1 A Systematic Review of the Genetic Mechanisms …...1 1 A Systematic Review of the Genetic...
59
1 A Systematic Review of the Genetic Mechanisms of Dolutegravir Resistance 1 2 Soo-Yon Rhee a #, Philip M. Grant a , Philip L. Tzou a , Geoffrey Barrow b , P. Richard Harrigan c , John 3 P.A. Ioannidis d , Robert W. Shafer a 4 5 a Department of Medicine, Stanford University, Stanford, California, USA 6 b Centre for HIV/AIDS Research, Education and Services (CHARES), Department of Medicine, 7 University of the West Indies, Kingston, Jamaica 8 c Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada 9 d Meta-Research Innovation Center at Stanford, Stanford University, Stanford, California, USA 10 11 12 13 Running Title: Dolutegravir Resistance 14 15 16 17 18 19 #Address correspondence to Soo-Yon Rhee, [email protected]. 20 21
Transcript of 1 A Systematic Review of the Genetic Mechanisms …...1 1 A Systematic Review of the Genetic...
1
A Systematic Review of the Genetic Mechanisms of Dolutegravir Resistance 1
2
Soo-Yon Rheea#, Philip M. Granta, Philip L. Tzoua, Geoffrey Barrowb, P. Richard Harriganc, John 3
P.A. Ioannidisd, Robert W. Shafera 4
5
aDepartment of Medicine, Stanford University, Stanford, California, USA 6
bCentre for HIV/AIDS Research, Education and Services (CHARES), Department of Medicine, 7
University of the West Indies, Kingston, Jamaica 8
cDepartment of Medicine, University of British Columbia, Vancouver, British Columbia, Canada 9
dMeta-Research Innovation Center at Stanford, Stanford University, Stanford, California, USA 10
11
12
13
Running Title: Dolutegravir Resistance 14
15
16
17
18
19
#Address correspondence to Soo-Yon Rhee, [email protected]. 20
21
2
ABSTRACT 22
Background: Dolutegravir (DTG) has is one of the most commonly used antiretroviral (ARV) 23
drugs but there has been no systematic review of the genetic mechanisms of DTG resistance. 24
Methods: We systematically reviewed DTG resistance studies to map key DTG resistance 25
concepts, analyzing mutations emerging in vitro and in vivo under DTG selection pressure; the 26
effect of integrase strand transfer inhibitor (INSTI)-resistance mutations on in vitro DTG 27
susceptibility; and the virological efficacy of DTG in populations at increased risk for virological 28
failure (VF). 29
Results: We analyzed 14 studies describing 84 in vitro passage experiments, 26 studies describing 30
63 persons developing VF plus INSTI-resistance mutations on a DTG-containing regimen, 41 31
studies describing 572 in vitro DTG susceptibility results, and 22 clinical trials and 16 cohort 32
studies of DTG-containing regimens in persons at increased risk of VF. The most common INSTI-33
resistance mutations arising in persons with VF on a DTG-containing regimen were R263K, 34
G118R, N155H, and Q148H/R, with R263K and G118R predominating in previously INSTI-naïve 35
persons. The public availability of complete integrase sequences in only 2 of 63 persons with VF 36
plus INSTI-resistance mutations precluded the identification of potentially novel DTG-resistance 37
mutations. R263K alone reduced DTG susceptibility approximately 2-fold while viruses 38
containing G118R alone generally reduced DTG susceptibility more than 5-fold. The highest 39
levels of reduced susceptibility occurred in viruses containing Q148 mutations in combination with 40
G140 and/or E138 mutations plus one or more accessory INSTI-resistance mutation. Several DTG-41
containing two-drug combinations were highly effective for first-line therapy and for virologically 42
suppressed persons provided DTG’s companion drug was fully active. DTG-containing three-drug 43
combinations were highly effective for salvage therapy in ARV-treated, INSTI-naïve persons 44
provided one or more of DTG’s companion drugs was fully active. However, the use of DTG 45
3
monotherapy in virologically suppressed persons and possibly functional DTG monotherapy in 46
persons with active viral replication were associated with a non-trivial risk of VF plus INSTI-47
resistance mutations. 48
Conclusions: The spectrum of DTG-selected mutations and effects of these mutations on in vitro 49
DTG susceptibility is emerging but is limited in part because integrase sequences have been 50
published for only a small proportion of cases of DTG-associated VF. The risks of VF and INSTI-51
resistance mutations in persons receiving functional DTG monotherapy poses a challenge to 52
standard fixed-dose DTG-containing combinations in low- and middle-income countries where 53
genotypic resistance testing is not routinely available and where such combinations have recently 54
been recommended for persons with VF on a first-line ARV regimen. 55

4
INTRODUCTION 56
The integrase strand transfer inhibitor (INSTI) dolutegravir (DTG) has an improved safety 57
profile, greater efficacy, and lower cost compared with efavirenz 1–3. DTG will play a dominant 58
role in first-line therapy in many countries, including those with and without high levels of pre-59
treatment drug resistance. DTG has also recently been recommended by the WHO as a preferred 60
component for second-line therapy 4. 61
The mutations selected by DTG and their effects on DTG susceptibility define the genetic 62
mechanisms of DTG resistance. Understanding these mechanisms is essential for monitoring 63
persons with VF on a DTG-containing regimen and for determining the genetic barrier to DTG 64
resistance. The efficacy of DTG in persons at increased risk of virological failure helps inform 65
which companion antiretroviral (ARV) drugs should be used in combination with DTG in ARV-66
treated persons. These data are particularly relevant to the use of DTG in the low- and middle-67
income countries where genotypic resistance testing is not routinely performed prior to starting a 68
DTG-containing regimen. 69
Here, we systematically review published studies and meeting presentations on DTG 70
resistance. The review maps key DTG resistance concepts and analyzes the mutations emerging 71
in vitro and in vivo under DTG selection pressure; the effect of INSTI-resistance mutations on in 72
vitro DTG susceptibility; and the virological efficacy of DTG in persons at increased risk for 73
virological failure (VF) and drug resistance. 74
75
5
METHODS 76
Literature Review 77
A systematic search of the NCBI PubMed database for all English language papers on DTG 78
resistance using the search string: “Dolutegravir or GSK1349572” was last updated on 24. January 79
2019. A list of the titles and abstracts presented at scientific meetings during 2017 and 2018 that 80
contained the drug name “Dolutegravir” was also compiled. The scientific meetings included 81
Conference on Retroviruses and Opportunistic Infections (CROI), IAS Conference on HIV 82
Science, International AIDS Conference, International Workshop on HIV Drug Resistance and 83
Treatment Strategies (HIVDRW), IDWeek, InterScience Conference on Antimicrobial Agents and 84
Chemotherapy, European AIDS Conference, European Meeting on HIV & Hepatitis, and Glasgow 85
HIV Drug Therapy. Additional publications and meeting presentations were identified from the 86
reference lists of identified papers. 87
Retrieved studies were reviewed in three stages. First, titles and/or abstracts were reviewed 88
to identify studies relevant to DTG resistance. Following the title/abstract review, complete 89
publications or posters (in the case of meeting presentations) were reviewed to determine which 90
studies contained data relevant to the three main areas of focus: (i) mutations emerging under DTG 91
selection pressure in vitro and in vivo; (ii) in vitro DTG susceptibility data; and (iii) virological 92
efficacy of DTG. In (iii), we examined the virological efficacy of DTG when used with a reduced 93
number of companion ARVs or when used to treat persons with viruses containing either INSTI-94
associated DRMs or containing DRMs that reduce the activity of the ARVs used in combination 95
with DTG. In the third stage, studies were reviewed further to determine whether they merited 96
inclusion in a table, a figure, or in the text. The complete list of studies meeting the first review 97

6
stage are available in a publicly available companion Zotero reference database 98
(https://www.zotero.org/groups/2262131/dtg_stanfordhivdb). 99
The following types of studies passing the first review stage were excluded: (i) review 100
papers lacking primary data; (ii) studies containing drug resistance data for the INSTIs raltegravir 101
or elvitegravir but not DTG; (iii) in vitro experiments designed to understand the cellular, 102
biochemical, or biophysical (rather than genetic) mechanisms of DTG resistance; (iv) studies of 103
HIV-2 or non-group M viruses; and (v) studies containing redundant analyses of a clinical trial or 104
cohort (Fig. 1). 105
Studies passing the first two review stages were subjected to additional exclusion criteria: 106
(i) clinical trials and cohort studies of persons receiving a standard three-drug first-line DTG- 107
containing regimen were excluded from summary tables as it has already been established from 108
previous reviews that such persons are at extremely low risk of VF and emergent resistance 1,5; (ii) 109
clinical trials and cohort studies of DTG intensification or switches to DTG-containing three-drug 110
regimens in virologically suppressed persons as persons in these studies would be expected to be 111
at extremely low risk of VF; (iii) cohort studies containing fewer than 20 persons that did not yield 112
findings that were not also observed in larger studies; (iv) cohort studies containing persons with 113
highly heterogeneous past treatment histories and/or highly heterogenous DTG-containing 114
regimens; (v) cohort studies and case reports of INSTI-experienced persons developing INSTI-115
resistance mutations, if there was no baseline integrase genotype prior to DTG therapy; and (vi) 116
studies describing novel in vitro susceptibility testing assays. 117
Data Extraction 118
Data for all studies was extracted by RWS and PMG, and then SYR. Discrepancies were 119
handled by jointly reviewing the full-text of studies with discrepancies. 120

7
121
Mutations emerging under DTG selection pressure 122
For studies in which viruses were cultured in the presence of increasing DTG 123
concentrations (in vitro passage experiments), we recorded data about the pre-passage virus 124
including its subtype, whether it was a laboratory strain or a clinical isolate, and whether it 125
contained pre-existing known or suspected INSTI-resistance mutations; and the integrase 126
mutations that developed during in vitro passage. 127
For studies of persons whose viruses developed established or suspected INSTI- resistance 128
mutations while receiving DTG we recorded (i) the extent of ARV treatment (ART) prior to DTG 129
therapy including whether the person was ART-naïve, ART-experienced but INSTI-naïve, or 130
INSTI-experienced but DTG-naïve; (ii) whether the person was stably virologically suppressed 131
defined as having a plasma HIV-1 RNA virus level below 50 copies/ml for ³6 months on an 132
unchanged ART regimen; (iii) the ARVs used in combination with DTG, specifically, whether the 133
person received DTG monotherapy or dual therapy, DTG plus two nucleoside RT inhibitors 134
(NRTIs), or DTG plus an optimized background regimen; and (iv) the integrase mutations reported 135
to develop during therapy. 136
INSTI-resistance mutations were defined as mutations previously reported to be selected 137
by raltegravir or elvitegravir and associated with reduced raltegravir or elvitegravir susceptibility. 138
Established nonpolymorphic INSTI-resistance mutations were defined as H51Y, T66A/I/K, E92Q, 139
G118R, F121Y, G140A/S/C, Y143C/G/H/K/R/S, S147G, Q148H/K/R, S153Y/F, N155H, S230R, 140
and R263K 6,7. Polymorphic accessory INSTI-associated mutations were defined as established 141
nonpolymorphic INSTI-resistance mutations occurring at a prevalence ³1% of INSTI-naïve 142

8
persons in one or more subtypes and included L74I/M, Q95K, T97A, V151I, E157Q, G163K/R, 143
and D232N 6,8. 144
In vitro susceptibility data 145
For studies containing in vitro susceptibility data, we recorded (i) whether the virus was a 146
clinical or laboratory isolate; (ii) the integrase mutations in the virus and, for laboratory isolates, 147
whether the virus contained one or more mutations placed by site-directed mutagenesis; (iii) the 148
virus subtype; (iv) the method of susceptibility testing; and (v) the fold reduced susceptibility 149
compared with wild type. Duplicate results defined as the identical results on the same site-directed 150
mutant performed by the same laboratory method were excluded. 151
Virological outcome studies 152
In both clinical trials and cohort studies, we characterized study subjects according to (i) 153
their past ART history as either ART-naïve, ART-experienced but INSTI-naïve, and INSTI-154
experienced; (ii) whether they were stably virologically suppressed; and (iii) the components of 155
their DTG-containing regimen: DTG monotherapy or dual therapy, DTG plus two NRTIs, or DTG 156
plus an optimized background. For clinical trial results reporting data at multiple time points, we 157
extracted data from the 24- and 48-week time points. 158
Analysis 159
Mutations emerging under DTG selection pressure 160
In vitro passage experiments included those performed in cell culture and those performed 161
in humanized mice. The analysis of these experiments focused on established nonpolymorphic 162
9
INSTI-resistance mutations as no novel nonpolymorphic mutations were reproducibly observed in 163
more than one study. 164
The analysis of emergent INSTI-resistance mutations in persons receiving DTG compiled 165
all reported established nonpolymorphic and polymorphic INSTI-resistance mutations and 166
additional novel nonpolymorphic integrase mutations. The analysis included reports of emergent 167
INSTI-resistance mutations from clinical trials, cohort studies, and case reports to identify the full 168
spectrum of DTG-selected mutations in vivo. 169
In vitro susceptibility data 170
For site-directed mutants, the complete list of mutations was known. However, for most 171
clinical isolates, neither the complete nucleotide sequence nor the complete list of integrase 172
mutations was reported. Therefore, for clinical isolates, only those mutations provided by authors 173
were reported. Of note, the INSTI-selected mutation V151I occurs in the NL43 laboratory isolate, 174
the most common laboratory isolate used for creating site-directed mutants. Therefore, this 175
mutation was excluded from our analyses. However, the supplementary material indicates which 176
susceptibility tests were performed on NL43 site-directed mutants. The in vitro susceptibility of 177
site-directed mutants and clinical isolates containing the four most commonly selected INSTI-178
resistance mutations among persons receiving DTG – R263K, G118R, N155H, and Q148H/R/K – 179
were characterized. 180
Virological outcome studies 181
VF was defined across all studies using an intention-to-treat approach such that subjects 182
discontinuing therapy for any reason such as intolerance or nonadherence were categorized as 183
experiencing VF. This approach was adopted both for studies that reported their results in this 184

10
manner and for those that employed a narrower definition of protocol-defined VF. 95% Clopper-185
Pearson confidence interval for proportions of VF and VF plus emergent INSTI resistance were 186
estimated for each individual study. Pooled proportion and the I2 statistic, a measure of 187
heterogeneity among studies, were calculated using the random-effects model implemented in the 188
R meta package in the proportions of VF and VF plus resistance at weeks 24 and 48. 189
RESULTS 190
In vitro Passage Experiments 191
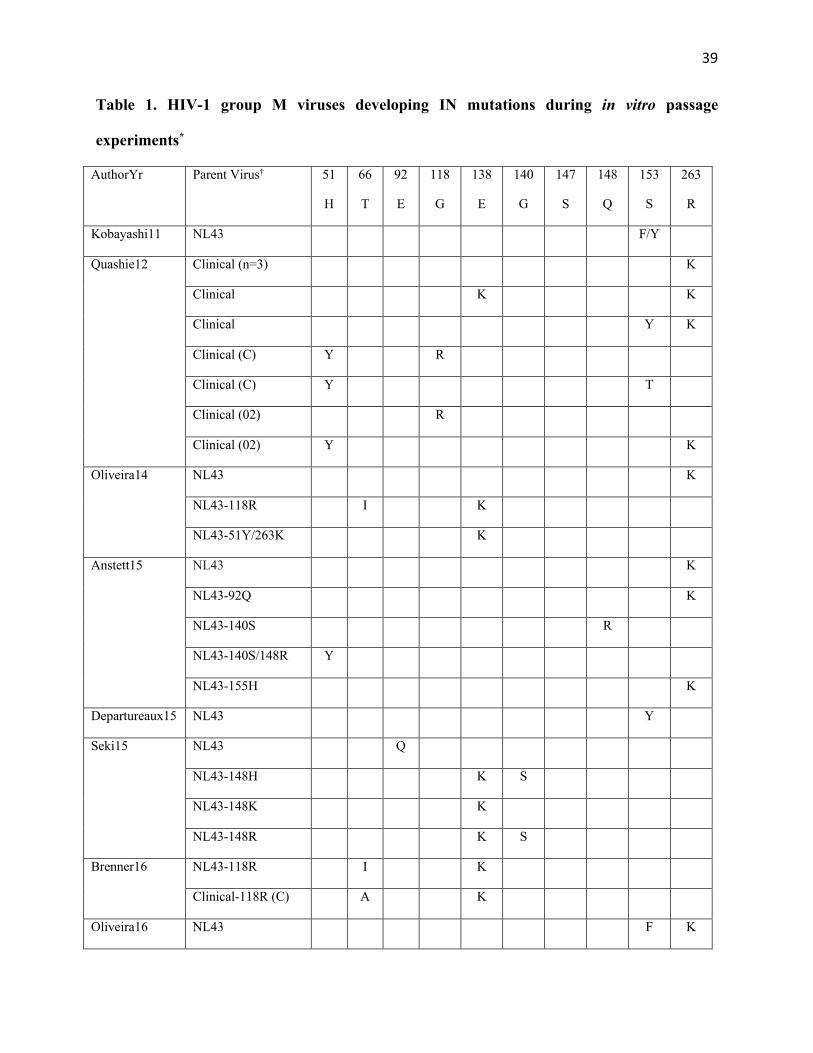
A total of 14 studies described 84 in vitro passage experiments in which an HIV-1 group 192
M virus was cultured with increasing DTG concentrations (Table 1). In 62 experiments, mutations 193
were selected after a median of 30 weeks (interquartile range [IQR]: 20 to 46 weeks). These 62 194
experiments used 37 clinically derived isolates and 25 laboratory isolates. Isolates lacking 195
established INSTI-associated DRMs prior to DTG passage were labeled as wild type. Fifty-three 196
of the viruses had a subtype B backbone; four had a subtype C backbone, two had a CRF02_AG 197
backbone, two had a subtype D backbone, and one had a CRF01_AE backbone. 198
R263K was the most commonly selected INSTI-resistance mutation, developing in 33 199
experiments from 6 studies performed by the same research laboratory (Table 1). In 31 of these 200
experiments, the baseline virus was wild type (including 5 with pre-existing polymorphic 201
accessory resistance mutation, E157Q); the other two baseline viruses contained E92Q or N155H. 202
Other commonly selected INSTI-resistance mutations included S153Y/F (11 isolates, 6 studies), 203
E138K (9 isolates, 4 studies), H51Y (7 isolates, 4 studies), T66A/I (3 isolates, 2 studies) and 204
G118R (2 isolates, 1 study). There was insufficient data to determine whether a particular subtype 205
predisposed to the emergence of specific mutations. In 21 experiments using 11 wild type and 10 206
11
viruses containing INSTI-resistance mutations, no additional mutations were observed during in 207
vitro passage. 208
There were two additional studies not shown in Table 1 of humanized mice infected with 209
a laboratory HIV-1 strain and subsequently treated with DTG monotherapy. In one study, one of 210
five mice infected with HIV-1BAL and treated with DTG monotherapy for 20 weeks developed the 211
INSTI-resistance mutations E138K, G140S, Q148H, H155H, and S230R 9. In another study, two 212
of four mice infected with HIV-1LAI and treated with an injectable long-acting DTG formulation, 213
developed R263K and E157Q 10. 214
In an additional experiment (also not shown in Table 1), the laboratory strain HIV-1LAI 215
passaged with high concentrations of DTG developed five nucleotide mutations in the nef gene: 216
three mutations and one deletion in the highly conserved last six nucleotides of the 3’ polypurine 217
tract (GGGGGG ® GCATG) and one mutation six nucleotides upstream of the 3’ polypurine tract 218
11. The nucleotide deletion resulted in a stop codon five amino acids downstream of the 3’ 219
polypurine tract. 220
Mutations Emerging in Persons Receiving DTG 221
The studies in which persons receiving DTG developed VF and one or more INSTI- 222
resistance mutations included (i) 11 studies of INSTI-naïve persons (Table 2); (ii) eight studies of 223
virologically suppressed persons receiving DTG monotherapy for treatment simplification (Table 224
3); and (iii) eight studies of persons who had a history of VF and INSTI- resistance mutations on 225
a raltegravir- or, less commonly, elvitegravir-containing regimen (Table 4). Emergent INSTI-226
resistance mutations have not been reported in any of the trials of a first-line regimen comprising 227
DTG plus two NRTIs 1,5. 228

12
The eleven studies of INSTI-naïve persons included four clinical trials, one cohort study, 229
and six case reports (Table 2). Three of the four clinical trials included 712 ART-experienced 230
patients receiving DTG plus an optimized backbone 12–16, which was required in the two largest 231
trials to include at least one fully active ARV based on a pre-therapy genotypic resistance test 12,14. 232
One of the clinical trials included 120 ART-naïve persons receiving DTG plus lamivudine (3TC) 233
17. The cohort study included 310 ART-naïve and ART-experienced INSTI-naïve persons 234
receiving DTG plus two NRTIs 18. The six case reports, included three ART-naïve persons who 235
received DTG plus TDF/FTC and three ART-experienced persons who received DTG plus an 236
optimized background regimen or 2 NRTIs. Overall, 21 persons developed VF and an INSTI-237
resistance mutation. The most common mutations were R263K in 13 persons and G118R in 6 238
persons. Other nonpolymorphic resistance mutations were E138K/T (3 persons), N155H (2 239
persons), Q148K (1 person), S230R (1 person), T66I (1 person) and H51Y (1 person). The 240
nonpolymorphic mutations A49G developed in two persons. 241
The eight studies of persons receiving DTG monotherapy for treatment simplification 242
included three trials with 211 persons, three cohort studies with 92 persons, and two case reports 243
(Table 3). Depending on the study, 6% to 61% of persons in the trials and cohorts had a history of 244
receiving an INSTI. Overall, 16 persons developed VF and an INSTI-resistance mutation. The 245
most common mutations were N155H (7 persons), Q148H/R (3 persons), R263K (2 persons), 246
G118R (2 persons), and S147G (2 persons). Among the 16 persons with VF and emergent INSTI-247
resistance mutations, seven had previously received raltegravir or elvitegravir but had not 248
previously experienced VF on a raltegravir or elvitegravir-containing regimen. 249
In two studies, in which the 3’ polypurine tract was sequenced, two of 17 of persons had 250
one or more nucleotide changes in this highly conserved region. One virus containing two 3’ 251
polypurine tract nucleotide changes (GGGGGG ® GGGAGC) compared with baseline and no 252

13
reported integrase mutations 19 and another containing one polypurine tract nucleotide change had 253
the integrase mutation R263K 20. 254
The eight studies of persons with history of VF and INSTI-resistance mutations on a 255
previous raltegravir- or elvitegravir-containing regimen included two of the VIKING trials (the 256
phase IIb VIKING and phase III VIKING-4 trials), one cohort study, and five case reports (Table 257
4). In these eight studies, 31 persons developed VF on a DTG-containing regimen. Prior to 258
receiving DTG, the most common DRMs were Q148H + G140S (22 persons), E138A/K/T (10 259
persons), Y143C/H/R (9 persons), L74M (5 persons), T97A (5 persons), N155H (2 persons), and 260
Q148R + G140A (1 person). After DTG VF, the most common emergent INSTI-associated DRMs 261
were T97A (22 persons), E138K/A/T (12 persons), N155H (7 persons), L74M/I (4 persons), 262
Q148H±G140S (3 persons), and S147G (3 persons). The nonpolymorphic mutations G149A and 263
F139Y developed in two persons and one person, respectively. Of the 63 sequences in Tables 2-4 264
with emergent INSTI-resistance mutations, only two were submitted to GenBank 21,22. 265
In vitro Susceptibility 266
A total of 41 studies contained 572 DTG in vitro susceptibility results (Table S1). These 267
included 28 studies of site-directed mutants, nine of clinical isolates, and four of both site-directed 268
mutants and clinical isolates. Overall, there were 395 susceptibility results on site-directed mutants 269
and 177 results on clinical isolates (Table S2). The site-directed mutants generally contained 270
raltegravir- and elvitegravir-associated resistance mutations, mutations observed under DTG 271
selection pressure, and additional accessory INSTI-associated mutations of uncertain significance. 272
The complete integrase sequence was known for all of the site-directed mutants but was available 273
for only 74 (41.8%) of the 177 clinical virus isolates. 274

14
The most commonly used assay was the recombinant virus reporter gene PhenoSense assay 275
(Monogram Biosciences, South San Francisco; n=279). Most of the remaining assays were 276
recombinant virus reporter gene assays developed by other laboratories including ViiV, McGill 277
University, the ANRS, and the NCI. The site-directed mutants contained 127 distinct mutational 278
patterns and for 45 patterns, susceptibility tests were performed with more than one assay. For 279
these 45 patterns, the range/median ratio, a nonparametric measure of dispersion, was £1.0 for 21 280
patterns; 1.1 to 2.0 for 20 patterns and >2.0 for 4 patterns. The dispersion appeared to be lowest 281
between the PhenoSense and ViiV assays (Table S3). 282
Fig. 2 summarizes results on 281 site-directed mutants and clinical isolates containing 283
patterns of INSTI-resistance mutations characterized by four signature mutations: R263K, G118R, 284
N155H, and Q148H/R/K. The first seven plots in Fig. 2 show the levels of fold reduced 285
susceptibility for 42 isolates containing R263K. Twenty-six of the 42 assays were performed using 286
either the McGill laboratory reporter gene (n=17) or peripheral blood mononuclear cell (n=9) 287
assays, while 16 results were determined using the PhenoSense (n=11), NCI (n=3), ViiV (n=1) or 288
ANRS assays (n=1). The median reduction in DTG susceptibility was ~2-fold for isolates with 289
R263K alone, ~5-fold for isolates with R263K plus two additional mutations, and 10 to 15-fold 290
for isolates with R263K plus G118R, N155H, or Q148R (usually in combination with one 291
additional INSTI-resistance mutation). 292
The next three plots in Fig. 2 summarize the levels of reduced susceptibility for 17 isolates 293
containing G118R without R263K. G118R alone or in combination with T66A, L74I, and T97A 294
reduced DTG susceptibility between 5 and 15-fold. Two of the site-directed mutants contained a 295
CRF02_AG integrase backbone. One G118R-containing clinical isolate lacking other reported 296
INSTI-resistance mutations had 30-fold reduced susceptibility; however, the complete list of 297
mutations in this isolate was not available 14. 298
15
The next eight plots summarize the levels of reduced susceptibility for 64 isolates 299
containing N155H (without R263K or G118R). N155H alone or in combination with one 300
additional INSTI-resistance mutation usually yielded <2-fold reduced DTG susceptibility. 301
However, in combination with Q148H/R or ³2 additional resistance mutations, reduced 302
susceptibility ranged from 2-fold to >15-fold. The highest levels of reduced susceptibility were 303
found in a site-directed mutant containing the extremely rare mutation pair L74F+V75I 23 and in 304
clinical isolates containing N155H plus Q148H, G140S, and T97A 24 and N155H plus T97A, 305
E138K, and S147G, each of which had >50-fold reduced DTG susceptibility 24. 306
The final nine plots in Fig. 2 summarize the levels of reduced susceptibility for 158 isolates 307
containing Q148H/R/K without R263K, G118R, or N155H. Q148H/R/K alone did not cause 308
measurably reduced DTG susceptibility. However, in combination with a single additional INSTI-309
resistance mutation (usually at position 140 or 138), the median reduction in susceptibility was 310
about 3-fold for Q148H/R and 10-fold for Q148K. In combination with ³2 additional resistance 311
mutations, the median reduction in susceptibility was generally >10-fold. The contribution of 312
accessory mutations to reductions in DTG susceptibility was most striking in clinical isolates 313
possibly because these viruses were likely to have additional background mutations that facilitate 314
reduced susceptibility 25–27. 315
Several isolates lacking each of the four signature mutations in integrase were also reported 316
to have ³2-fold reduced DTG susceptibility including isolates with F121Y 28, S230R 29, 317
E92Q+G140A 30, and T66K+L74M, V151L, and S153Y 31. Additionally, a site-directed mutant 318
containing the five nucleotide changes selected in vitro in the 3’ polypurine tract region displayed 319
23-fold reduced DTG susceptibility 11. 320
16
Virological Efficacy in Populations at Increased Risk for Drug Resistance 321
There were 22 clinical trials and 19 cohort studies meeting one of the following inclusion 322
criteria: (i) dual or monotherapy in ART-naïve persons (Table 5); (ii) dual or monotherapy in 323
virologically suppressed persons (Tables 6 and 7); (iii) DTG-containing regimens in ART-324
experienced, INSTI-naïve persons without virological suppression (Table 8); and (iv) DTG-325
containing regimens in INSTI-experienced persons (Table 9). Each table includes the proportions 326
of VF and VF plus emergent INSTI resistance for each study and the pooled proportion for all 327
studies combined at weeks 24 and 48. Genotypic resistance testing was performed In each of the 328
clinical trials in non-virologically suppressed persons (Tables 5, 8, and 9) either to determine 329
subject eligibility and/or to select the ARVs to be used in combination with DTG. 330
Dual or monotherapy in ART-naïve persons 331
Three clinical trials described 856 ART-naïve persons treated with DTG/3TC dual therapy 332
(Table 5) 17,32,33. Each excluded persons with baseline plasma HIV-1 RNA levels >100,000 32 or 333
>500,000 copies/mL 17 or genotypic evidence of 3TC resistance. The largest trial was a 334
randomized controlled trial (GEMINI) that reported a noninferior 91% virological response rate at 335
week 48 for 716 persons receiving DTG/3TC compared with a similar number of persons receiving 336
DTG plus tenofovir (TDF) plus emtricitabine (FTC) 32. The remaining two trials were pilot trials 337
that enrolled 120 persons for 48 weeks (A5353) 17,34 or 20 persons for 48 weeks 33. The VF rate 338
was 10% in these two trials. One person in A5353 with VF developed the DTG-resistance mutation 339
R263K 17. 340
There were two small studies of ART-naïve persons treated with DTG monotherapy that 341
are not shown in Table 5. One was a cohort study of 20 ART-naïve persons with baseline plasma 342
HIV-1 RNA levels <100,000 copies/mL of whom 18 maintained virological suppression when 343
17
receiving DTG monotherapy for a median of 13 months 35. There was also one dose-finding 10-344
day DTG monotherapy trial, which recruited 28 participants 36. Among those receiving 50 mg 345
daily, the mean reduction in virus load was ~2.5 log copies/ml. No INSTI-resistance mutations or 346
reduction in INSTI susceptibility was observed. 347
Dual therapy in ART-experienced virologically suppressed persons 348
Table 6 lists the 13 studies of virologically suppressed persons on a stable ART regimen 349
switched to DTG dual therapy with either 3TC, rilpivirine (RPV), unboosted atazanavir (ATV), or 350
ritonavir-boosted darunavir (DRV/r). DTG/RPV was used in one randomized clinical trial and in 351
four cohort studies totaling 1,067 persons. The randomized controlled SWORD trial demonstrated 352
that DTG/RPV maintained 95% virological suppression at week 48 in 513 persons and was non-353
inferior to the control arm of continued unchanged ART. DTG/3TC was used in two randomized 354
clinical trials, one single arm pilot trial and three cohort studies totaling 504 persons. DTG/ATV 355
and DTG/DRV/r were each used in one small cohort study. Four studies, which included both 356
virologically suppressed persons and persons with active virus replication were excluded 37–40. 357
In all but three studies, the proportion of persons with VF was at or below 10%, and no 358
person developed INSTI-resistance mutations. The pooled proportion of VF at week 48 was 8.6% 359
(95% CI: 4.8% – 12.3%). The extent of heterogeneity was high with an I2 of 82%. This 360
heterogeneity reflects the different dual drug combinations, the inclusion of cohort studies and 361
clinical trials, and the heterogeneous ART histories of the study subjects. Nonetheless, no person 362
developed INSTI-resistance mutations. 363

18
Monotherapy in ART-experienced virologically suppressed persons 364
There were four clinical trials and four cohort studies in which virologically suppressed 365
persons were treated with DTG monotherapy (Table 7). The four clinical trials included 279 366
persons of whom 26 (9.3%) developed virological failure and 9 (3.2%) developed INSTI-367
resistance mutations over periods ranging from 24 to 48 weeks 20,41–43. The four cohort studies 368
included 113 persons of whom six (5.3%) developed VF and five (4.4%) developed INSTI-369
resistance mutations over periods ranging from 24 to 48 weeks 44–47. 370
The DTG monotherapy arm was discontinued prematurely in three of the four randomized 371
controlled trials because of an increase in VF and INSTI-resistance mutations compared with the 372
control arm either at week 24 42 or between weeks 24 and 48 20,41. The pooled proportion of persons 373
with VF and INSTI-resistance mutations was 2.4% (95% CI: 0.4-4.3 ; I2: 26%) at study 374
termination. However, the raw proportion was 3.6% (i.e. all the cases with VF and INSTI-375
resistance mutations / the total number of treated persons). An analysis of the DOMONO trial 376
reported that a longer duration between the time of HIV-1 diagnosis and ART initiation, a lower 377
CD4 nadir, and a higher peripheral blood mononuclear cell virus level while virologically 378
suppressed were associated with an increased risk of VF during DTG monotherapy 48. 379
ART-experienced INSTI-naïve persons 380
There were two randomized clinical trials, one single arm phase I/II trial, and one cohort 381
study of DTG-containing regimens in non-virologically suppressed, ART-experienced, INSTI-382
naïve persons (Table 8). Pre-therapy genotypic resistance testing was performed on all persons in 383
three clinical trials and on an unspecified proportion of persons in the cohort study. 384
In the DAWNING trial, DTG + 2 NRTIs was superior to ritonavir-boosted lopinavir + 2 385
NRTIs in persons with VF on a first-line NNRTI-containing regimen who were predicted to have 386

19
one fully active NRTI – usually either zidovudine (AZT) or TDF. The overall rate of VF at week 387
48 was 36.2% with two persons (0.6% of subjects) developing one or more INSTI-resistance 388
mutations. 389
In the SAILING trial, DTG plus an optimized background was superior to raltegravir plus 390
an optimized background in persons with a history of resistance to two or more ARV classes who 391
nonetheless had a baseline genotypic resistance test indicating that at least one ARV in addition to 392
DTG or raltegravir was fully active. In the DTG arm, the proportion of persons with VF in this 393
treatment-experienced population was 29.1%. Two persons (0.6% of subjects) developed one or 394
more INSTI-resistance mutations during the 48 week trial 12 while another three (0.8% of subjects) 395
developed such mutations after week 48 13. 396
In the heavily treated adolescent population enrolled in the phase I/II P1093 dose-finding 397
trial, 39% of 23 subjects developed VF by week 48 and one developed emergent INSTI resistance 398
15. A subsequent analysis of two additional treatment cohorts later recruited to the study containing 399
38 additional adolescents identified two additional cases of emergent INSTI resistance, one at 400
week 52 and another at week 192 16. In the single cohort study, the proportion of persons with VF 401
and emergent INSTI-resistance mutations were 16.7% and 0.8%, respectively, after a median of 402
60 weeks 18. 403
The pooled proportion of VF at week 48 was 28.0% (95% CI: 18.6%-37.5%) with a high 404
degree of heterogeneity (I2: 91%) reflecting the lower VF rate in the cohort study compared with 405
the three clinical trials. The pooled proportion of VF plus INSTI-resistance mutations at week 48 406
was 0.7% (95% CI: 0.2%-1.2%; I2: 0%). 407
There were also two randomized controlled trials totaling 242 persons in which DTG plus 408
2 NRTIs was substituted for a ritonavir-boosted protease inhibitor (PI) plus 2 NRTIs in persons 409
with stable virological suppression 49,50. Both trials were performed for the management of PI-410

20
associated toxicities and included no one with a history of NRTI-resistance mutations. VF rates 411
were low and no persons developed INSTI-resistance mutations. One randomized controlled trial 412
substituted DTG plus abacavir/3TC for ongoing therapy in 519 persons who were virologically 413
suppressed on their initial ART-regimen which demonstrating noninferiority of the DTG 414
containing regimen; no person in this study developed INSTI-resistance mutations 51. 415
INSTI-experienced persons 416
One multi-part clinical trial (VIKING cohorts I and II, VIKING-3, and VIKING-4) and 417
one cohort study investigated the response to DTG plus an optimized background in persons with 418
a history of INSTI resistance as a result of previous VF on a raltegravir or elvitegravir-containing 419
regimen 25,52–55 (Table 9). Overall, the VIKING studies included 264 persons and the cohort study 420
included 190 persons. 31% of the 190 persons in the cohort study had previously been enrolled in 421
one of the VIKING studies. DTG 50 mg twice daily (BID) was received in all persons except for 422
a small number of persons in the dose-finding VIKING cohort I trial. In two trials, VIKING cohort 423
II and VIKING-4, a small number of individuals had a period of functional DTG monotherapy 424
lead-in of seven (VIKING-4) to ten (VIKING cohort II) days before the ARVs accompanying 425
DTG were optimized. 426
In nearly all persons in the VIKING trials and in the cohort study, the number of optimized 427
background ARVs predicted to be fully active was low and the overall VF rate was high ranging 428
from 25% to 59% at week 24 and from 39% to 60% at week 48. The VIKING study defined 429
genotypic DTG resistance as Q148H/R/K in combination with one or more of the following 430
accessory DRMs: L74M/I, T97A, E138A/K/T, or G140S/A/C. In an analysis of the 183 person 431
VIKING-3 study, the risk of VF at week 24 was 21% in the absence of a Q148 mutation, 42% in 432

21
the presence of Q148H/R/K plus one accessory mutation, and 76% in the presence of Q148H/R/K 433
and two accessory mutations 53. 434
Using in vitro susceptibility data measured by the PhenoSense assay, there was a VF risk 435
of 24% for persons with viruses having <4-fold reduced DTG susceptibility, 46% for persons with 436
viruses having 4-10-fold reduced susceptibility, and 73% for persons with viruses having >10-fold 437
reduced susceptibility 53. A similar analysis performed by the FDA found that a ³3-fold (rather 438
than 4-fold) reduction in DTG susceptibility was associated with a reduced virological response. 439
The absence of the raw genotypic and phenotypic data from these studies precluded an independent 440
analysis. The VIKING-4 study suggested that the brief functional monotherapy period may have 441
increased the subsequent VF risk even after the background ARVs were optimized 25. 442
The development of INSTI-resistance mutations at VF that were not present at baseline 443
was reported for 26 persons (Table 4). However, the overall proportions of subjects developing 444
additional INSTI-resistance mutations was not provided presumably because all persons in the 445
VIKING trials and the cohort study had INSTI-resistance mutations prior to starting DTG. 446
DISCUSSION 447
DTG-Selected Mutations 448
The mutations developing during in vitro passage were similar to those developing in vivo 449
in INSTI-naïve persons. R263K was the most common mutation in both scenarios. G118R, E138K, 450
and H51Y also occurred both in vitro and in vivo, although E138K and H51Y occurred only in 451
combination with other mutations. S153Y/F occurred commonly in vitro but has not yet been 452
reported in vivo. N155H and Q148 mutations were not selected in vitro but developed in several 453
INSTI-naïve persons, particularly in virologically suppressed persons receiving DTG 454
22
monotherapy. 3’ polypurine tract mutations developed in one in vitro passage experiment and in 455
two of 17 persons with VF on DTG monotherapy. 456
The spectrum of mutations selected by DTG in INSTI-experienced persons differed from 457
the spectrum in INSTI-naïve persons. Of 31 primarily raltegravir-experienced persons with 458
baseline INSTI-resistance mutations, none developed R263K or G118R. Rather, the most common 459
DTG-selected mutations were L74M/I, T97A, E138A/K/T, G140A/S, Q148H/R, and N155H. 460
However, as previously reported for raltegravir, it would be expected that in DTG-treated persons, 461
non-subtype B viruses would be less likely than subtype B viruses to develop Q148 mutations as 462
a result of the requirement in non-subtype B viruses for two nucleotide changes for the key 463
compensatory mutation G140S 56–58. 464
G118R was previously reported in a person receiving raltegravir 59 and R263K was 465
previously selected during in vitro passage with elvitegravir 60. However, these mutations occurred 466
in a much higher proportion of persons with VF on DTG compared with previous studies of VF in 467
persons receiving raltegravir or elvitegravir 5,6. Indeed, no completely novel nonpolymorphic 468
INSTI-selected mutations were identified in persons receiving DTG except for A49G, G149A, and 469
3’ polypurine tract mutations, each of which occurred in two persons. However, as integrase 470
sequences were not available for 61 of 63 viruses from DTG-treated persons with VF and INSTI-471
resistance mutations, it is likely that some DTG-selected mutations were not reported. 472
Effect of INSTI-Resistance Mutations on in vitro DTG Susceptibility 473
R263K alone reduced DTG susceptibility approximately 2-fold while viruses containing 474
R263K plus N155H or Q148R reduced susceptibility 10 to 15-fold. G118R alone generally 475
reduced DTG susceptibility more than 5-fold with higher levels of reduced susceptibility reported 476
in site-directed mutants containing accessory resistance mutations including L74I, T97A, and 477
23
E138K. Both R263K and G118R were associated with reduced enzymatic activity and replication 478
capacity 61–63. The relative rarity of G118R compared with R263K may be due to its usual 479
requirement for mutations at two nucleotides rather than one nucleotide regardless of subtype (i.e., 480
G118R results from a single nucleotide mutation only when the amino acid glycine [G] is encoded 481
by GGA and GGG and not when it is encoded by GGC and GGT) 21. 482
Although N155H was among the most common DTG-selected mutations, it was rarely 483
associated with reduced DTG susceptibility in the absence of R263K or Q148H/R. Q148 mutations 484
alone also had no effect on DTG susceptibility. However, Q148 mutations nearly always occur in 485
combination with other INSTI-resistance mutations. Of 251 isolates in the Stanford HIV Drug 486
Resistance Database with Q148H/R/K, only 14 (5.6%) did not also include a mutation at positions 487
140 or 138. Q148H occurred alone in 3 (1.9%) of its 160 occurrences, Q148R in 11 (15.7%) of its 488
70 occurrences, and Q148K in 0 of its 11 occurrences. 489
In site-directed mutants containing Q148 mutations, reduced susceptibility ranged from 490
approximately 3-fold with the commonly occurring combination Q148H+G140S, 5 to 10-fold with 491
Q148R+G140A/S, and 10 to 20-fold with Q148K+E138K. The greatest levels of reduced DTG 492
susceptibility, often as high as 50-fold, occurred in clinical isolates containing Q148 mutations in 493
combination with mutations at positions 140 and/or 138 and one or more accessory mutations 25–494
27. 495
The greater reduction in susceptibility in clinical compared with laboratory isolates, a 496
phenomenon observed with several established mutation patterns 14,25–27, suggests that 497
unrecognized mutations likely also contribute to reduced DTG susceptibility. The absence of 498
integrase sequences for the majority of the phenotyped clinical isolates precluded an analysis of 499
the potentially novel integrase mutations on reduced DTG susceptibility. 500

24
Virological Efficacy in Populations at Increased Risk for Drug Resistance 501
The risk of VF and INSTI-resistance on a DTG-containing regimen depended on a person’s 502
prior ART experience and the ARVs used in combination with DTG. It likely also depended on 503
whether a person’s virus was actively replicating or stably suppressed on therapy. 504
In ARV-naïve persons without a history of pre-existing drug resistance, standard first-line 505
DTG-containing regimens and DTG/3TC were associated with a very low risk of VF and emergent 506
INSTI resistance. Although DTG/3TC is unlikely to be used in regions without baseline genotypic 507
resistance testing, the success of this regimen indicates that DTG does not require two fully active 508
NRTIs to be highly effective. Data from ARV-experienced persons with stable virological 509
suppression also support this concept as DTG/3TC and DTG/RPV were highly effective dual 510
therapy simplification regimens as summarized here and in a previous meta-analysis of DTG-511
containing dual therapy for treatment simplification 64. Although subjects in the larger of these 512
studies were at low risk of VF (i.e., having no history of VF or of resistance to INSTIs, RPV, or 513
3TC), several of the smaller studies included persons with multiple past VFs including some 514
harboring viruses with reduced 3TC susceptibility. 515
Among 392 virologically suppressed persons in four clinical trials and four cohort studies 516
receiving DTG monotherapy for 24 to 48 weeks, 14 (3.6%) developed VF plus INSTI-resistance 517
mutations. Although this risk is not very high, it is unacceptable because the proportion of persons 518
with virological failure and INSTI resistance increased markedly between weeks 24 and 48 20,41. 519
Further monotherapy studies will therefore be unlikely except possibly for certain populations that 520
appear to be at low risk of VF including those who initiated ART shortly after HIV-1 infection or 521
who had low proviral DNA levels, factors associated with a smaller and less heterogeneous latent 522
virus population 43,48. Finally, the 3.6% risk of VF and emergent resistance over a period of 24 to 523
25
48 weeks may underestimate the risk associated with functional DTG monotherapy in persons with 524
active virological replication rather than stable virological suppression. 525
Our analyses of DTG in virologically suppressed persons (described in the previous two 526
paragraphs and Tables 6 and 7) included 20 studies that overlapped with 19 distinct studies in a 527
recent systematic review of VF during DTG-based mono and dual therapy in virologically 528
suppressed persons 64. We excluded three studies from this previous review including two studies 529
that had fewer than ten persons 66,67 and one that included persons with both virological 530
suppression and active virus replication 39. We included four studies that were not in this previous 531
review 20,68,69. 532
In addition to studies of DTG monotherapy and of DTG plus one active ARV, there were 533
four studies of 941 persons in which DTG was used with NRTIs that may have been compromised 534
by pre-existing NRTI resistance including four studies of ART-experienced, INSTI-naïve persons, 535
in which DTG was used with two NRTIs or an optimized background 12,14,15,18. These studies are 536
relevant to the use of DTG plus two NRTIs in two important clinical scenarios in low- and middle-537
income countries: second-line therapy in persons with confirmed VF on a first-line NNRTI-538
containing regimen and transitioning from a first-line NNRTI-containing regimen to a DTG-539
containing regimen in the absence of a viral load assay confirming virological suppression. 540
In the four reviewed studies of DTG in ARV-experienced INSTI-naïve persons, baseline 541
genotypic resistance testing was available to guide therapy. Indeed, to be eligible for participation 542
in the two largest trials, subjects were required to be placed on at least one ARV that was predicted 543
to be active by genotypic resistance testing 12,14. Genotypic resistance testing, however, is usually 544
not available in low- and middle-income countries. Therefore, the proportion of persons with VF 545
and emergent INSTI resistance during the first 48 weeks of therapy in low- and middle-income 546

26
countries would likely be higher than the 0.7% observed in the reviewed studies in which baseline 547
genotypic resistance testing was performed in an attempt to avoid functional DTG monotherapy. 548
Finally, the studies in which DTG plus an optimized background regimen was used for the 549
treatment of INSTI-experienced persons showed that the Q148 mutational pathway was associated 550
with reduced clinical as well as in vitro DTG susceptibility. These studies also indicated that a 3 551
to 4-fold reduction in DTG susceptibility was associated with a measurably reduced response to 552
therapy compared with full DTG susceptibility. It is not known, however, whether this phenotypic 553
threshold for clinically significant susceptibility also applies to the R263K or G118R mutational 554
pathways. 555
In conclusion, the most common mutations arising in persons with VF on a DTG-556
containing regimen were R263K, G118R, N155H, and Q148H/R. R263K and G118R occurred 557
more commonly than N155H and Q148H/R in previously INSTI-naïve persons. R263K alone 558
reduced DTG susceptibility approximately 2-fold while viruses containing while G118R alone 559
generally reduced DTG susceptibility more than 5-fold. The highest levels of reduced 560
susceptibility occurred in viruses containing Q148 mutations in combination with G140 and/or 561
E138 mutations plus one or more additional accessory INSTI-resistance mutations. Knowledge of 562
DTG-selected mutations and their effects on in vitro susceptibility is, nonetheless, still emerging 563
and remains limited in part because integrase sequences have been published for only 2 of the 63 564
viruses with emergent INSTI resistance in persons receiving DTG and for only 42% of the 177 565
clinical isolates that underwent in vitro susceptibility testing. 566
In INSTI-naïve persons, several DTG-containing two-drug combinations are likely to be 567
highly effective for first-line therapy, treatment simplification, and even salvage therapy provided 568
DTG’s companion drug is fully active. However, actual and functional DTG monotherapy are 569
associated with non-negligible risks of VF and emergent INSTI resistance. These risks have 570

27
implications for the use of DTG plus two NRTIs in NRTI-experienced persons in low- and middle-571
income countries where genotypic resistance testing is not routinely available to guide therapy in 572
persons with VF on a first-line NRTI/NNRTI-containing regimen or where viral load testing may 573
not be available to confirm virological suppression in persons transitioning from a first-line 574
NRTI/NNRTI-containing regimen. Further studies are required to determine the effectiveness of 575
DTG plus two NRTIs in NRTI-experienced persons in low- and middle-income countries. 576
FUNDING 577
S. Y. R., P. L. T., and R.W.S. were supported in part by the National Institute of Allergy 578
and Infectious Diseases (NIAID) of the National Institutes of Health (NIH) (award number 579
AI136618). 580
581
TRANSPARENCY DECLARATIONS 582
R.W.S has received research funding from Janssen Pharmaceuticals and Vela Diagnostics and has 583
consulted for Abbott Diagnostics. 584
585
SUPPLEMENTARY DATA 586
Table S1. Summary of studies containing DTG in vitro susceptibility test results: assays, type of 587
isolates, either site-directed mutants (SDMs) isolates or clinical isolates and number of isolates 588
tested, and SDMs or INSTI-resistance mutations in tested isolates. 589
590
Table S2. Complete set of in vitro DTG susceptibility test results and list of reported mutations. 591
592

28
Table S3. Summary of in vitro DTG susceptibility test results of site-directed mutants according 593
to patterns of INSTI-resistance mutations: number of assays, number of mutants and fold reduced 594
susceptibility. 595
596
29
REFERENCES 597
1. Vitoria M, Hill A, Ford N, et al. The transition to dolutegravir and other new antiretrovirals in 598 low-income and middle-income countries: what are the issues? AIDS Lond Engl 2018; 32: 1551–599 61. 600
2. Dorward J, Lessells R, Drain PK, et al. Dolutegravir for first-line antiretroviral therapy in low-601 income and middle-income countries: uncertainties and opportunities for implementation and 602 research. Lancet HIV 2018; 5: e400–4. 603
3. Meintjes G, Moorhouse MA, Carmona S, et al. Adult antiretroviral therapy guidelines 2017. 604 South Afr J HIV Med 2017; 18: 776. 605
4. World Health Organization. Updated recommendations on first-line and second-line 606 antiretroviral regimens and post-exposure prophylaxis and recommendations on early infant 607 diagnosis of HIV. July 2018. HIV Treatment - Interim Guidance. 608
5. White KL, Raffi F, Miller MD. Resistance analyses of integrase strand transfer inhibitors within 609 phase 3 clinical trials of treatment-naive patients. Viruses 2014; 6: 2858–79. 610
6. Rhee S-Y, Sankaran K, Varghese V, et al. HIV-1 Protease, Reverse Transcriptase, and Integrase 611 Variation Kirchhoff F, ed. J Virol 2016; 90: 6058–70. 612
7. Wensing AM, Calvez V, Günthard HF, et al. 2017 Update of the Drug Resistance Mutations in 613 HIV-1. Top Antivir Med 2017; 24: 132–3. 614
8. Blanco J-L, Varghese V, Rhee S-Y, Gatell JM, Shafer RW. HIV-1 integrase inhibitor resistance 615 and its clinical implications. J Infect Dis 2011; 203: 1204–14. 616
9. Heredia A, Hassounah S, Medina-Moreno S, et al. Monotherapy with either dolutegravir or 617 raltegravir fails to durably suppress HIV viraemia in humanized mice. J Antimicrob Chemother 618 2017; 72: 2570–3. 619
10. Kovarova M, Benhabbour SR, Massud I, et al. Ultra-long-acting removable drug delivery 620 system for HIV treatment and prevention. Nat Commun 2018; 9: 4156. 621
11. Malet I, Subra F, Charpentier C, et al. Mutations Located outside the Integrase Gene Can 622 Confer Resistance to HIV-1 Integrase Strand Transfer Inhibitors. mBio 2017; 8. 623
12. Cahn P, Pozniak AL, Mingrone H, et al. Dolutegravir versus raltegravir in antiretroviral-624 experienced, integrase-inhibitor-naive adults with HIV: week 48 results from the randomised, 625 double-blind, non-inferiority SAILING study. Lancet Lond Engl 2013; 382: 700–8. 626
13. Underwood M, DeAnda F, Dorey D, et al. Resistance post week 48 in ART-experienced, 627 integrase inhibitor-naive subjects with dolutegravir (DTG) vs. raltegravir (RAL) in SAILING 628 (ING111762). In: Presentation of the 13th European Meeting on HIV & Hepatitis Treatment 629 Strategies & Antiviral Drug Resistance, Barcelona, Spain ,2015. 630
30
14. Aboud M, Kaplan R, Lombaard J, et al. Dolutegravir versus ritonavir-boosted lopinavir both 631 with dual nucleoside reverse transcriptase inhibitor therapy in adults with HIV-1 infection in whom 632 first-line therapy has failed (DAWNING): an open-label, non-inferiority, phase 3b trial. Lancet 633 Infect Dis 2019. 634
15. Viani RM, Alvero C, Fenton T, et al. Safety, Pharmacokinetics and Efficacy of Dolutegravir 635 in Treatment-experienced HIV-1 Infected Adolescents: Forty-eight-week Results from IMPAACT 636 P1093. Pediatr Infect Dis J 2015; 34: 1207–13. 637
16. Vavro C, Ruel T, Wiznia A, et al. Emergence of resistance in HIV-1 Integrase (IN) following 638 dolutegravir (DTG) treatment in 6 to 18 year old participants enrolled in the P1093 study. In: 639 Abstracts of the 22nd International AIDS Conference, Amsterdam, the Netherlands 2018. Abstract 640 THPEB114. 641
17. Taiwo BO, Zheng L, Stefanescu A, et al. ACTG A5353: A pilot study of dolutegravir plus 642 lamivudine for initial treatment of HIV-1-infected participants with HIV-1 RNA < 500,000 643 copies/mL. Clin Infect Dis Off Publ Infect Dis Soc Am 2018; 66: 1689–97. 644
18. Lepik KJ, Harrigan PR, Yip B, et al. Emergent drug resistance with integrase strand transfer 645 inhibitor-based regimens. AIDS Lond Engl 2017; 31: 1425–34. 646
19. Wijting IEA, Lungu C, Rijnders BJA, et al. HIV-1 resistance dynamics in patients failing 647 dolutegravir maintenance monotherapy. J Infect Dis 2018; 218: 688–97. 648
20. Hocqueloux L, Raffi F, Prazuck T, et al. Dolutegravir monotherapy versus 649 dolutegravir/abacavir/lamivudine for virologically suppressed people living with chronic HIV 650 infection: the randomized non-inferiority MONCAY trial. Clin Infect Dis Off Publ Infect Dis Soc 651 Am 2019; [Epub ahead of print]. 652
21. Brenner BG, Thomas R, Blanco JL, et al. Development of a G118R mutation in HIV-1 653 integrase following a switch to dolutegravir monotherapy leading to cross-resistance to integrase 654 inhibitors. J Antimicrob Chemother 2016; 71: 1948–53. 655
22. Seatla KK, Avalos A, Moyo S, et al. Four-class drug-resistant HIV-1 subtype C in a treatment 656 experienced individual on dolutegravir-based antiretroviral therapy in Botswana. AIDS Lond Engl 657 2018; 32: 1899–902. 658
23. Hachiya A, Kirby KA, Ido Y, et al. Impact of HIV-1 Integrase L74F and V75I Mutations in a 659 Clinical Isolate on Resistance to Second-Generation Integrase Strand Transfer Inhibitors. 660 Antimicrob Agents Chemother 2017; 61. 661
24. Hardy I, Brenner B, Quashie P, et al. Evolution of a novel pathway leading to dolutegravir 662 resistance in a patient harbouring N155H and multiclass drug resistance. J Antimicrob Chemother 663 2015; 70: 405–11. 664
25. Naeger LK, Harrington P, Komatsu T, Deming D. Effect of dolutegravir functional 665 monotherapy on HIV-1 virological response in integrase strand transfer inhibitor resistant patients. 666 Antivir Ther 2016; 21: 481–8. 667
31
26. Zhang WW, Cheung PK, Oliviera N, Robbins MA, Harrigan PR, Shahid A. Accumulation of 668 multiple mutations in vivo confers cross-resistance to new and existing integrase inhibitors. J 669 Infect Dis 2018; 218: 1773–6. 670
27. George JM, Kuriakose SS, Dee N, et al. Rapid Development of High-Level Resistance to 671 Dolutegravir With Emergence of T97A Mutation in 2 Treatment-Experienced Individuals With 672 Baseline Partial Sensitivity to Dolutegravir. Open Forum Infect Dis 2018; 5: ofy221. 673
28. Malet I, Gimferrer Arriaga L, Artese A, et al. New raltegravir resistance pathways induce broad 674 cross-resistance to all currently used integrase inhibitors. J Antimicrob Chemother 2014; 69: 2118–675 22. 676
29. Pham HT, Labrie L, Wijting IEA, et al. The S230R Integrase Substitution Associated with 677 Viral Rebound during DTG Monotherapy Confers Low Levels INSTI Drug Resistance. J Infect 678 Dis 2018; 218. 679
30. Andreatta KN, Chang S, Martin R, Willkom M, White K. Integrase inhibitor resistance 680 selections initiated with drug resistant HIV-1. In: Abstracts of CROI, Boston, US 2018. Abstract 681 546. 682
31. Yoshinaga T, Kobayashi M, Seki T, et al. Antiviral characteristics of GSK1265744, an HIV 683 integrase inhibitor dosed orally or by long-acting injection. Antimicrob Agents Chemother 2015; 684 59: 397–406. 685
32. Cahn P, Madero JS, Arribas JR, et al. Dolutegravir plus lamivudine versus dolutegravir plus 686 tenofovir disoproxil fumarate and emtricitabine in antiretroviral-naive adults with HIV-1 infection 687 (GEMINI-1 and GEMINI-2): week 48 results from two multicentre, double-blind, randomised, 688 non-inferiority, phase 3 trials. Lancet Lond Engl 2018; 393: 143–55. 689
33. Cahn P, Rolon MJ, Figueroa MI, Gun A, Patterson P, Sued O. Dolutegravir-lamivudine as 690 initial therapy in HIV-1 infected, ARV-naive patients, 48-week results of the PADDLE (Pilot 691 Antiretroviral Design with Dolutegravir LamivudinE) study. J Int AIDS Soc 2017; 20: 21678. 692
34. Nyaku AN, Zheng L, Gulick RM, et al. Dolutegravir plus lamivudine for initial treatment of 693 HIV-1-infected participants with HIV-1 RNA <500 000 copies/mL: week 48 outcomes from 694 ACTG 5353. J Antimicrob Chemother 2019; [Epub ahead of print]. 695
35. Lanzafame M, Nicolè S, Gibellini D, et al. Dolutegravir monotherapy in HIV-infected naive 696 patients with an HIV-RNA load <100 000 copies/mL: a medium-term follow-up. J Antimicrob 697 Chemother 2017; 72: 2136–8. 698
36. Min S, Song I, Borland J, et al. Pharmacokinetics and safety of S/GSK1349572, a next-699 generation HIV integrase inhibitor, in healthy volunteers. Antimicrob Agents Chemother 2010; 54: 700 254–8. 701
37. Capetti AF, Sterrantino G, Cossu MV, et al. Salvage therapy or simplification of salvage 702 regimens with dolutegravir plus ritonavir-boosted darunavir dual therapy in highly cART-703 experienced subjects: an Italian cohort. Antivir Ther 2017; 22: 257–62. 704
32
38. Palacios R, Mayorga M, González-Domenech CM, et al. Safety and Efficacy of Dolutegravir 705 Plus Rilpivirine in Treatment-Experienced HIV-Infected Patients: The DORIVIR Study. J Int 706 Assoc Provid AIDS Care 2018; 17: 2325958218760847. 707
39. Revuelta-Herrero JL, Chamorro-de-Vega E, Rodriguez-Gonzalez CG, Alonso R, Herranz-708 Alonso A, Sanjurjo-Saez M. Effectiveness, Safety, and Costs of a Treatment Switch to 709 Dolutegravir Plus Rilpivirine Dual Therapy in Treatment-Experienced HIV Patients. Ann 710 Pharmacother 2018; 52: 11–8. 711
40. Jabłonowska E, Siwak E, Bociąga-Jasik M, et al. Real-life study of dual therapy based on 712 dolutegravir and ritonavir-boosted darunavir in HIV-1-infected treatment-experienced patients. 713 PloS One 2019; 14: e0210476. 714
41. Wijting I, Rokx C, Boucher C, et al. Dolutegravir as maintenance monotherapy for HIV 715 (DOMONO): a phase 2, randomised non-inferiority trial. Lancet HIV 2017; 4: e547–54. 716
42. Blanco JL, Rojas J, Paredes R, et al. Dolutegravir-based maintenance monotherapy versus dual 717 therapy with lamivudine: a planned 24 week analysis of the DOLAM randomized clinical trial. J 718 Antimicrob Chemother 2018; 73: 1965–71. 719
43. Braun D, Turk T, Hampel B, et al. Simplification to dolutegravir monotherapy is non-inferior 720 compared to continuation of combination antiretroviral therapy in patients who initiated 721 combination antiretroviral therapy during primary HIV infection: A randomized, controlled, non-722 inferiority trial. In: Abstracts of the 22nd International AIDS Conference, Amsterdam, the 723 Netherlands 2018. Abstract TUAB0102. 724
44. Katlama C, Soulie C, Caby F, et al. Dolutegravir as monotherapy in HIV-1-infected individuals 725 with suppressed HIV viraemia. J Antimicrob Chemother 2016; 71: 2646–50. 726
45. Gubavu C, Prazuck T, Niang M, et al. Dolutegravir-based monotherapy or dual therapy 727 maintains a high proportion of viral suppression even in highly experienced HIV-1-infected 728 patients. J Antimicrob Chemother 2016; 71: 1046–50. 729
46. Oldenbuettel C, Wolf E, Ritter A, et al. Dolutegravir monotherapy as treatment de-escalation 730 in HIV-infected adults with virological control: DoluMono cohort results. Antivir Ther 2017; 22: 731 169–72. 732
47. Rojas J, Blanco JL, Marcos MA, et al. Dolutegravir monotherapy in HIV-infected patients 733 with sustained viral suppression. J Antimicrob Chemother 2016; 71: 1975–81. 734
48. Wijting I, Rutsaert S, Rokx C, et al. Predictors of virological failure in HIV-1-infected patients 735 switching to dolutegravir maintenance monotherapy. HIV Med 2018; 20: 63–8. 736
49. Negredo E, Estrada V, Domingo P, et al. Switching from a ritonavir-boosted PI to dolutegravir 737 as an alternative strategy in virologically suppressed HIV-infected individuals. J Antimicrob 738 Chemother 2017; 72: 844–9. 739
50. Gatell JM, Assoumou L, Moyle G, et al. Immediate vs. Deferred Switching from a Boosted 740 Protease Inhibitor (PI/r) Based Regimen to a Dolutegravir (DTG) Based Regimen in Virologically 741

33
Suppressed Patients with High Cardiovascular Risk or Age ≥50 years: Final 96 Weeks Results of 742 NEAT 022 study. Clin Infect Dis Off Publ Infect Dis Soc Am 2018; [Epub ahead of print]. 743
51. Trottier B, Lake JE, Logue K, et al. Dolutegravir/abacavir/lamivudine versus current ART in 744 virally suppressed patients (STRIIVING): a 48-week, randomized, non-inferiority, open-label, 745 Phase IIIb study. Antivir Ther 2017; 22: 295–305. 746
52. Eron JJ, Clotet B, Durant J, et al. Safety and efficacy of dolutegravir in treatment-experienced 747 subjects with raltegravir-resistant HIV type 1 infection: 24-week results of the VIKING Study. J 748 Infect Dis 2013; 207: 740–8. 749
53. Castagna A, Maggiolo F, Penco G, et al. Dolutegravir in antiretroviral-experienced patients 750 with raltegravir- and/or elvitegravir-resistant HIV-1: 24-week results of the phase III VIKING-3 751 study. J Infect Dis 2014; 210: 354–62. 752
54. Castagna A, Ferrara M, Galli L, et al. Long-term efficacy of dolutegravir in treatment-753 experienced subjects failing therapy with HIV-1 integrase strand inhibitor-resistant virus. J 754 Antimicrob Chemother 2018; 73: 177–82. 755
55. Akil B, Blick G, Hagins DP, et al. Dolutegravir versus placebo in subjects harbouring HIV-1 756 with integrase inhibitor resistance associated substitutions: 48-week results from VIKING-4, a 757 randomized study. Antivir Ther 2015; 20: 343–8. 758
56. Fourati S, Charpentier C, Amiel C, et al. Cross-resistance to elvitegravir and dolutegravir in 759 502 patients failing on raltegravir: a French national study of raltegravir-experienced HIV-1-760 infected patients. J Antimicrob Chemother 2015; 70: 1507–12. 761
57. Doyle T, Dunn DT, Ceccherini-Silberstein F, et al. Integrase inhibitor (INI) genotypic 762 resistance in treatment-naive and raltegravir-experienced patients infected with diverse HIV-1 763 clades. J Antimicrob Chemother 2015; 70: 3080–6. 764
58. SECOND-LINE Study Group, Boyd MA, Kumarasamy N, et al. Ritonavir-boosted lopinavir 765 plus nucleoside or nucleotide reverse transcriptase inhibitors versus ritonavir-boosted lopinavir 766 plus raltegravir for treatment of HIV-1 infection in adults with virological failure of a standard 767 first-line ART regimen (SECOND-LINE): a randomised, open-label, non-inferiority study. Lancet 768 Lond Engl 2013; 381: 2091–9. 769
59. Malet I, Fourati S, Charpentier C, et al. The HIV-1 integrase G118R mutation confers 770 raltegravir resistance to the CRF02_AG. J Antimicrob Chemother 2011; 66: 2827–30. 771
60. Margot NA, Hluhanich RM, Jones GS, et al. In vitro resistance selections using elvitegravir, 772 raltegravir, and two metabolites of elvitegravir M1 and M4. Antiviral Res 2012; 93: 288–96. 773
61. Quashie PK, Mesplede T, Han Y-S, et al. Characterization of the R263K mutation in HIV-1 774 integrase that confers low-level resistance to the second-generation integrase strand transfer 775 inhibitor dolutegravir. J Virol 2012; 86: 2696–705. 776
34
62. Quashie PK, Mesplede T, Han Y-S, et al. Biochemical analysis of the role of G118R-linked 777 dolutegravir drug resistance substitutions in HIV-1 integrase. Antimicrob Agents Chemother 2013; 778 57: 6223–35. 779
63. Quashie PK, Oliviera M, Veres T, et al. Differential effects of the G118R, H51Y, and E138K 780 resistance substitutions in different subtypes of HIV integrase. J Virol 2015; 89: 3163–75. 781
64. Wandeler G, Buzzi M, Anderegg N, et al. Virologic failure and HIV drug resistance on 782 simplified, dolutegravir-based maintenance therapy: Systematic review and meta-analysis. 783 F1000Research 2018; 7: 1359. 784
65. Hocqueloux L, Allavena C, Prazuck T, et al. Dolutegravir monotherapy versus 785 dolutegravir/abacavir/lamivudine for HIV-1-infected virologically suppressed patients: Results 786 from the randomized non-inferiority MONCAY trial. In: Abstracts of the 22nd International AIDS 787 Conference, Amsterdam, the Netherlands, 2018. Abstract TUAB0103. 788
66. Rokx C, Schurink CAM, Boucher CAB, Rijnders BJA. Dolutegravir as maintenance 789 monotherapy: first experiences in HIV-1 patients. J Antimicrob Chemother 2016; 71: 1632–6. 790
67. Sculier D, Doco-Lecompte T, Yerly S, Metzner KJ, Decosterd LA, Calmy A. Stable HIV-1 791 reservoirs on dolutegravir maintenance monotherapy: the MONODO study. HIV Med 2018; 792 [Epub ahead of print]. 793
68. Capetti AF, Sterrantino G, Cossu MV, et al. Switch to Dolutegravir plus Rilpivirine Dual 794 Therapy in cART-Experienced Subjects: An Observational Cohort. PloS One 2016; 11: e0164753. 795
69. Braun DL, Turk T, Tschumi F, et al. Non-inferiority of simplified dolutegravir monotherapy 796 compared to continued combination antiretroviral therapy that was initiated during primary HIV 797 infection: a randomized, controlled, multi-site, open-label, non-inferiority trial. Clin Infect Dis Off 798 Publ Infect Dis Soc Am 2019; Epub ahead of print]. 799
70. Oliveira M, Ibanescu R-I, Anstett K, et al. Selective resistance profiles emerging in patient-800 derived clinical isolates with cabotegravir, bictegravir, dolutegravir, and elvitegravir. 801 Retrovirology 2018; 15: 56. 802
803

35
FIGURE LEGENDS
Fig. 1
Flow chart of study selection process. Of 742 studies identified through a PubMed search
performed January 2019 using the search string “Dolutegravir or GSK1349572”, 229 were read in
their entirety following an initial review of titles and abstracts. Following a full text review of these
229 studies and of 35 additional studies from meeting presentations, 95 studies met our inclusion
criteria, containing data on mutations emerging under DTG selection pressure in vitro and in vivo;
in vitro DTG susceptibility; and the risk of virological failure and drug resistance in clinical trials
and cohorts.
Fig. 2
Box plots of in vitro DTG susceptibility results for 176 site-directed mutants and 105 clinical
isolates containing R263K, G118R, N155H, and/or Q148H/R/K. Purple plots indicate the fold
reduced susceptibility for viruses with R263K with or without G118R, N155H, and Q148H/R. Red
plots indicate the fold reduced susceptibility for viruses containing G118R. Yellow plots indicate
the fold reduced susceptibility for viruses containing N155H with or without Q148H/R. Blue plots
indicate the fold reduced susceptibility for viruses containing Q148H/R/K. In addition to the four
signature mutations, mutation patterns were characterized by the number of additional INSTI-
resistance mutations. The number of isolates with each pattern is shown in parentheses.
36
GLOSSARY
Phrase (abbreviation) Definition
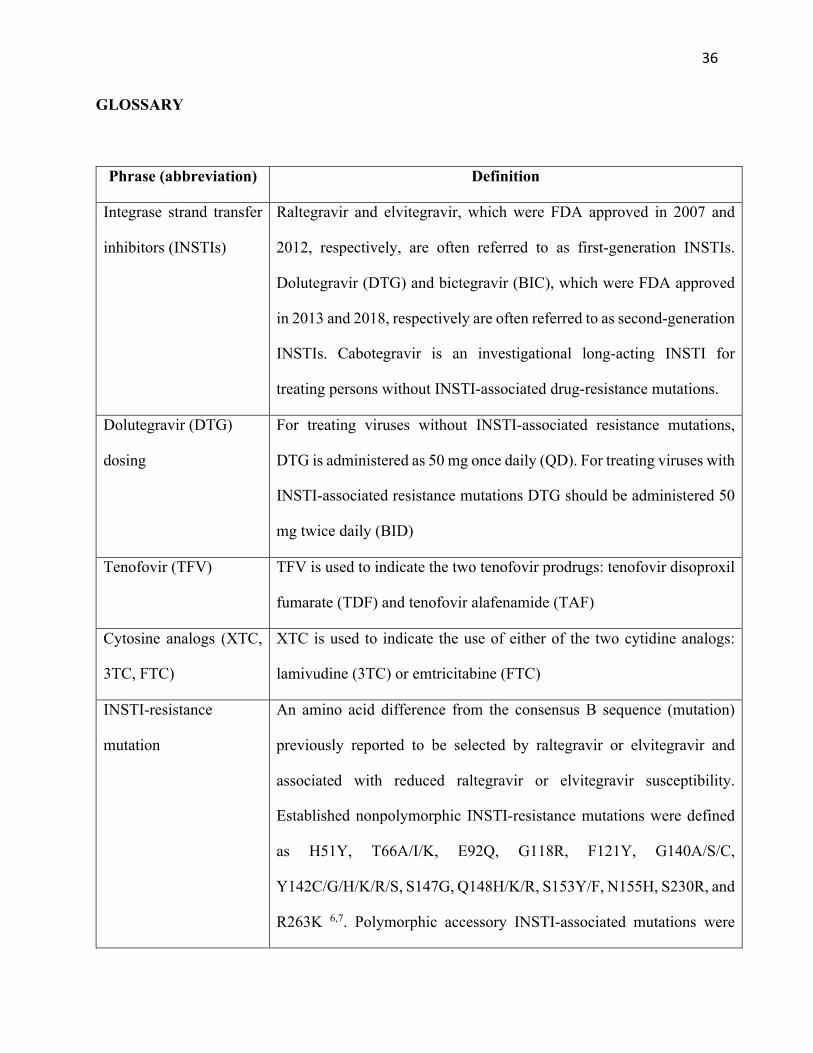
Integrase strand transfer
inhibitors (INSTIs)
Raltegravir and elvitegravir, which were FDA approved in 2007 and
2012, respectively, are often referred to as first-generation INSTIs.
Dolutegravir (DTG) and bictegravir (BIC), which were FDA approved
in 2013 and 2018, respectively are often referred to as second-generation
INSTIs. Cabotegravir is an investigational long-acting INSTI for
treating persons without INSTI-associated drug-resistance mutations.
Dolutegravir (DTG)
dosing
For treating viruses without INSTI-associated resistance mutations,
DTG is administered as 50 mg once daily (QD). For treating viruses with
INSTI-associated resistance mutations DTG should be administered 50
mg twice daily (BID)
Tenofovir (TFV) TFV is used to indicate the two tenofovir prodrugs: tenofovir disoproxil
fumarate (TDF) and tenofovir alafenamide (TAF)
Cytosine analogs (XTC,
3TC, FTC)
XTC is used to indicate the use of either of the two cytidine analogs:
lamivudine (3TC) or emtricitabine (FTC)
INSTI-resistance
mutation
An amino acid difference from the consensus B sequence (mutation)
previously reported to be selected by raltegravir or elvitegravir and
associated with reduced raltegravir or elvitegravir susceptibility.
Established nonpolymorphic INSTI-resistance mutations were defined
as H51Y, T66A/I/K, E92Q, G118R, F121Y, G140A/S/C,
Y142C/G/H/K/R/S, S147G, Q148H/K/R, S153Y/F, N155H, S230R, and
R263K 6,7. Polymorphic accessory INSTI-associated mutations were
37
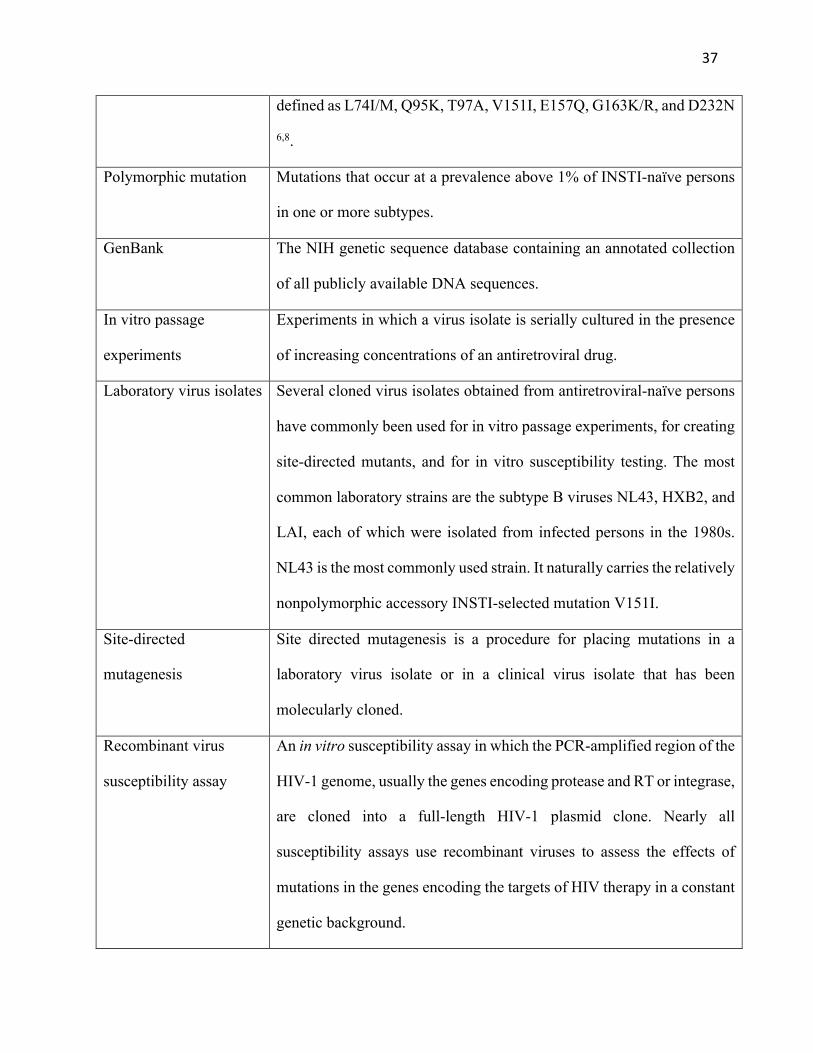
defined as L74I/M, Q95K, T97A, V151I, E157Q, G163K/R, and D232N
6,8.
Polymorphic mutation Mutations that occur at a prevalence above 1% of INSTI-naïve persons
in one or more subtypes.
GenBank The NIH genetic sequence database containing an annotated collection
of all publicly available DNA sequences.
In vitro passage
experiments
Experiments in which a virus isolate is serially cultured in the presence
of increasing concentrations of an antiretroviral drug.
Laboratory virus isolates Several cloned virus isolates obtained from antiretroviral-naïve persons
have commonly been used for in vitro passage experiments, for creating
site-directed mutants, and for in vitro susceptibility testing. The most
common laboratory strains are the subtype B viruses NL43, HXB2, and
LAI, each of which were isolated from infected persons in the 1980s.
NL43 is the most commonly used strain. It naturally carries the relatively
nonpolymorphic accessory INSTI-selected mutation V151I.
Site-directed
mutagenesis
Site directed mutagenesis is a procedure for placing mutations in a
laboratory virus isolate or in a clinical virus isolate that has been
molecularly cloned.
Recombinant virus
susceptibility assay
An in vitro susceptibility assay in which the PCR-amplified region of the
HIV-1 genome, usually the genes encoding protease and RT or integrase,
are cloned into a full-length HIV-1 plasmid clone. Nearly all
susceptibility assays use recombinant viruses to assess the effects of
mutations in the genes encoding the targets of HIV therapy in a constant
genetic background.

38
Cohort A group of people receiving a similar treatment outside of a clinical trial.
The past treatments of individuals in the cohort were often variable. The
cohorts in this review were all retrospective.
Randomized controlled
trial
A clinical trial containing two or more arms in which subjects were
randomized to each arm. In general, the large randomized controlled
trials in this review were double-blinded and placebo controlled;
whereas many of the smaller randomized controlled trials were open-
label.
Stable virological
suppression
Persons in whom plasma HIV-1 RNA levels were below 50 copies/ml
on two or more occasions for a period of six months or longer in the
absence of a change in ART.
Optimized background
The ARVs selected by the a clinical trial subject’s care provider to be
used in combination with DTG. This is also commonly referred to as
optimal backbone.
Virological failure
Virological failure was defined across all studies using an intention-to-
treat approach such that subjects discontinuing therapy for any reason
such as intolerance or nonadherence were categorized as experiencing
virological failure. This approach was adopted both for studies that
reported their results in this manner and for those that employed a
narrower definition of protocol-defined virological failure, typically a
confirmed or repeated plasma HIV-1 RNA level ³50 copies/ml.
39
Table 1. HIV-1 group M viruses developing IN mutations during in vitro passage
experiments*
AuthorYr Parent Virus† 51
H
66
T
92
E
118
G
138
E
140
G
147
S
148
Q
153
S
263
R
Kobayashi11 NL43
F/Y
Quashie12 Clinical (n=3)
K
Clinical
K
K
Clinical
Y K
Clinical (C) Y
R
Clinical (C) Y
T
Clinical (02)
R
Clinical (02) Y
K
Oliveira14 NL43
K
NL43-118R
I
K
NL43-51Y/263K
K
Anstett15
NL43
K
NL43-92Q
K
NL43-140S
R
NL43-140S/148R Y
NL43-155H
K
Departureaux15 NL43
Y
Seki15 NL43
Q
NL43-148H
K S
NL43-148K
K
NL43-148R
K S
Brenner16 NL43-118R
I
K
Clinical-118R (C)
A
K
Oliveira16 NL43
F K
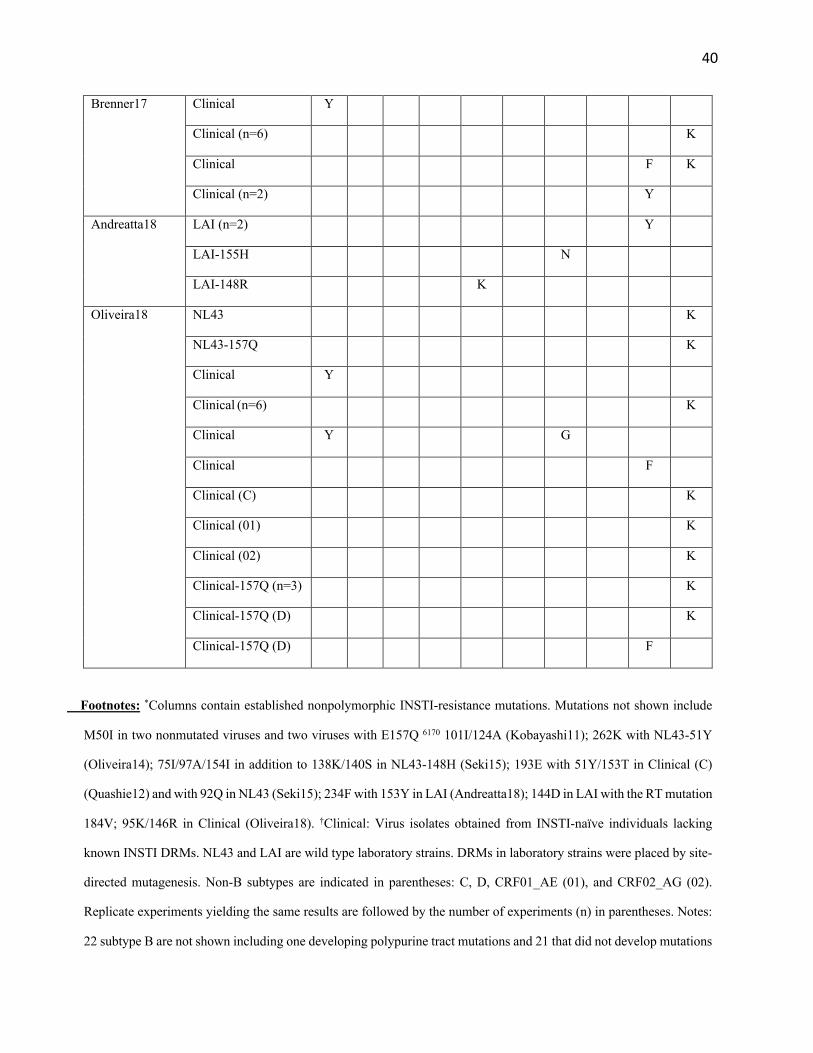
40
Brenner17 Clinical Y
Clinical (n=6)
K
Clinical
F K
Clinical (n=2)
Y
Andreatta18
LAI (n=2)
Y
LAI-155H
N
LAI-148R
K
Oliveira18 NL43
K
NL43-157Q
K
Clinical Y
Clinical (n=6)
K
Clinical Y
G
Clinical
F
Clinical (C)
K
Clinical (01)
K
Clinical (02)
K
Clinical-157Q (n=3)
K
Clinical-157Q (D)
K
Clinical-157Q (D)
F
Footnotes: *Columns contain established nonpolymorphic INSTI-resistance mutations. Mutations not shown include
M50I in two nonmutated viruses and two viruses with E157Q 6170 101I/124A (Kobayashi11); 262K with NL43-51Y
(Oliveira14); 75I/97A/154I in addition to 138K/140S in NL43-148H (Seki15); 193E with 51Y/153T in Clinical (C)
(Quashie12) and with 92Q in NL43 (Seki15); 234F with 153Y in LAI (Andreatta18); 144D in LAI with the RT mutation
184V; 95K/146R in Clinical (Oliveira18). †Clinical: Virus isolates obtained from INSTI-naïve individuals lacking
known INSTI DRMs. NL43 and LAI are wild type laboratory strains. DRMs in laboratory strains were placed by site-
directed mutagenesis. Non-B subtypes are indicated in parentheses: C, D, CRF01_AE (01), and CRF02_AG (02).
Replicate experiments yielding the same results are followed by the number of experiments (n) in parentheses. Notes:
22 subtype B are not shown including one developing polypurine tract mutations and 21 that did not develop mutations

41
including those with parent viruses 92Q (2), 92Q/155H (1), 51Y/118R (1), 143C (1), 143R (1), 148R (1), 155H (1),
263K (2), RT-65R (1), RT-184V/I (2), and 8 without mutations.
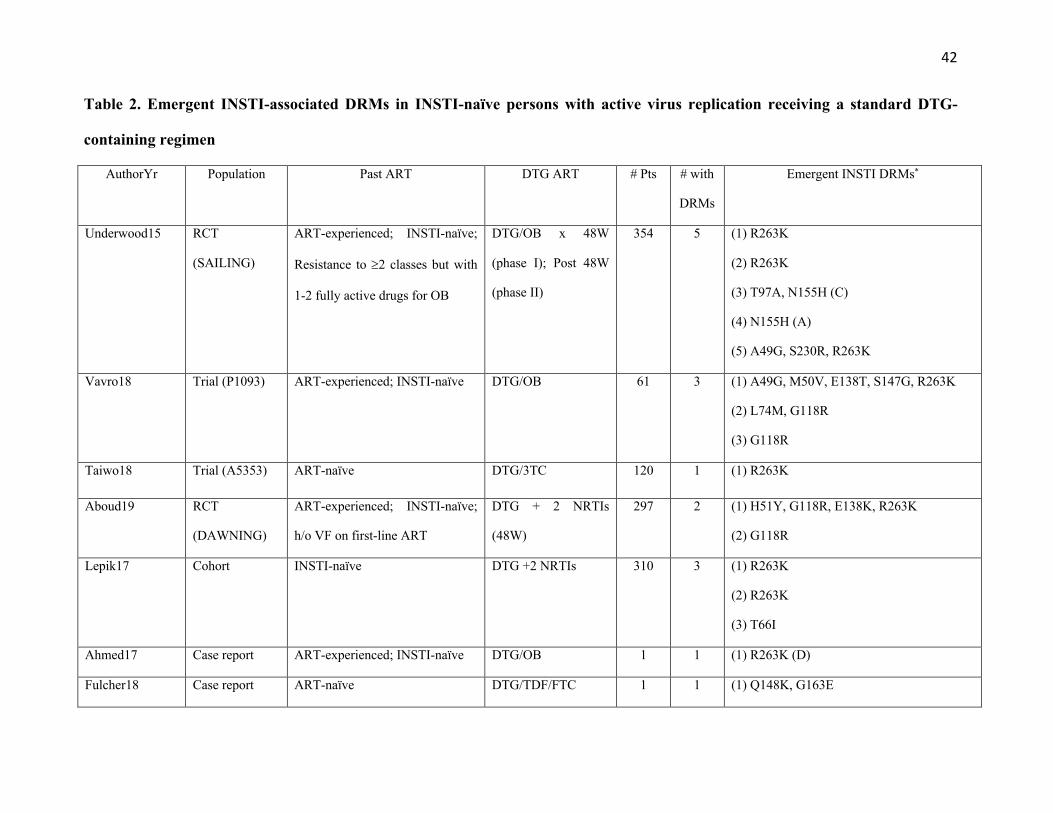
42
Table 2. Emergent INSTI-associated DRMs in INSTI-naïve persons with active virus replication receiving a standard DTG-
containing regimen
AuthorYr Population Past ART DTG ART # Pts # with
DRMs
Emergent INSTI DRMs*
Underwood15 RCT
(SAILING)
ART-experienced; INSTI-naïve;
Resistance to ³2 classes but with
1-2 fully active drugs for OB
DTG/OB x 48W
(phase I); Post 48W
(phase II)
354
5 (1) R263K
(2) R263K
(3) T97A, N155H (C)
(4) N155H (A)
(5) A49G, S230R, R263K
Vavro18 Trial (P1093) ART-experienced; INSTI-naïve DTG/OB 61 3 (1) A49G, M50V, E138T, S147G, R263K
(2) L74M, G118R
(3) G118R
Taiwo18 Trial (A5353) ART-naïve DTG/3TC 120 1 (1) R263K
Aboud19 RCT
(DAWNING)
ART-experienced; INSTI-naïve;
h/o VF on first-line ART
DTG + 2 NRTIs
(48W)
297 2 (1) H51Y, G118R, E138K, R263K
(2) G118R
Lepik17 Cohort INSTI-naïve DTG +2 NRTIs 310 3 (1) R263K
(2) R263K
(3) T66I
Ahmed17 Case report ART-experienced; INSTI-naïve DTG/OB 1 1 (1) R263K (D)
Fulcher18 Case report ART-naïve DTG/TDF/FTC 1 1 (1) Q148K, G163E

43
Pena Lopez18 Case report ART-naïve DTG/TDF/FTC 1 1 (1) E157Q, R263K (CRF14_BG)
Seatla18 Case report ART-experienced; INSTI-naïve DTG/OB 1 1 (1) G118R, E138K
Cardoso18 Case report ART-experienced; INSTI-naïve DTG + 2 NRTIs 2 2 (1) E157Q, R263K
(2) R263K (G)
Lubke18 Case report ART-naïve DTG/TDF/FTC 1 1 (1) G118R, R263K (F)
Footnote: Abbreviations: RCT: randomized clinical trial; OB: optimized background; VF: virological failure; DRMs: drug-resistance mutations. *Subtypes are indicated
in parentheses. In Underwood15, the two cases of R263K were reported in the first 48 weeks of the SAILING trial 12. The three additional cases of INSTI DRMs in this
trial occurred between weeks 72 and 120. In Want19, the first isolate contained 3 clones with H51Y/G118R and 11 clones with G118R/E138K/R263K. In Lepik17,
R263K was detected in two ART-experienced persons and T66I detected in a previously ART-naïve person. In Pena Lopez18, DTG was administered BID in a person
who was also receiving rifampin. Complete sequences were unavailable for all isolates in this table.
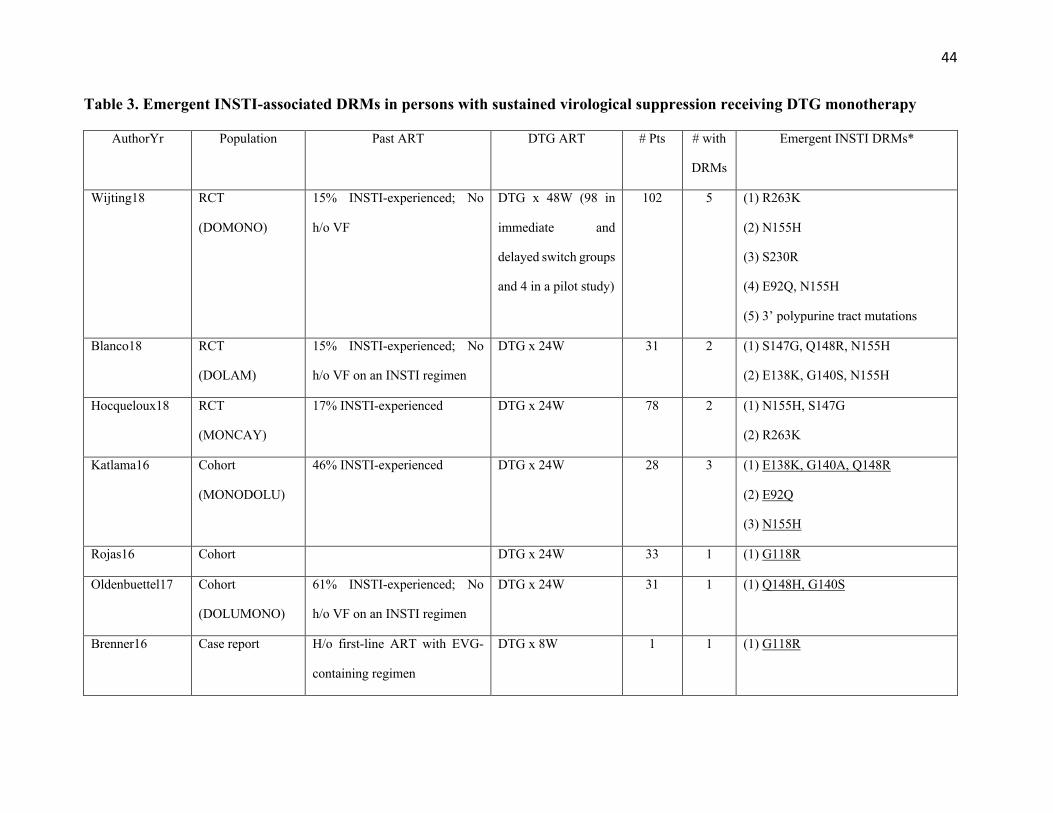
44
Table 3. Emergent INSTI-associated DRMs in persons with sustained virological suppression receiving DTG monotherapy
AuthorYr
Population Past ART DTG ART # Pts # with
DRMs
Emergent INSTI DRMs*
Wijting18 RCT
(DOMONO)
15% INSTI-experienced; No
h/o VF
DTG x 48W (98 in
immediate and
delayed switch groups
and 4 in a pilot study)
102 5 (1) R263K
(2) N155H
(3) S230R
(4) E92Q, N155H
(5) 3’ polypurine tract mutations
Blanco18 RCT
(DOLAM)
15% INSTI-experienced; No
h/o VF on an INSTI regimen
DTG x 24W 31 2 (1) S147G, Q148R, N155H
(2) E138K, G140S, N155H
Hocqueloux18 RCT
(MONCAY)
17% INSTI-experienced DTG x 24W 78 2
(1) N155H, S147G
(2) R263K
Katlama16 Cohort
(MONODOLU)
46% INSTI-experienced DTG x 24W 28 3 (1) E138K, G140A, Q148R
(2) E92Q
(3) N155H
Rojas16 Cohort DTG x 24W 33 1 (1) G118R
Oldenbuettel17 Cohort
(DOLUMONO)
61% INSTI-experienced; No
h/o VF on an INSTI regimen
DTG x 24W 31 1 (1) Q148H, G140S
Brenner16 Case report H/o first-line ART with EVG-
containing regimen
DTG x 8W 1 1 (1) G118R

45
Malet18 Case report RAL-experienced DTG 1 1 (1) N155H
Footnote: Abbreviations: RCT: randomized clinical trial; VF: virological failure; RAL: raltegravir; EVG: elvitegravir; DRMs: drug-resistance mutations. *Underlined
mutations indicate that the virus emerged in an INSTI-experienced person. In Wijting18, R263K, N155H and S230R detected in persons in the main DOMONO
study which required a nadir CD4 count greater than 200 (Wijting17); whereas E92Q/N155H and 3’ polypurine tract mutations occurred in four persons in the pilot
DOMONO study which included persons with a nadir CD4 count below 200. The virus with R263K reported by Hocqueloux16 also had a single G to A mutation in
the 3’ polypurine tract whereas two of the six nucleotides in the 3’ polypurine tract were mutated in Wijting18. The G118R mutation in Rojas16 was detected as a
minority variant in 7% of viruses by next-generation sequencing. Complete sequences were unavailable for all sequences except Brenner16

46
Table 4. Emergent INSTI-resistance mutations in INSTI-experienced persons receiving DTG in combination with an optimized
background (OB) regimen
AuthorYr Population DTG ART Time
to VF
Pre-DTG DRMs Emergent INSTI DRMs
Eron13 RCT (VIKING) Cohort I
(50mg QD)
Day11 G140S, Y143H, Q148H L74I/M, E138A
Day11 L74M, T97A, Y143R, G163R E138K
W8 None L74I/M, T97A, G140S, Q148H
W24 L74M, T97A, E138A, Y143R N155H
W24 L74M, T97A, Y143R N155H
Cohort II
(50mg BID)
Day11 E138A, G140S, Q148H T97A, E138T
Day11 G140S, Q148H N155H
Day11 E138K, G140S, Q148H T97A
W8 E138A, G140S, Q148H E92Q, T97A
W8 G140S, Q148H E138K, N155H
W16 G140S, Q148H T97A, E138K, N155H
Naeger16 RCT
(VIKING-4)
DTG 50 mg BID + OB
W12 E138D, G140S, Q148H L74M, G149A, N155H
W24 G140S, Q148H T97A, E138K, G149A
W24 E138A/K/T, G140S, Q148H T97A
W24 L74M, Q95K, T97A, Y143C E138K, S147G
W4 G140S, Q148H T97A
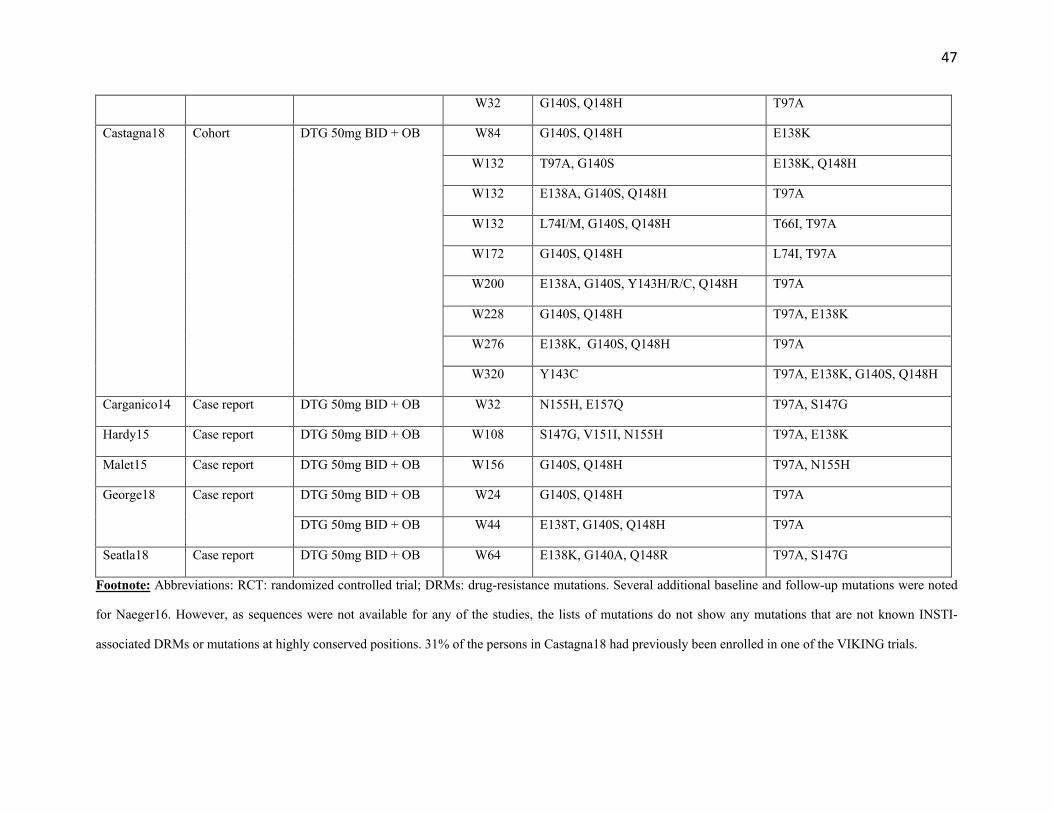
47
W32 G140S, Q148H T97A
Castagna18 Cohort DTG 50mg BID + OB W84 G140S, Q148H E138K
W132 T97A, G140S E138K, Q148H
W132 E138A, G140S, Q148H T97A
W132 L74I/M, G140S, Q148H T66I, T97A
W172 G140S, Q148H L74I, T97A
W200 E138A, G140S, Y143H/R/C, Q148H T97A
W228 G140S, Q148H T97A, E138K
W276 E138K, G140S, Q148H T97A
W320 Y143C T97A, E138K, G140S, Q148H
Carganico14 Case report DTG 50mg BID + OB W32 N155H, E157Q T97A, S147G
Hardy15 Case report DTG 50mg BID + OB W108 S147G, V151I, N155H T97A, E138K
Malet15 Case report DTG 50mg BID + OB W156 G140S, Q148H T97A, N155H
George18 Case report DTG 50mg BID + OB W24 G140S, Q148H T97A
DTG 50mg BID + OB W44 E138T, G140S, Q148H T97A
Seatla18 Case report DTG 50mg BID + OB W64 E138K, G140A, Q148R T97A, S147G
Footnote: Abbreviations: RCT: randomized controlled trial; DRMs: drug-resistance mutations. Several additional baseline and follow-up mutations were noted
for Naeger16. However, as sequences were not available for any of the studies, the lists of mutations do not show any mutations that are not known INSTI-
associated DRMs or mutations at highly conserved positions. 31% of the persons in Castagna18 had previously been enrolled in one of the VIKING trials.
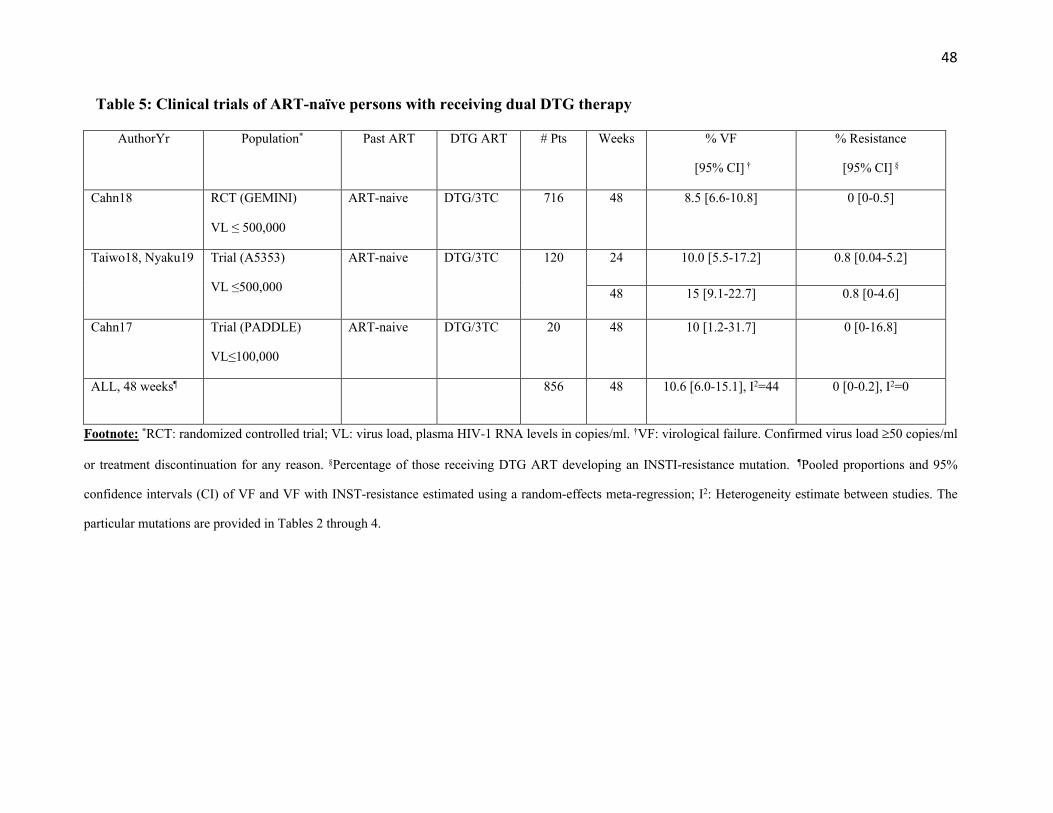
48
Table 5: Clinical trials of ART-naïve persons with receiving dual DTG therapy
AuthorYr
Population* Past ART DTG ART # Pts Weeks % VF
[95% CI] †
% Resistance
[95% CI] §
Cahn18 RCT (GEMINI)
VL ≤ 500,000
ART-naive DTG/3TC 716 48 8.5 [6.6-10.8]
0 [0-0.5]
Taiwo18, Nyaku19 Trial (A5353)
VL ≤500,000
ART-naive DTG/3TC 120 24 10.0 [5.5-17.2] 0.8 [0.04-5.2]
48 15 [9.1-22.7] 0.8 [0-4.6]
Cahn17 Trial (PADDLE)
VL≤100,000
ART-naive DTG/3TC 20 48 10 [1.2-31.7] 0 [0-16.8]
ALL, 48 weeks¶ 856 48 10.6 [6.0-15.1], I2=44 0 [0-0.2], I2=0
Footnote: *RCT: randomized controlled trial; VL: virus load, plasma HIV-1 RNA levels in copies/ml. †VF: virological failure. Confirmed virus load ³50 copies/ml
or treatment discontinuation for any reason. §Percentage of those receiving DTG ART developing an INSTI-resistance mutation. ¶Pooled proportions and 95%
confidence intervals (CI) of VF and VF with INST-resistance estimated using a random-effects meta-regression; I2: Heterogeneity estimate between studies. The
particular mutations are provided in Tables 2 through 4.
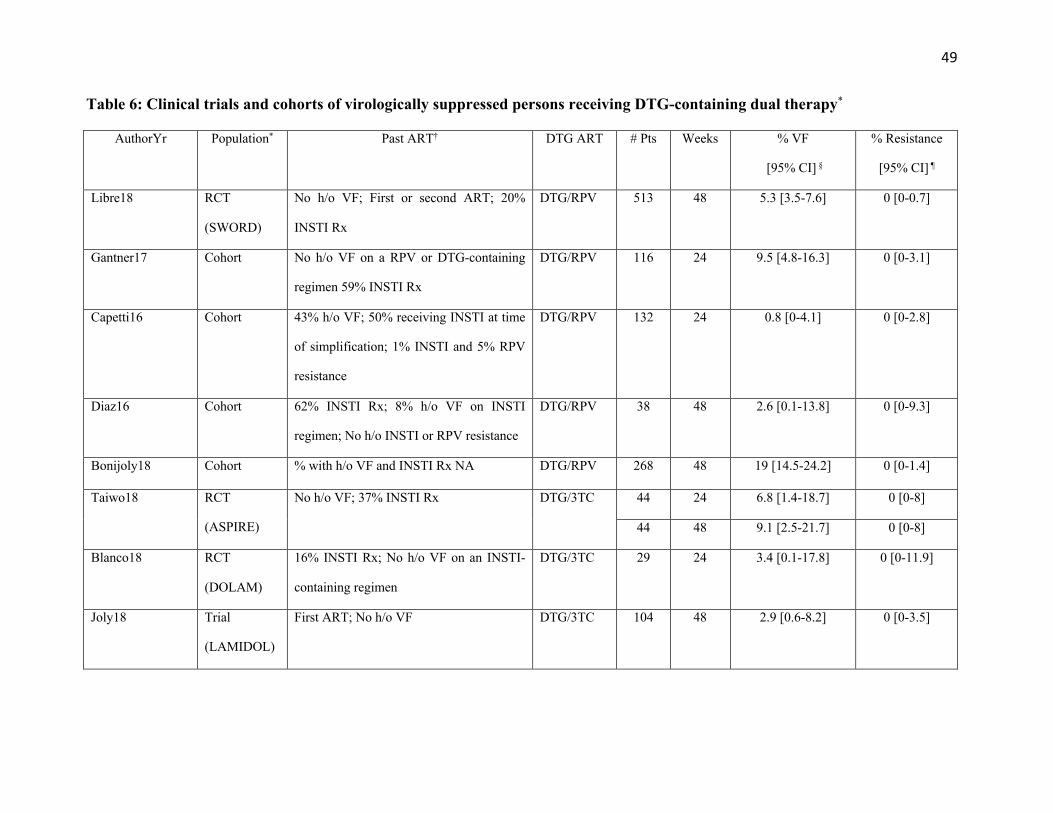
49
Table 6: Clinical trials and cohorts of virologically suppressed persons receiving DTG-containing dual therapy*
AuthorYr Population* Past ART†
DTG ART # Pts Weeks % VF
[95% CI] §
% Resistance
[95% CI] ¶
Libre18
RCT
(SWORD)
No h/o VF; First or second ART; 20%
INSTI Rx
DTG/RPV 513 48 5.3 [3.5-7.6]
0 [0-0.7]
Gantner17
Cohort No h/o VF on a RPV or DTG-containing
regimen 59% INSTI Rx
DTG/RPV 116 24 9.5 [4.8-16.3]
0 [0-3.1]
Capetti16
Cohort 43% h/o VF; 50% receiving INSTI at time
of simplification; 1% INSTI and 5% RPV
resistance
DTG/RPV 132 24 0.8 [0-4.1] 0 [0-2.8]
Diaz16 Cohort 62% INSTI Rx; 8% h/o VF on INSTI
regimen; No h/o INSTI or RPV resistance
DTG/RPV 38 48 2.6 [0.1-13.8] 0 [0-9.3]
Bonijoly18 Cohort % with h/o VF and INSTI Rx NA DTG/RPV 268 48 19 [14.5-24.2] 0 [0-1.4]
Taiwo18 RCT
(ASPIRE)
No h/o VF; 37% INSTI Rx DTG/3TC 44 24 6.8 [1.4-18.7] 0 [0-8]
44 48 9.1 [2.5-21.7] 0 [0-8]
Blanco18 RCT
(DOLAM)
16% INSTI Rx; No h/o VF on an INSTI-
containing regimen
DTG/3TC 29 24 3.4 [0.1-17.8] 0 [0-11.9]
Joly18 Trial
(LAMIDOL)
First ART; No h/o VF DTG/3TC 104 48 2.9 [0.6-8.2] 0 [0-3.5]

50
Maggiolo17 Cohort 15% INSTI Rx at simplification; % with
past VF NA; No h/o INSTI or 3TC
resistance
DTG/3TC 94 24 0 [0-3.8] 0 [0-3.8]
Borghetti18 Cohort 16% INSTI Rx at simplification; No h/o VF
on INSTI regimen; 6% had h/o M184I/V
DTG/3TC 206 48 13.1 [8.8-18.5] 0 [0-1.8]
Reynes17 Cohort
(DOLULAM)
26% h/o INSTI Rx at simplification; No h/o
INSTI resistance; 37% had h/o MI84V
DTG/3TC 27 48 11.1 [2.4-29.2] 0 [0-12.8]
Castagna17 Cohort 43% INSTI at simplification; % past INSTI
resistance NA
DTG/ATV 116 48 8.6 [4.2-15.3] 0 [0-3.1]
Navarro17 Cohort 15% h/o VF on an INSTI regimen; No h/o
INSTI-resistance
DTG/DRVr 27 48 7.4 [0.9-24.3] 0 [0-12.8]
ALL, 24 weeksY 415 24 2.6 [0.01-5.2], I2=72 0 [0-0.7], I2=0
ALL, 48 weeksY 1,343 48 8.6[4.8-12.3], I2=82 0 [0-0.2], I2=0
Footnotes: *Virologically suppressed persons: persons with plasma HIV-1 RNA levels £50 copies/ml on two or more occasions for a period of ³6 months in the
absence of a change in ART; RCT: randomized controlled trial; †Past ART: Where available this column includes the following: (i) number of previous regimens;
(ii) Extent of INSTI exposure (Rx); (iii) % with past virological failure: and (iv) % with past INSTI resistance or resistance to the ARV used with DTG. §VF:
virological failure. Confirmed virus load ³50 copies/ml or treatment discontinuation for any reason. For the cohort study, the proportion of persons with VF after the
median time of follow-up was provided. ¶Percentage of those receiving DTG ART developing an INSTI-resistance mutation. YPooled proportions and 95% confidence
intervals (CI) of VF and VF with INST-resistance estimated using a random-effects meta-regression; I2: Heterogeneity estimate between studies. The particular
51
mutations are provided in Tables 2 through 4. Reynes17 and Borghetti18 also had week 96 follow up. In Borghtetti18, the VF rate increased to 20% at week 96, The
median number of weeks of follow-up was 48 and 51, respectively, in Navarro17 and Castagna17.
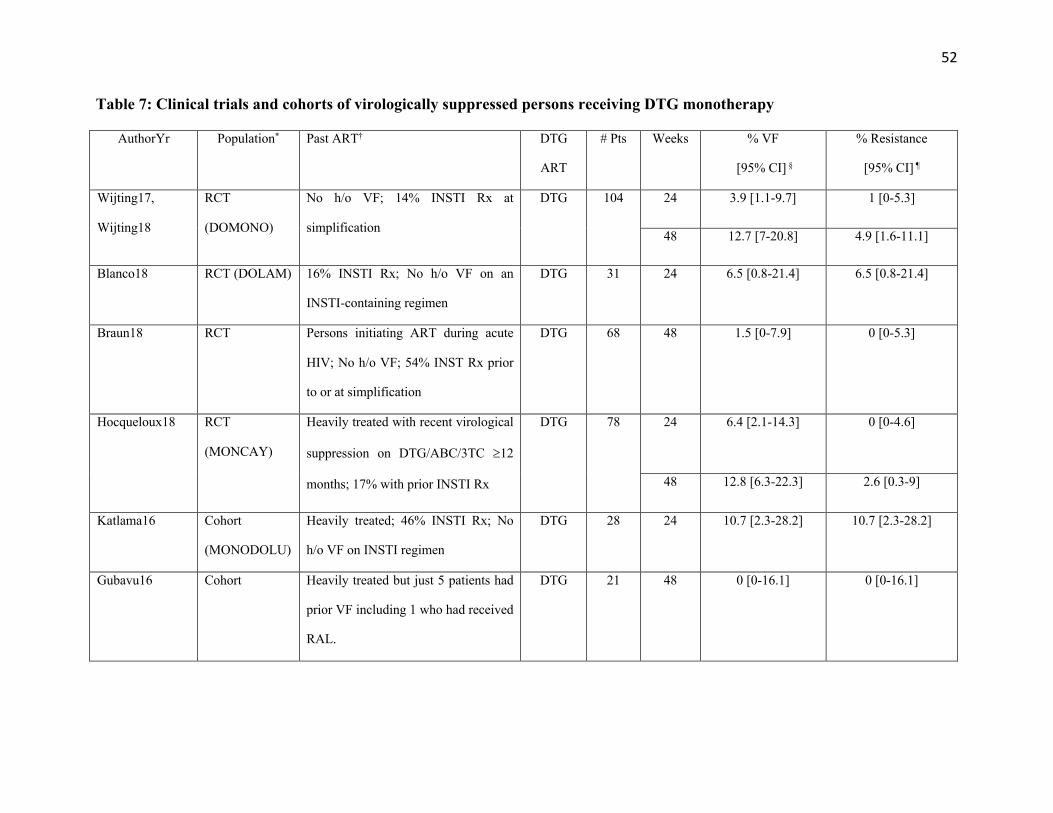
52
Table 7: Clinical trials and cohorts of virologically suppressed persons receiving DTG monotherapy
AuthorYr
Population* Past ART† DTG
ART
# Pts Weeks % VF
[95% CI] §
% Resistance
[95% CI] ¶
Wijting17,
Wijting18
RCT
(DOMONO)
No h/o VF; 14% INSTI Rx at
simplification
DTG 104 24 3.9 [1.1-9.7] 1 [0-5.3]
48 12.7 [7-20.8] 4.9 [1.6-11.1]
Blanco18
RCT (DOLAM) 16% INSTI Rx; No h/o VF on an
INSTI-containing regimen
DTG 31 24 6.5 [0.8-21.4]
6.5 [0.8-21.4]
Braun18
RCT Persons initiating ART during acute
HIV; No h/o VF; 54% INST Rx prior
to or at simplification
DTG 68 48 1.5 [0-7.9] 0 [0-5.3]
Hocqueloux18 RCT
(MONCAY)
Heavily treated with recent virological
suppression on DTG/ABC/3TC ³12
months; 17% with prior INSTI Rx
DTG 78 24 6.4 [2.1-14.3] 0 [0-4.6]
48 12.8 [6.3-22.3] 2.6 [0.3-9]
Katlama16
Cohort
(MONODOLU)
Heavily treated; 46% INSTI Rx; No
h/o VF on INSTI regimen
DTG 28 24 10.7 [2.3-28.2] 10.7 [2.3-28.2]
Gubavu16 Cohort Heavily treated but just 5 patients had
prior VF including 1 who had received
RAL.
DTG 21
48 0 [0-16.1] 0 [0-16.1]

53
Oldenbuettel17
Cohort
(DOLUMONO)
32% INSTI rx; No h/o VF on INSTI or
INSTI resistance
DTG 31 24 6.5 [0.8-21.4] 3.2 [0.1-16.7]
Rojas16 Cohort Heavily treated; % with past INSTI rx
or past VF not provided
DTG 33 24 3 [0.1-15.8] 3 [0.1-15.8]
ALL, 24 weeksY 303 24 5.0 [2.5-7.4], I2=0 1.3 [0-2.9], I2=23
ALL, 48 weeksY 269 48 6.3 [0-12.9], I2=82 1.7 [0-4.0], I2=41
ALL, study
terminationY 392 6.0 [2.2-9.8], I2=63 2.4 [0.4-4.3], I2=26
Footnote: *Virologically suppressed persons: plasma HIV-1 RNA levels £50 copies/ml on two or more occasions for a period of ³6 months in the absence of a
change in ART. RCT: randomized controlled trial; †Past ART: Where available this column includes the following: (i) number of previous regimens; (ii) Extent of
INSTI exposure (Rx); (iii) % with past VF: and (iv) % with past INSTI resistance or resistance to the ARV used with DTG. §VF: Confirmed virus load ³50
copies/ml or treatment discontinuation for any reason. For the cohort studies, the proportion of persons with VF after the median time of follow-up was provided.
¶Percentage of those receiving DTG ART developing an INSTI-resistance mutation. YPooled proportions and 95% confidence intervals (CI) of VF and VF with
INST-resistance estimated using a random-effects meta-regression; I2: Heterogeneity estimate between studies. The particular mutations are summarized in Table
3. Four of the subjects in the DOMONO trial, including two with VF and resistance, were in a pilot trial that included persons with a CD4 count nadir <200 whereas
those in the main trial had a CD4 count nadir >200 (Wijting18). Two cohort studies with 5 66 and 8 67 subjects did not meet inclusion criteria.
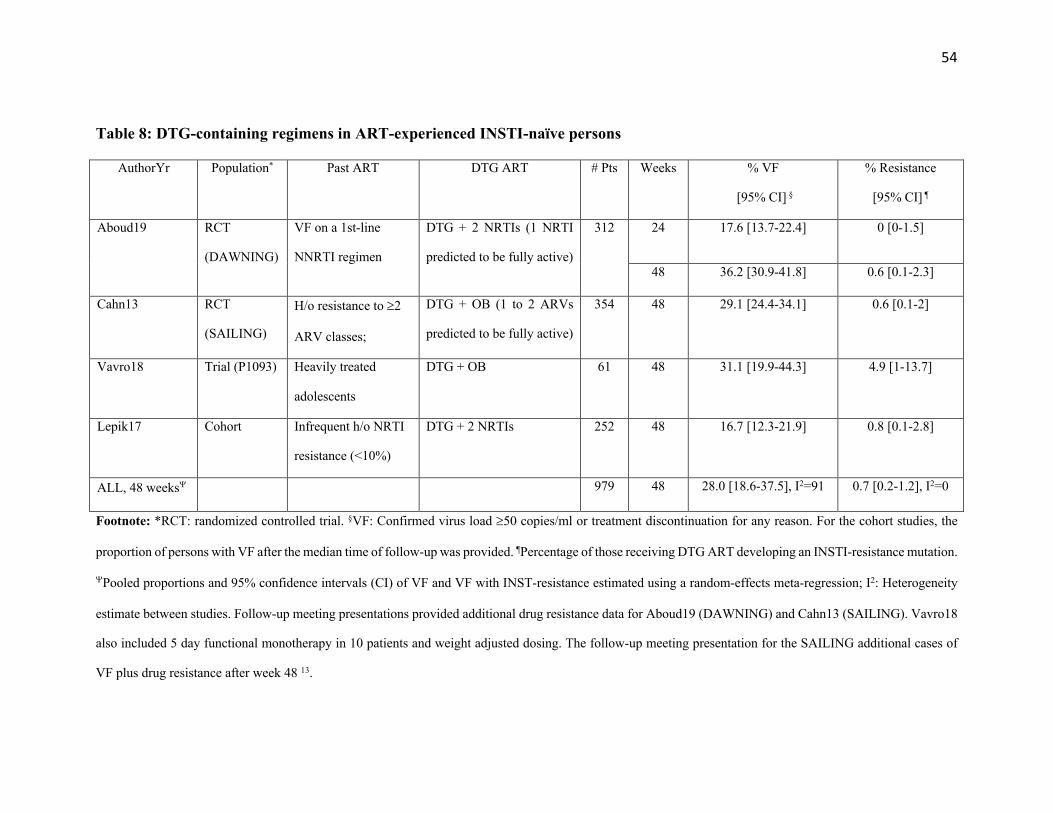
54
Table 8: DTG-containing regimens in ART-experienced INSTI-naïve persons
AuthorYr
Population* Past ART DTG ART # Pts Weeks % VF
[95% CI] §
% Resistance
[95% CI] ¶
Aboud19
RCT
(DAWNING)
VF on a 1st-line
NNRTI regimen
DTG + 2 NRTIs (1 NRTI
predicted to be fully active)
312 24 17.6 [13.7-22.4] 0 [0-1.5]
48 36.2 [30.9-41.8] 0.6 [0.1-2.3]
Cahn13
RCT
(SAILING)
H/o resistance to ³2
ARV classes;
DTG + OB (1 to 2 ARVs
predicted to be fully active)
354 48 29.1 [24.4-34.1] 0.6 [0.1-2]
Vavro18 Trial (P1093) Heavily treated
adolescents
DTG + OB 61 48 31.1 [19.9-44.3] 4.9 [1-13.7]
Lepik17 Cohort Infrequent h/o NRTI
resistance (<10%)
DTG + 2 NRTIs 252 48 16.7 [12.3-21.9] 0.8 [0.1-2.8]
ALL, 48 weeksY 979 48 28.0 [18.6-37.5], I2=91 0.7 [0.2-1.2], I2=0
Footnote: *RCT: randomized controlled trial. §VF: Confirmed virus load ³50 copies/ml or treatment discontinuation for any reason. For the cohort studies, the
proportion of persons with VF after the median time of follow-up was provided. ¶Percentage of those receiving DTG ART developing an INSTI-resistance mutation.
YPooled proportions and 95% confidence intervals (CI) of VF and VF with INST-resistance estimated using a random-effects meta-regression; I2: Heterogeneity
estimate between studies. Follow-up meeting presentations provided additional drug resistance data for Aboud19 (DAWNING) and Cahn13 (SAILING). Vavro18
also included 5 day functional monotherapy in 10 patients and weight adjusted dosing. The follow-up meeting presentation for the SAILING additional cases of
VF plus drug resistance after week 48 13.
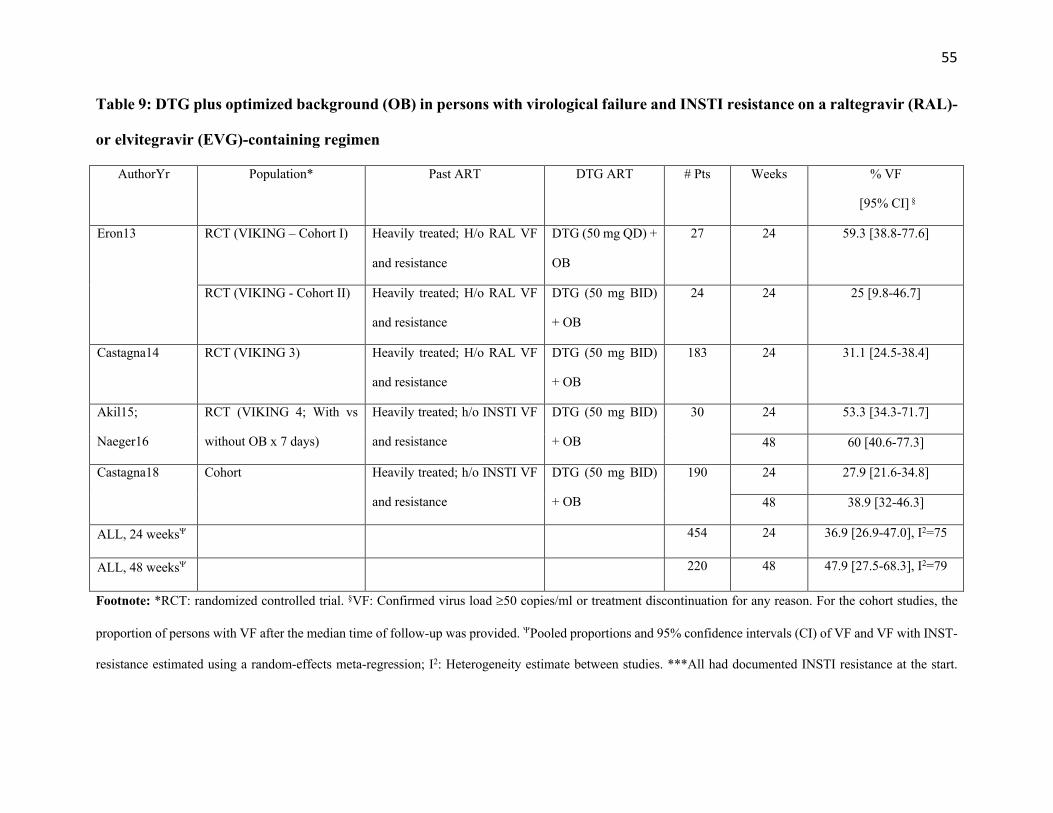
55
Table 9: DTG plus optimized background (OB) in persons with virological failure and INSTI resistance on a raltegravir (RAL)-
or elvitegravir (EVG)-containing regimen
AuthorYr
Population* Past ART DTG ART # Pts Weeks % VF
[95% CI] §
Eron13 RCT (VIKING – Cohort I) Heavily treated; H/o RAL VF
and resistance
DTG (50 mg QD) +
OB
27 24 59.3 [38.8-77.6]
RCT (VIKING - Cohort II)
Heavily treated; H/o RAL VF
and resistance
DTG (50 mg BID)
+ OB
24 24 25 [9.8-46.7]
Castagna14 RCT (VIKING 3) Heavily treated; H/o RAL VF
and resistance
DTG (50 mg BID)
+ OB
183 24 31.1 [24.5-38.4]
Akil15;
Naeger16
RCT (VIKING 4; With vs
without OB x 7 days)
Heavily treated; h/o INSTI VF
and resistance
DTG (50 mg BID)
+ OB
30 24 53.3 [34.3-71.7]
48 60 [40.6-77.3]
Castagna18 Cohort Heavily treated; h/o INSTI VF
and resistance
DTG (50 mg BID)
+ OB
190 24 27.9 [21.6-34.8]
48 38.9 [32-46.3]
ALL, 24 weeksY 454 24 36.9 [26.9-47.0], I2=75
ALL, 48 weeksY 220 48 47.9 [27.5-68.3], I2=79
Footnote: *RCT: randomized controlled trial. §VF: Confirmed virus load ³50 copies/ml or treatment discontinuation for any reason. For the cohort studies, the
proportion of persons with VF after the median time of follow-up was provided. YPooled proportions and 95% confidence intervals (CI) of VF and VF with INST-
resistance estimated using a random-effects meta-regression; I2: Heterogeneity estimate between studies. ***All had documented INSTI resistance at the start.
56
Most or possibly all developed one or more additional INSTI resistance mutation after DTG VF. 31% of the persons in Castagna18 had previously been enrolled
in one of the VIKING trials.

57
FIG. 1
Flow chart of study selection process. Of 742 studies identified through a PubMed search
performed January 2019 using the search string “Dolutegravir or GSK1349572”, 229 were read in
their entirety following an initial review of titles and abstracts. Following a full text review of these
229 studies and of 35 additional studies from meeting presentations, 95 studies met our inclusion
742 studies identified through PubMed search as of January 2019
229 studies after titles/abstracts reviews
264 studies for full reviews
35 additional studies from other sources
118 studies excluded:Reviews (40)Data for first-generations INSTIs (25)Mechanism studies (22) HIV-2 and non-group M (11)Duplicate studies (20)
146 studies assessed for eligibility
in vivo selection(26)
51 studies excluded:Virological outcome with standard first-line ART (24)Virological outcome in small numbers of persons or in
persons with heterogeneous past treatments and DTG-containing regimens (21)
Virological outcome during DTG intensification or stable treatment switch (6)
No baseline genotype prior to DTG in INSTI experienced persons (2)
Description of novel susceptibility methods (2)
95 studies included
clinical outcomes(38)
in vitro susceptibility(41)
in vitro selection(14)
Iden
tifica
tion
Scre
enin
gEl
igib
ility
Inclu
ded
58
criteria, containing data on mutations emerging under DTG selection pressure in vitro and in vivo;
in vitro DTG susceptibility; and the risk of virological failure and drug resistance in clinical trials
and cohorts.

59
FIG. 2
Box plots of in vitro DTG susceptibility results for 176 site-directed mutants and 105 clinical
isolates containing R263K, G118R, N155H, and/or Q148H/R/K. Purple plots indicate the fold
reduced susceptibility for viruses with R263K with or without G118R, N155H, and Q148H/R. Red
plots indicate the fold reduced susceptibility for viruses containing G118R. Yellow plots indicate
the fold reduced susceptibility for viruses containing N155H with or without Q148H/R. Blue plots
indicate the fold reduced susceptibility for viruses containing Q148H/R/K. In addition to the four
signature mutations, mutation patterns were characterized by the number of additional INSTI-
resistance mutations. The number of isolates with each pattern is shown in parentheses.
Q148K+2,3 (n=5)Q148R+2,3 (n=15)Q148H+2,3 (n=35)
Q148K+1 (n=10)Q148R+1 (n=27)Q148H+1 (n=41)
Q148K (n=7)Q148R (n=7)
Q148H (n=11)N155H,Q148R+2 (n=1)
N155H,Q148R (n=4)N155H,Q148H+2 (n=1)N155H,Q148H+1 (n=1)
N155H,Q148H (n=1)N155H+2,4 (n=7)N155H+1 (n=28)
N155H (n=21)G118R+2,3 (n=3)
G118R+1 (n=5)G118R (n=9)
R263K,Q148R+2 (n=2)R263K,Q148R+1 (n=1)R263K,N155H+1 (n=5)
R263K,N155H (n=1)R263K,G118R+2 (n=1)
R263K+2,3 (n=3)R263K+1 (n=13)
R263K (n=16)
Reduced Susceptibility
<=0.5 1 2 4 8 16 32 >=64