
015-ECG 1/13/04 11:31 AM Page 15 ECG
2
Perspectives in Cardiology / January 2004 15 University of Ottawa Heart Institute ECG of the Month By Martin S. Green, MD, FRCPC Too Fast or Too Slow? This is the ECG of an 85-year-old woman, with a history of syncope, who frequently passes out. What is the diagnosis? 015-ECG 1/13/04 11:31 AM Page 15
Transcript of 015-ECG 1/13/04 11:31 AM Page 15 ECG

Perspectives in Cardiology / January 2004 15
University of Ottawa Heart Institute
ECGof the Month
By Martin S. Green, MD, FRCPC
Too Fast or Too Slow?This is the ECG of an 85-year-old woman, with a history of syncope, who frequentlypasses out.
What is the diagnosis?
015-ECG 1/13/04 11:31 AM Page 15
Perspectives in Cardiology / January 200416
The ECG shows a regular, narrow complex ventric-ular rhythm, approximating 25 beats per minute(bpm). The morphology is consistent with an incom-plete right bundle branch block (RBBB).Superimposed upon this regular ventricular activityare P waves in a regular sinus rhythm approximating75 bpm. There appears to be no association betweenthe atria and ventricle rhythm. This electrocardio-graphic picture is consistent withcomplete heart block. This diag-nosis is made based on the disso-ciation of atrioventricular activi-ty, and with a regular ventricularescape (usually less than 40bpm). If the ventricular rhythm isnot regular in the presence ofmultiple atrial stimuli, one maysuppose that a high level of sec-ond-degree block exists, ratherthan complete heart block.
Provided the patient has anadequate ventricular escape, this rhythm is normallywell-tolerated in elderly patients. The prolongeddiastolic filling results in supra-normal preload and,consequently, large stroke volumes. Indeed, thiswoman’s blood pressure was 180/70 mmHg whenthe 12-lead ECG was obtained. So, why is thispatient passing out?
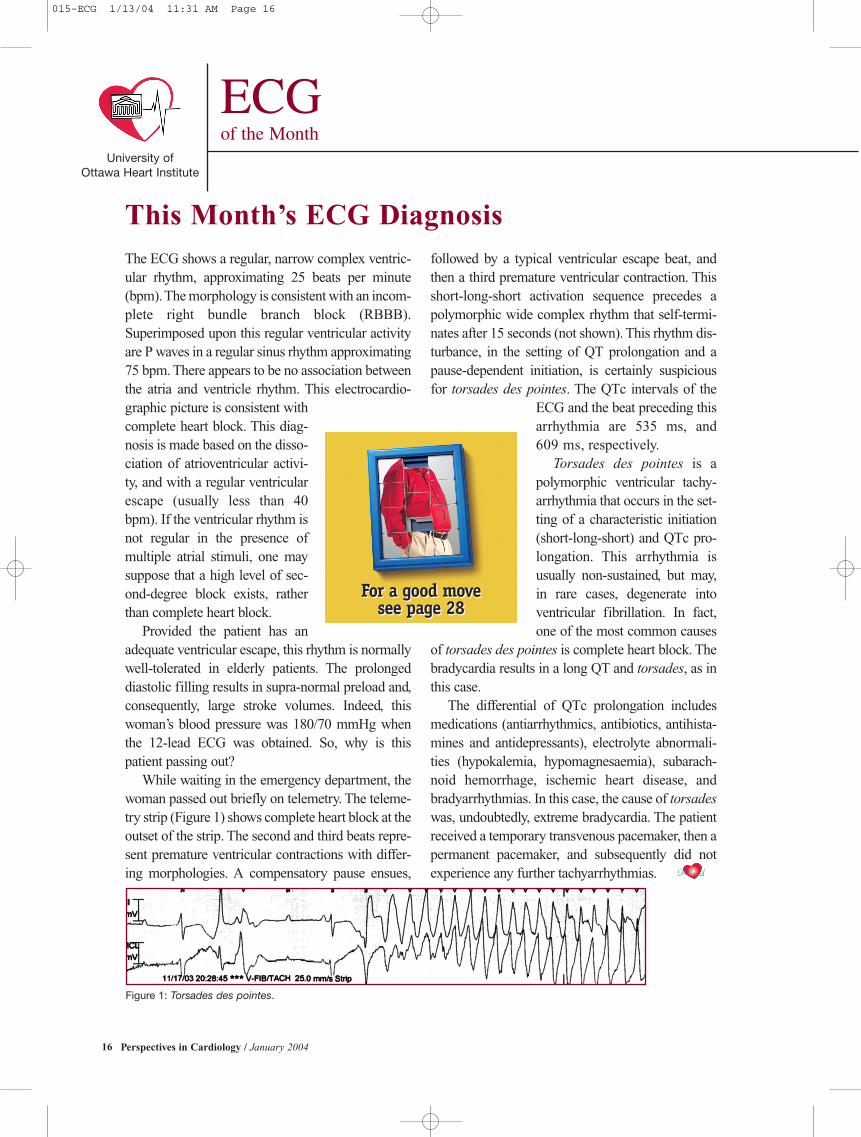
While waiting in the emergency department, thewoman passed out briefly on telemetry. The teleme-try strip (Figure 1) shows complete heart block at theoutset of the strip. The second and third beats repre-sent premature ventricular contractions with differ-ing morphologies. A compensatory pause ensues,
followed by a typical ventricular escape beat, andthen a third premature ventricular contraction. Thisshort-long-short activation sequence precedes apolymorphic wide complex rhythm that self-termi-nates after 15 seconds (not shown). This rhythm dis-turbance, in the setting of QT prolongation and apause-dependent initiation, is certainly suspiciousfor torsades des pointes. The QTc intervals of the
ECG and the beat preceding thisarrhythmia are 535 ms, and609 ms, respectively.
Torsades des pointes is apolymorphic ventricular tachy-arrhythmia that occurs in the set-ting of a characteristic initiation(short-long-short) and QTc pro-longation. This arrhythmia isusually non-sustained, but may,in rare cases, degenerate intoventricular fibrillation. In fact,one of the most common causes
of torsades des pointes is complete heart block. Thebradycardia results in a long QT and torsades, as inthis case.
The differential of QTc prolongation includesmedications (antiarrhythmics, antibiotics, antihista-mines and antidepressants), electrolyte abnormali-ties (hypokalemia, hypomagnesaemia), subarach-noid hemorrhage, ischemic heart disease, andbradyarrhythmias. In this case, the cause of torsadeswas, undoubtedly, extreme bradycardia. The patientreceived a temporary transvenous pacemaker, then apermanent pacemaker, and subsequently did notexperience any further tachyarrhythmias.
University of Ottawa Heart Institute
ECGof the Month
This Month’s ECG Diagnosis
Figure 1: Torsades des pointes.
For a good move see page 28
For a good move see page 28
PCard
015-ECG 1/13/04 11:31 AM Page 16

















![[XLS]tax.vermont.govtax.vermont.gov/sites/tax/files/documents/SPAN Data List... · Web view015-005-10947 015-005-10091 015-005-11649 015-005-10773 015-005-11222 015-005-10889 015-005-11109](https://static.fdocuments.in/doc/165x107/5ac161e67f8b9a5a4e8d129a/xlstax-data-listweb-view015-005-10947-015-005-10091-015-005-11649-015-005-10773.jpg)
