 mg/d in advanced disease
– Patients with exon 9 mutants should get 800 mg/d
• Sunitinib is the agent of choice for patients who are resistant or intolerant to imatinib


















