060117An Overview of the New Resuscitation Guidelines
3
UPDATE NT CLINICAL NT CLINICAL is an essential resource for extending your knowledge base. You can fulfil your continuing professional development PREP requirements by reflecting on the articles in this section. P25 UPDATE informs you of new developments in clinical practice P29 FACTS supplies key information on clinical topics. This week: leprosy P30 SYSTEMS OF LIFE presents educational information on anatomy and physiology. This week: the liver, part six – transplantation P34 KNOWLEDGE provides guided learning to help you with your CPD. This week: managing bite wounds P38 DEVELOPMENT highlights how nurses are developing practice. This week: smoking cessation services P41 DRUGS is a comprehensive summary of specific medicines. This week: goserelin P42 RESEARCH presents the latest nursing research papers. This week: patient restraint positions in psychiatric care NT 17 January 2006 Vol 102 No 3 www.nursingtimes.net An overview of the new resuscitation guidelines AUTHOR Phil Jevon, PGCE, BSc, RN, is resuscitation officer/clinical skills lead, Manor Hospital, Walsall. ABSTRACT Jevon, P. (2006) An overview of the new resuscitation guidelines. Nursing Times; 102: 3, 25–27. New resuscitation guidelines contain significant changes intended to improve resuscitation practice and survival from cardiac arrest. The guidelines also include helpful new sections with guidance on in-hospital resuscitation. This article provides an overview of the key changes and discusses their practice implications for nurses. The first international resuscitation guidelines were published in 2000. This followed global collaboration led by the International Liaison Committee on Resuscitation to improve the practice and teaching of resuscitation (Colquhoun and Nolan, 2005). The ILCOR 2005 formed the basis for the European Resuscitation Council guidelines (European Resuscitation Council, 2005). The Resuscitation Council (UK) has issued an abbreviated version of these guidelines (Resuscitation Council (UK), 2005a). The key changes Chain of survival The ‘Chain of Survival’ (Fig 1, p27), which describes the actions linking a patient who has a cardiac arrest with survival, has been revised to reflect the emphasis of the European guidelines (Nolan, 2005). Prevention of in-hospital cardiac arrest There is particular emphasis on the importance of prevention of in-hospital cardiac arrest. Most patients who suffer a cardiac arrest in hospital display adverse signs such as tachypnoea, tachycardia or hypotension prior to collapse. Unfortunately, ill patients at risk of cardiorespiratory arrest are rarely identified, and those that are, are often inappropriately managed (Kause et al, 2004). Confirmation of cardiorespiratory arrest Confirmation of cardiorespiratory arrest is not straightforward. Undertaking a carotid pulse check is an unreliable method of confirming the presence or absence of circulation (Bahr et al, 1997). In addition, there is no evidence that checking for movement, breathing or coughing, as previously recommended, is diagnostically superior. Agonal gasps and slow, laboured or noisy breathing are common at the onset of an arrest (Soar and Spearpoint, 2005) and can be mistaken for adequate breathing. To confirm cardiorespiratory arrest, look, listen, and feel for signs of breathing for up to 10 seconds to determine the absence of normal breathing. In addition, those experienced in clinical assessment may wish to check for the carotid pulse for up to 10 seconds either simultaneously or after checking for breathing to determine its absence (Soar and Spearpoint, 2005). Chest compressions The main focus of the new guidelines is on chest compressions, particularly on optimal performance and minimising interruptions. Chest compression technique is often poor with unnecessary and lengthy interruptions (Abella et al, 2005). After a break it takes several compressions to reach the prestoppage coronary perfusion pressure (Kern et al, 1998). The new guidelines recommend: l Using a ratio of 30 compressions to two ventilations. In most situations the initial two
-
Upload
christan-chaputtra -
Category
Documents
-
view
218 -
download
2
description
New resuscitation guidelines contain significantchanges intended to improve resuscitation practiceand survival from cardiac arrest. The guidelinesalso include helpful new sections with guidance onin-hospital resuscitation. This article provides anoverview of the key changes and discusses theirpractice implications for nurses
Transcript of 060117An Overview of the New Resuscitation Guidelines

update
NtCliniCalNT CliNiCal is an essential resource for extending your knowledge base. You can fulfil your continuing
professional development PREP requirements by reflecting on the articles in this section.
P25 UPDaTE informs you of new developments in clinical practice
P29faCTs supplies key information on clinical topics. This week: leprosy
P30 sYsTEMs Of lifE presents educational information on anatomy and physiology. This week: the liver, part six – transplantation
P34KnOwlEDgE provides guided learning to help you with your CPD. This week: managing bite wounds
P38DEvElOPMEnT highlights how nurses are developing practice. This week: smoking cessation services
P41 DRUgs is a comprehensive summary of specific medicines. This week: goserelin
P42REsEaRCh presents the latest nursing research papers. This week: patient restraint positions in psychiatric care
NT 17 January 2006 Vol 102 No 3 www.nursingtimes.net
An overview of the new resuscitation guidelinesauthor phil Jevon, pGCe, BSc, RN, is resuscitation officer/clinical skills lead, Manor hospital, walsall.abstract Jevon, p. (2006) an overview of the new resuscitation guidelines. Nursing Times; 102: 3, 25–27. new resuscitation guidelines contain significant changes intended to improve resuscitation practice and survival from cardiac arrest. The guidelines also include helpful new sections with guidance on in-hospital resuscitation. This article provides an overview of the key changes and discusses their practice implications for nurses.
The first international resuscitation guidelines were published in 2000. This followed global collaboration led by the International Liaison Committee on Resuscitation to improve the practice and teaching of resuscitation (Colquhoun and Nolan, 2005). The ILCOR 2005 formed the basis for the European Resuscitation Council guidelines (European Resuscitation Council, 2005). The Resuscitation Council (UK) has issued an abbreviated version of these guidelines (Resuscitation Council (UK), 2005a).
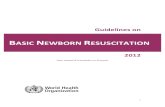
The key changesChain of survivalThe ‘Chain of Survival’ (Fig 1, p27), which describes the actions linking a patient who has a cardiac arrest with survival, has been revised to reflect the emphasis of the European guidelines (Nolan, 2005).
Prevention of in-hospital cardiac arrestThere is particular emphasis on the importance of prevention of in-hospital cardiac arrest. Most patients who suffer a cardiac arrest in hospital display adverse signs such as tachypnoea,
tachycardia or hypotension prior to collapse. Unfortunately, ill patients at risk of cardiorespiratory arrest are rarely identified, and those that are, are often inappropriately managed (Kause et al, 2004).
Confirmation of cardiorespiratory arrestConfirmation of cardiorespiratory arrest is not straightforward. Undertaking a carotid pulse check is an unreliable method of confirming the presence or absence of circulation (Bahr et al, 1997). In addition, there is no evidence that checking for movement, breathing or coughing, as previously recommended, is diagnostically superior. Agonal gasps and slow, laboured or noisy breathing are common at the onset of an arrest (Soar and Spearpoint, 2005) and can be mistaken for adequate breathing.
To confirm cardiorespiratory arrest, look, listen, and feel for signs of breathing for up to 10 seconds to determine the absence of normal breathing. In addition, those experienced in clinical assessment may wish to check for the carotid pulse for up to 10 seconds either simultaneously or after checking for breathing to determine its absence (Soar and Spearpoint, 2005).
Chest compressionsThe main focus of the new guidelines is on chest compressions, particularly on optimal performance and minimising interruptions. Chest compression technique is often poor with unnecessary and lengthy interruptions (Abella et al, 2005). After a break it takes several compressions to reach the prestoppage coronary perfusion pressure (Kern et al, 1998). The new guidelines recommend:l Using a ratio of 30 compressions to two ventilations. In most situations the initial two

update
RefeRenCes
abella, B. et al (2005) Chest compression rates during
cardiopulmonary resuscitation are suboptimal: a prospective study during inhospital cardiac arrest.
Circulation; 111: 428–434.
Bahr, J. et al (1997) Skills of lay people in checking the carotid pulse.
Resuscitation; 35: 23–26.
Bingham, R. et al (2005) Paediatric Basic life Support in Resuscitation
Guidelines 2005. Resuscitation Council UK: London.
Chamberlain, D. (2005) New international consensus
on cardiopulmonary resuscitation. British Medical Journal;
331: 1281–1282.
Colquhoun, M., nolan, J. (2005) Introduction in Resuscitation
Guidelines 2005. London: Resuscitation Council UK.
Davies, s. (2005) The Use of Automated External Defibrillators in Resuscitation Guidelines 2005. London: Resuscitation Council UK.
Deakin, C. et al (2005) Adult Advanced Life Support in
Resuscitation Guidelines 2005. London: Resuscitation Council UK.
European Resuscitation Council (2005) European Resuscitation
Council guidelines for resuscitation. Resuscitation; 67:
(Suppl 1), S1–S190.
handley, a. (2005) Adult Basic Life Support in Resuscitation
Guidelines 2005. London: Resuscitation Council UK.
26 NT 17 January 2006 Vol 102 No 3 www.nursingtimes.net
This article has been double-blind peer-reviewed.
for related articles on this subject and links to relevant websites see
www.nursingtimes.net
ventilations are omitted (except in the situations discussed below) to allow more time for chest compressions; l Locate the correct position for compressions by placing one hand in the centre of the chest and the other on top, rather than wasting time using the ‘rib margin’ location method. Avoid applying pressure over the end of the sternum and the upper abdomen; l To prevent fatigue, rotate the person performing compressions approximately every two minutes;l Following defibrillation, start chest compressions immediately, without checking for a pulse (Deakin et al, 2005).
VentilationsWhen performing ventilations an inspiratory time of one second should be sufficient to achieve chest rise similar to normal breathing (Soar and Spearpoint, 2005) and minimise interruptions to chest compressions. The initial two ventilations are no longer recommended except in a minority of situations, such as near drowning. Otherwise, CPR should begin with chest compressions.
Most practitioners are unwilling to undertake mouth-to-mouth resuscitation for a variety of reasons, including perceived risk of infection and distaste of the procedure (Handley, 2005). If there is a clinical reason to avoid mouth-to-mouth ventilation, such as a perceived risk of infection, or if the rescuer is unable or unwilling to perform it, provide chest compressions only until further help and equipment arrive. Appropriate resuscitation equipment should always be immediately available in the hospital setting.
DefibrillationIn-hospital defibrillation should be performed as soon as possible – within three minutes of arrest (Soar and Spearpoint, 2005).
The three-shock sequence for a resistant shockable rhythm is no longer recommended. After the first shock, compressions and ventilations (30:2) should be performed for two minutes before undertaking a pulse/ECG rhythm check, to minimise the ‘no-bloodflow’ time. Further shocks are only delivered after additional two-minute periods of CPR (Chamberlain, 2005).
The recommended initial energy level when using a biphasic defibrillator is 150–200J, with second and subsequent shocks at 150–360J (if using a monophasic defibrillator the initial and subsequent shocks should be 360J) (Deakin et al, 2005).
Defibrillation is no longer recommended if there is uncertainly over whether the ECG trace is asystole or fine ventricular fibrillation (VF) because it is unlikely to result in a perfusing rhythm: continue with CPR (Soar and Spearpoint, 2005).
The use of an automated external defibrillator (AED) should be considered by nurses to be part of their role (Davies, 2005).
epinephrine (adrenaline)In ventricular fibrillation/ventricular tachycardia, epinephrine (adrenaline) is only administered if the rhythm persists after the second shock. In asystole and pulseless electrical activity, it should be administered as soon as IV access is achieved (Deakin et al, 2005). It is then repeated every 3–5 minutes.
Treatment algorithmsThe adult and paediatric basic and advanced algorithms have been updated to reflect changes in the 2005 guidelines. Every effort has been made to keep the algorithms simple, yet make them applicable to cardiac arrest victims in most circumstances (Colquhoun and Nolan, 2005).
Post-resuscitation careInterventions in the post-resuscitation period can significantly influence the final outcome (Deakin et al, 2005). In particular, therapeutic hypothermia (cooled to 32–34°C) is now indicated in unconscious adult patients with a spontaneous circulation following an out-of-hospital VF arrest (Deakin et al, 2005). In addition, mild hypothermia may benefit unconscious adult patients with a spontaneous circulation following an out-of-hospital cardiac arrest due to a non-VF arrest or following an in-hospital arrest (Deakin et al, 2005). Hyperthermia should be treated.
Paediatric resuscitationThere have been a number of changes to the way paediatric resuscitation is performed, partly as a result of new scientific evidence and partly to simplify teaching and retention (Bingham et al, 2005). The main changes are as follows:l Age definition for a child: from one year to puberty;l Start resuscitation with five ventilations – priority is oxygenation;l The ratio for compressions to ventilations is 15:2 (30:2 for a lone or layperson rescuer);l Chest compressions in children – use one or two-handed technique according to preference;l Treatment for foreign body airway obstruction has been simplified depending on whether the child is conscious or unconscious;l Ideally administer medications via the IV or intraosseous (IO), rather than the tracheal, route;l Cuffed or uncuffed tracheal tubes can be used in the hospital setting;l As in adults, the three-shock sequence for a resistant shockable rhythm is no longer

RefeRenCes
international liaison Committee on Resuscitation (2005) International Consensus on Cardiopulmonary Resuscitation. www.erc.edu/index.php/ilcor/en
Kause, J. et al (2004) A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom: the ACADEMIA study. Resuscitation; 62: 275–282.
Kern, K. et al (1998) Efficacy of chest compression-only BLS CPR in the presence of an occluded airway. Resuscitation; 39: 179–188. nolan, J. (2005) European Resuscitation Council Guidelines for Resuscitation 2005 section 1. Introduction. Resuscitation; 67S1: S3–S6.
nolan, J. et al (2005) European Resuscitation Council Guidelines for Resuscitation 2005 Section 4. Adult advanced life support. Resuscitation; 67S1, S39–S86.
Resuscitation Council (UK) (2005a) Resuscitation Guidelines 2005. London: Resuscitation Council UK.
Resuscitation Council (UK) (2005b) Statement on the Use of AEDs (Interim Period until AED has been Re-programmed). www.resus.org.uk
Richmond, s. (2005) Newborn Life Support in Resuscitation Guidelines 2005. London: Resuscitation Council UK.
soar, J., spearpoint, K. (2005) In-hospital resuscitation. In: RCUK. Resuscitation Guidelines. London: RCUK.
keywoRdS n Resuscitation n Cardiac arrest n Guidelines
27NT 17 January 2006 Vol 102 No 3 www.nursingtimes.net
FiG 1. the ChaiN oF SuRvival (adapted FRom NolaN et al, 2005)
This article has been double-blind peer-reviewed.
for related articles on this subject and links to relevant websites see www.nursingtimes.net
recommended; after the first shock, compressions and ventilations (15:2) should be performed for two minutes (see above);l If using a manual defibrillator, the shock energy for children is 4J/kg for all shocks;l A standard AED can be used in children over eight years of age; for younger children, ideally use a paediatric system such as paediatric pads, as these automatically select an appropriate energy level. However, if the only defibrillator available is an AED, use this;l The standard dose for adrenaline (epinephrine) in cardiac arrest is 10mcg/kg – higher doses are no longer routinely recommended (Bingham et al, 2005).
newborn resuscitationThe main changes for newborn resuscitation are as follows:l A food-grade plastic wrapper can be applied to significantly premature babies to maintain body temperature;l The aspiration of meconium from the nose and mouth of the unborn baby, while the head is still on the perineum, is no longer advocated;l If indicated, ventilations can be started with air; however, additional oxygen should be available if the baby does not rapidly improve;l Adrenaline (epinephrine) should be administered intravenously or via the intraosseous route because standard doses are unlikely to be effective if the tracheal tube route is used;l If there are no signs of life after 10 minutes of continuous and adequate resuscitation, it may be justified to discontinue resuscitation (Richmond, 2005).
Implementing the new guidelinesThere are a number of major changes in the new guidelines and this will result in delays in their implementation. At a local level, this process of
change will ideally be overseen by the trust’s resuscitation committee. Nationally, the Resuscitation Council (UK)’s courses are in the process of being revised and updated, with new teaching materials being developed, which will be ready during 2006.
During the transition period, the Resuscitation Council (UK) has acknowledged that there will undoubtedly be some variation in resuscitation practice between individuals and between health care organisations.
It must be stressed that the publication of the guidelines does not imply that current clinical care is either unsafe or ineffective (Colquhoun and Nolan, 2005). While awaiting the local implementation of the new guidelines, continue with current practice, as it would be unhelpful at a resuscitation attempt if conflicting guidelines were being followed. For further advice contact a local resuscitation officer.
Implications for nursesFollowing the publication of the new resuscitation guidelines, nurses must ensure their skills and knowledge are updated and that they are competent to carry out resuscitation at a level appropriate for their clinical role.
All nurses should at least be proficient in basic life support with the use of airway adjuncts and basic ventilatory devices as appropriate. They should also consider the use of an AED to be part of their role (Davies, 2005).
Nurses should liaise with their resuscitation officer who can advise on the date for ‘going live’ with the new resuscitation guidelines. AEDs will need to be reprogrammed in line with the new guidelines, for example to ensure voice prompts and energy levels are appropriate (RCUK, 2005b). The full guidelines are available from the www.resus.org.uk website. n
early recognition and call for help to prevent cardiac arrest
early CpR to buy time early defibrillation to restart the heart
post-resuscitation care to restore quality of life