
020 uterine torsion - Sher-e-Bangla Agricultural University
18
1. Carpal flexion Dystocia due to postural defects and management Professor Nasrin Sultana Juyena, PhD
Transcript of 020 uterine torsion - Sher-e-Bangla Agricultural University

1.Carpal flexion
Dystocia due to postural defects and managementProfessor Nasrin Sultana Juyena, PhD

1.Carpal flexion
Correction:
Retropulsion of the foetal head or shoulder
Push the retained carpal upward (Fig.1a Grasp the digits in the cupped hand and pull it into the pelvic cavity alongside
the other limb (Fig 1b). With little traction the foetus can be delivered.
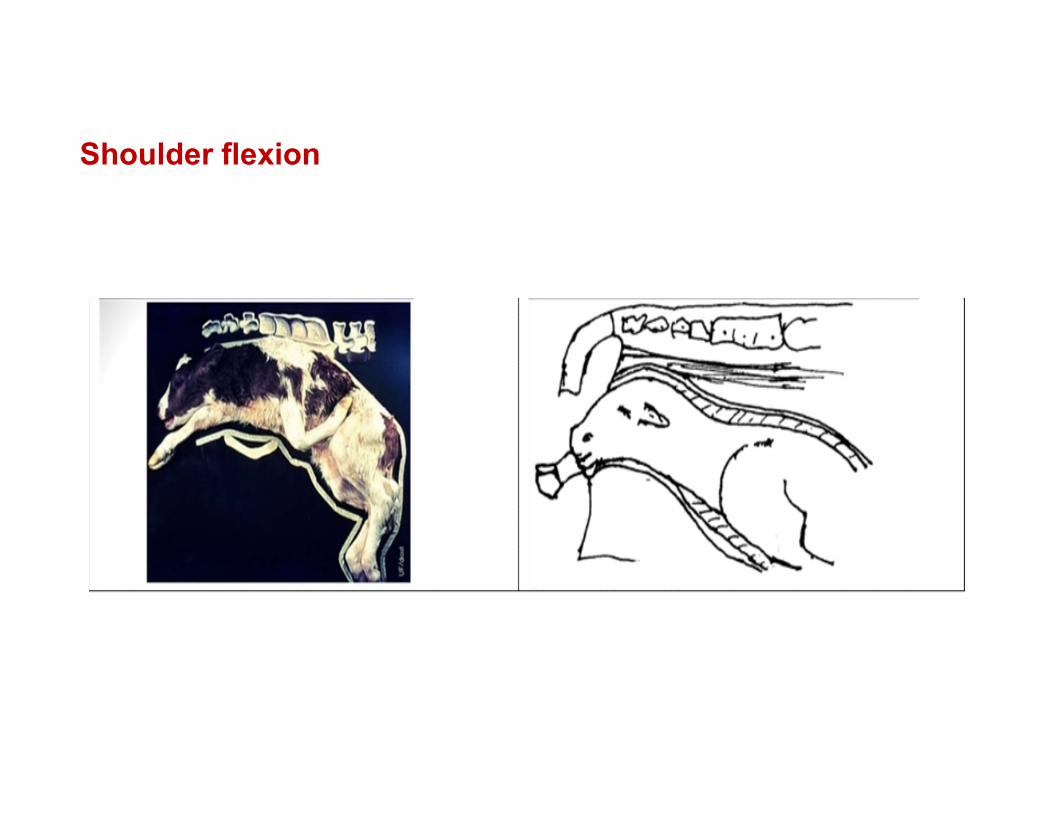
Shoulder flexion

Shoulder flexion
Apply a snare at the mandible and repulse the foetal head into the pelvic cavity.
Locate the flexed limb and make it into carpal flexion by holding below the shoulder joint and pulling it upward (Fig.2a & b).
After this, correction is similar to that of carpal flexion
Correction

Lateral deviation of head

Lateral deviation of head
Correction
Apply snares at the presented limbs andapply retropulsion at the base of the neck.
Locate the head and apply a snare at themandible (Figure 3 a&b).
Ask the assistant to apply traction at thesnare applied to the mandible until thehead comes to the normal posture.
Apply synchronized traction with theabdominal contraction of the dam until thefoetus is delivered.

Downward displacement of head
Correction Apply snare at the limbs Push the foetal head back into the abdominal cavity. Locate the muzzle of the foetus, grasp by mandible and pull itinto
the pelvic cavity. Apply traction to deliver the foetus.

Foot–nape presentation
Correction
The uppermost limb is recognized, and as the foal’s muzzle is vigorously repelled in a cranial and upward direction. the fetal foot is raised and then pushed, or pulled, to the appropriate side.
The other foot is similarly manipulated and, finally, the head is again raised and each foreleg placed underneath it.
Traction is then applied to the head and both forelimbs.

Hip flexion posture/‘breech presentation’

Hip flexion posture/‘breech presentation’
Correction
The manipulative procedure is to repel the calf’s perineum forwards andupwards with a view to bringing the retained limbs within reach, when the legmay be grasped as near to the hock as possible.
Traction on the limb converts the posture into hock flexion, from which pointthe previously described procedure is carried out.
If it is impossible to bring the hock within reach, and the calf is dead, thenfetotomy may be performed.

The best method for removing the retained hind limb is to use the wire-sawfetotome.o One tube of the instrument is threaded, and the free end of the wire, attached
to an introducer, is passed from above to below around the proximal part of themore accessible limb.
o The introducer is sought from below and brought out and the other tube of thefetotome is threaded. The fetotome is passed along the vagina, and the head ofthe instrument placed against the fetal perineum.
o At this stage, a most important step in the procedure is to include the fetal tail inthe loop of wire and to hold the head of the instrument firmly to the perineumwhile sawing takes place.
o In this way the femur is sectioned through its articular head. The detached limbis removed. The other hindlimb is similarly removed.

An alternative procedure, after the amputation of one limb, is to apply traction – through the medium of an anal hook which is passed into the fetal anus and over the fetal pelvic brim and to attempt to deliver the calf without extending the other hind limb.
If, after a proper effort, attempts to extend the hind limbs are unsuccessful and the foal is still alive, a caesarean operation is recommended
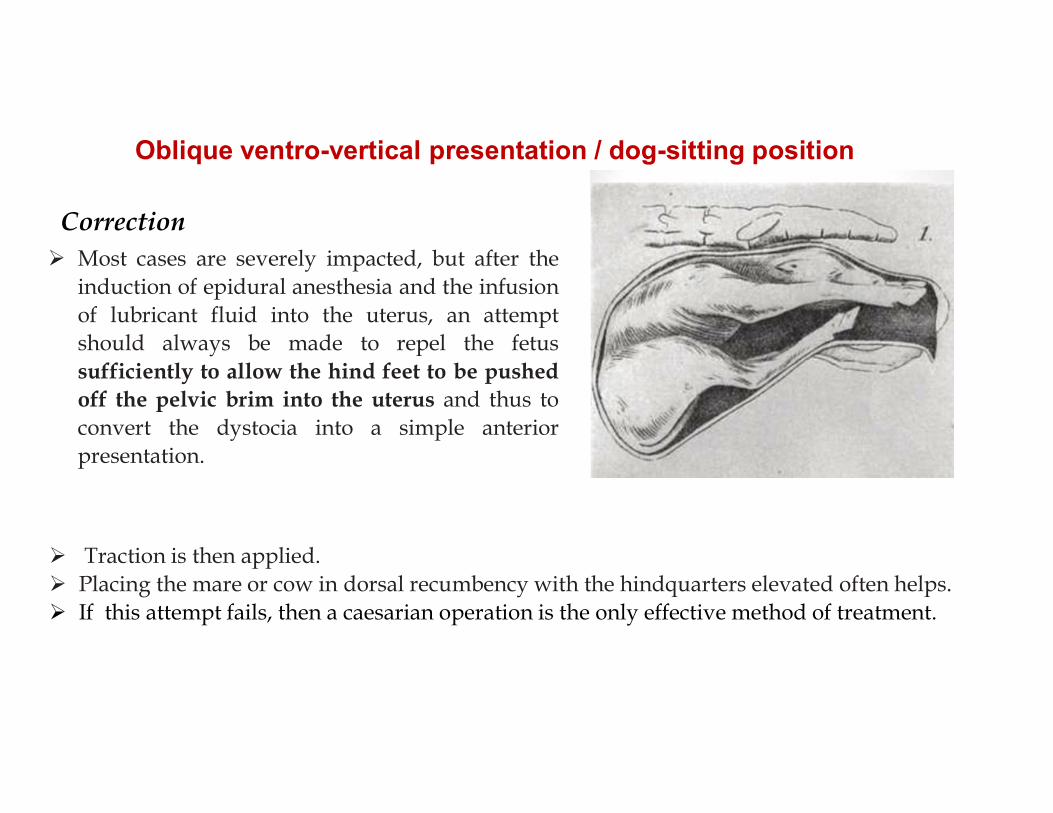
Oblique ventro-vertical presentation / dog-sitting position
Traction is then applied. Placing the mare or cow in dorsal recumbency with the hindquarters elevated often helps. If this attempt fails, then a caesarian operation is the only effective method of treatment.
Most cases are severely impacted, but after theinduction of epidural anesthesia and the infusionof lubricant fluid into the uterus, an attemptshould always be made to repel the fetussufficiently to allow the hind feet to be pushedoff the pelvic brim into the uterus and thus toconvert the dystocia into a simple anteriorpresentation.
Correction

Ventro-transverse presentation
Correction
The aim of vaginal interference is firstly to convert the abnormality into longitudinal– usuallyposterior – presentation, ventral position; this means that the posterior extremity must be advancedwhile the anterior extremity is repelled.
General anaesthesia and dorsal recumbency are helpful in the mare. If version fail, the caesarean operation is recommended for both mare and cow.
In the bicornual type of transverse presentation peculiar to mares the fetal extremities are disposed inthe two horns and its trunk lies across the anterior portion of the uterine body.
Ventral displacement of the uterus may have occurred, and, if so, it may be impossible to palpate thefetus. As soon as the presentation is recognized a caesarean operation should be performed.

Dorso-transverse presentation
Correction
The technique of correction required involves repulsion of the fetus, and the advancement of itsnearer extremity to the birth canal.
The cow should be given an epidural anaesthetic, and in the mare general anaesthesia should beinduced, so that she can be placed on her back (dorsal recumbence).
Fetal fluid supplement is then instilled and an attempt made by manipulation of the proximalfetal extremity to turn the fetus into ventral position, anterior or posterior presentation.
The next step is to rotate the fetus into dorsal position. Finally, fetus is delivered by traction.If version cannot be achieved, a caesarean operation should be performed immediately. Fetotomy is very difficult to carry out in this type of dystocia and consequently is not recommended.

Lack of tone or failure of the uterine muscle to contract. Most commonly seen in Dogs & Cow especially in older dairy cows.
Causes- Diseases of uterine muscle Due to lack or failure of release of hormones. Lace of exercise Excessive fatness Debility and senility causes weakness of uterine contraction at parturition.
Treatment:-i. 10% ii. Ca borogluconate :0.5-1.5 ml/kg bwiii. Inj. Oxytocine/Pitutrin- Large Animal 20-100 units, Small animal- 10-20 units.Inj. should be
given with saline by an IV drip. iv. Feathering-(Dog) - Feathering the vagina by inserting finger and stroking the dorsal wall of the
vagina to stimulate the production of oxytocine by animal.
If no respond after 3-5 hours Caesarean Section recommended.
Primary Uterine inertia
Prolonged by dystocia & it is characterized by exhaustation of uterine muscles.Cattle- Retracting/ contracting ring dystocia:- Where the uterine muscle just cranial to the cervix contract tightly, so normal
expulsion of the fetus in to birth canal do not take place. - In this condition by per vaginal palpation revealed normal PPP-Presentation,
Position, Posture but uterine muscle contract over fetus.
Treatment:- Lubrication of birth canal, and removal the fetus by traction if normal
PPP. Injection of Ca borogluconate Injection of oxytocine Caesarean indicated is recommended if fetus is large and live.
Secondary inertia

1. Ca borogluconate SC/IV and wait 1-2 hrs.2. Application of misoprostol
Technique: The perineum and adjacent areas were washed with soap and water and
disinfected with lugol’s iodine. Obstetrical hands covered with long plastic gloves and lubricated with
obstetrical lubricant need to inserted in the birth canal, then 1 mg (5 tablets)of misoprostol (synthetic PGE1) (Cytotec, Searle Pharmaceuticals Ltd, UK)can be inserted in the partially dilated cervical canal.
Every 10 minutes the cervical canal should be examined. After 45 minutes the cervix can be completely dilated and the fetal parts
can easily be examined.
Incomplete dilatation of cervix
Called Ringwomb, very common problem for ruminants


















