
01%$2*)%' 3%).'45676'' - oncoconferences.ch · – Does not kill tumor cells directly, but rather,...
62
!"#$%& ()**%")+, !"#$%$&$'()" +&,-.-/$" 0 123-4 52&("4 6778&-.-/9:;<! =&$>"4'$?@?''A$?2. <2'". #BC+ D84' C?E F2.."& 0 GHEIEIJGK -..+/01%$2*)% 3%). 45676
-
Upload
doannguyet -
Category
Documents
-
view
217 -
download
0
Transcript of 01%$2*)%' 3%).'45676'' - oncoconferences.ch · – Does not kill tumor cells directly, but rather,...

!"#$%&'()**%")+,'!"#$%$&$'()"*+&,-.-/$"*0*123-4*52&("4*6778&-.-/9:;<!*
=&$>"4'$?@?''A$?2.*<2'".*
#BC+*D84'*C?E*F2.."&*0*GHEIEIJGK*
-..+/01%$2*)%'3%).'45676''

• 63yearoldwhitefemale• ECOGPS0• Adenocarcinoma,noEGFR,BRAF,HER2,KRAS,NRAS,ALKalteraVon;T4N3M1b(mediasVnallymphnodes,boneandretroperitonealmets)diagnosedinJanuary2013.
• 4linesofsystemictherapy(carbo/pemetrexed&maintenance,taxotere,gemzar/vinorelbine)anderloVnib.
• Pulmonary,adrenal,boneandnodalprogressioninApril2014
Casepresenta8on

April2014 August2014
PD-1directedtherapy

Pulmonary,adrenalandboneprogressioninApril2015=1yearaGerbeginning
June2015:onsetofboneradiotherapyandongoingimmunotherapyNewbrainlesions,pulmonaryembolism.Death08/15
StablediseasefromAugust2014,working,PS0-1

O1%',+BB%,,'9#')..+/901%$2*C'

O1%'$%/2),,2/B%'9#')..+/901%$2*C'

5)"&^!"..72&Q*6778&$?9*IJGL*
-//9P28P%')..+/901%$2*)%,''!""#$%&'()%("*'$++,%$-.'(./"'-,*%$%&')%0'1,21"3,"%-/.'$%(*")1$%&'*"1#4%1"'*)-"1'
•! QA6O7!='•! QARS=;'•! QA6@:T'•! QA6@<UT'•! QAV-OW'•! -7A:'•! -7A<:'
•! X2BB)/%,'•! QA6@=;'
•! QA?@<MA?@A7<'•! QA7!VU'•! QAO-V-O'•! QAY-W'
•! QARS=;'•! QAZO7!'•! QA65[<W'•! -@R')/1)3)09$,''
•! QAX\V['•! \/&901%")/'$%B%*09$'•! 7[!<M-6!]<'•! 5%"%B8/,'
•! 6S67^'•! 6S67<;'•! 667E'

!24V&(-4"&2*"?*2.Q*C($"&("*IJG_*
5*%B0$+.'9#',9.28B'.+0289/,')/'B2/B%$'>%/9.%,'_'$%"28P%'B9/0$)3+89/'9#'.+0289/2"'*$9B%,,%,'
516+)-"'47'-8"'%"4)%6&"%'*"#"*-4$*"'$%'8,+)%'()%("*'
[9$.289/'9#'4%92/8>%/,'
''''''''
#$%`+%/0"C'
$%>+"2$"C'
9BB2,)9/2""C'

7+/>'62/B%$'-..+/901%$2*C'A'7!4@56!?\'
52&("4*6778&-?)"42A9`*2&9*$&?"42(V-&*M$?)*?)"*$778&"*'9'?"7*?-*?4"2?*(2&("4*
P(V>"`*A4$7$&/*-N*?)"*6778&"*'9'?"7*
P&V/"&a*'A"($b(*
U-&a2&V/"&a*'A"($b(*
ac*PFa'A"($b(*2&V3-#$"'*^*
(9?-?-]$(*X*("..'*
ac*"&)2&("7"&?*-N*$778&"*'9'?"7*
•! 59?-,$&"'*•! 5)"(,A-$&?*
$&)$3$?-4'*
52&("4**d2(($&2V-&*X)"42A9*
52&("4**6778&-7-#8.2V-&*
X)"42A9*
P&V/"&a*
O2''$>"`*#".$>"49*-N*(-7A-8&#'*?)2?*729*8'"*?)"*$778&"*'9'?"7*
!-&-(.-&2.*P&V3-#$"'*
P#-AV>"*5"..*X42&'N"4*
•! 5"?8]$723*•! ?42'?8%8723*
•! X5S*"&/$&""4$&/*
•! 5PS'*•! ;"$V(*("..'*
X24/"?"#*P&V3-#$"'*
6778&-?)"42A9*
5"..8.24**6778&-?)"42A9*
!-&-(.-&2.*

O1%'&),2**9)/0.%/0'9#'2B8P%')..+/901%$2*C'
)/'45676'5%a/>' ?12,%'---'
\2$"C'502>%''?9,0'5+$>%$C'
]!V\A!U'"#$%&'!()*+,(!--./!4"A-4?"#*BC!+*IJGY*
79BK'!&PK'502>%''?9,0'B1%.9$2&'
O%B%.98&%'b7AZ7?:Ec'0'#%'!()*+,(!12//!4"A-4?"#*PC5+*IJGL*
''''!&P2/B%&'''-/'B9.39'J)01'B1%.9'
Z%"2>%/*+.20+B%"A7'0'34!()*+,(!.//!4"A-4?"#*BC!+*IJGL*
$\V['X24/"?*GJJJ*4"(48$?"#*
OV=;<;''&"5!()*+,(!1///!6&?"4$7*BC!+*IJGY*ac*(-&V&82V-&*
W2B90+.9.23'b<\<;[*')*+,(!1/6-!-&/-$&/*
4'dLD;;;'
2#2A?"#*N4-7*d2&'?""&,$'?"Q*IJG_*

-..+/%'&C,#+/B89/')/1)3)8/>'P2BB)/%'%eB2BC''2/&'*90%/82"'0$%20.%/,'9*89/,'
•! X2BB)/%A,*%B)fB'O'B%""'),'%g12+,0%&'
•! ()"(,A-$&?*$&)$3$V-&*
•! 5-aCV78.2V-&*•! (9?-,$&"'*
•! !?6,'2$%'/90'9*8.2""C')..+/9>%/)B'
•! U->".*2#e8>2&?'*•! 5)"7-?)"42A9*•! 42#$2V-&*
•! 79B2"')..+/9A,+**$%,,)9/')/'01%'0+.9$'.)B$9AP%/)$9/.%/0'
•! 5)"(,A-$&?*$&)$3$V-&*
•! 6&)$3$V-&*-N*$778&-'AAA4"''$-&*"E/E*61aGJQ*X4"/'Q*6;+*
•! 72BN'9#'19.)/>' •! P&V2&/$-/"&$('*•! S2#$2V-&*•! ()"7-?)"42A9*
•! O9"%$2/B%'09'P2BB)/%'2/8>%/,'
•! &"-2&V/"&'*
S$%>$*"?*2.Q*C($"&("*IJG_*

7+/>'62/B%$'-..+/901%$2*C'A'7!4@56!?\'
52&("4*6778&-?)"42A9`*2&9*$&?"42(V-&*M$?)*?)"*$778&"*'9'?"7*?-*?4"2?*(2&("4*
P(V>"`*A4$7$&/*-N*?)"*6778&"*'9'?"7*
P&V/"&a*'A"($b(*
U-&a2&V/"&a*'A"($b(*
ac*PFa'A"($b(*2&V3-#$"'*^*
(9?-?-]$(*X*("..'*
ac*"&)2&("7"&?*-N*$778&"*'9'?"7*
•! 59?-,$&"'*•! 5)"(,A-$&?*
$&)$3$?-4'*
52&("4**d2(($&2V-&*X)"42A9*
52&("4**6778&-7-#8.2V-&*
X)"42A9*
O2''$>"`*#".$>"49*-N*(-7A-8&#'*?)2?*729*8'"*?)"*$778&"*'9'?"7*
!-&-(.-&2.*P&V3-#$"'*
P#-AV>"*5"..*X42&'N"4*
•! 5"?8]$723*•! ?42'?8%8723*
•! X5S*"&/$&""4$&/*
•! 5PS'*•! ;"$V(*("..'*
X24/"?"#*P&V3-#$"'*
6778&-?)"42A9*
5"..8.24**6778&-?)"42A9*
P&V/"&a* !-&-(.-&2.*

W%>+"289/'9#'O'B%""'2B8P289/'_'32"2/B)/>'2B8P28/>'2/&')/1)3)09$C',)>/2",'
!"..72&Q*U2?84"*IJGG*
'7,8,!)*,!9*:++);<,!()*+,(8!=>*!(:?>*!@??:A>(7,*)BC!
9%8$2$-4*.'*"("#-4*1:'$";'$++,%"'(8"(!#4$%-1'#/).')'!".'*4/"'$%')0)#6<"'$++,%$-.='•! ")@A(,A)AD,!>=!B,*@B7,*)<!!!!!!!8,<=!(><,*)AD,!•! 4*,E,AF>A!>=!):(>G@??:A@(C!
>*)%1$"%-'"?#*"11$4%'4%'7,%(64%)/'"@"(-4*'>'("//1'!A,1-)$%"0'"?#*"11$4%'4%'0.17,%(64%:'$"';"?8),1-"0'>'("//1'

GY*
]%B12/),.'9#'6O7!A='2/&'?@A<')/1)3)89/'_''&)h%$%/0'9$',8""'`+)0%',).)"2$'i'
D9$Q*RB<C*1"f*IJGY*

IpilimumabPhase2CA184-041:StudySchema
Lynchetal,JCO2012
1°endpoint irPFSOther PFS,BORR,irBORR,OS,safety

19&()*"?*2.Q*\5+*IJGI*
-*)").).23'?12,%':'6!<L=A;=<I''50+&C'5B1%.2'
?12,%&'
69/B+$$%/0'
-*)").+.23I'45676'*12,%'---'0$)2"'
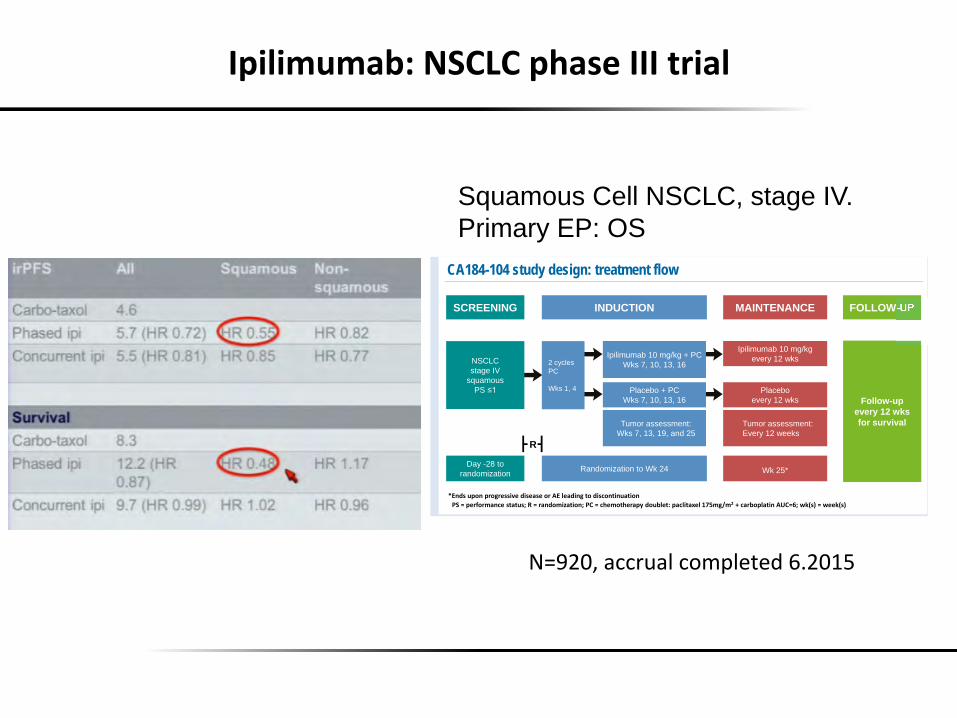
CA184-104: Randomized, Multicenter, Double-Blind, Phase 3 Trial Comparing the Efficacy of Ipilimumab with Paclitaxel/Carboplatin versus Placebo with Paclitaxel/Carboplatin in Patients with Stage IV/Recurrent Non-Small Cell Lung Cancer of Squamous Histology
Background • Years of research in advanced non-small cell lung cancer (NSCLC) have
not improved outcomes for the squamous cell subtype beyond those of standard platinum doublets
• Increasing evidence of responses to immune therapies in NSCLC of squamous cell histology support continued clinical development of immunotherapy in this subtype
• Ipilimumab – A fully human, IgG1 monoclonal antibody which blocks cytotoxic T-
lymphocyte antigen-4 (CTLA-4) and augments antitumor T-cell responses
– CTLA-4 is a negative regulator of T-cell activation – Blockade of CTLA-4 on T cells—which allows CD28 to interact with
B7—can augment T-cell activation, proliferation, and infiltration into tumors, leading to cell death1 (Figure 1)
– Does not kill tumor cells directly, but rather, causes tumor cell death indirectly via activated T cells
• Ipilimumab in metastatic melanoma – Demonstrated overall survival (OS) benefit in two phase 3 trials for
advanced melanoma1-3
– Manageable adverse event (AE) profile using product-specific guidelines1,3
– Approved in many countries at a dose of 3 mg/kg for treatment of patients with unresectable or metastatic melanoma3+reference ex-US labels
~254 sites in 35 countries
53E
CA184-104* trial design and endpoints • Randomized, double-blind, phase 3 trial (Table 1)
• Patients with Stage IV or recurrent†/squamous NSCLC
• Phased schedule of first-line P (175 mg/m2 q3w x 2) / C (AUC = 6 q3w x 2) followed by ipilimumab (10 mg/kg q3w x 4 � q12w) and P (175 mg/m2 q3w x 4) / C (AUC = 6 q3w x 4) vs placebo plus PC
CT = paclitaxel (175 mg/m2) plus carboplatin (AUC = 6) or carboplatin (AUC 5); Ipi = ipilimumab (10 mg/kg)
CA184-104 inclusion and exclusion criteria • Patient population: Stage IV or recurrent†/squamous NSCLC (Tables 2a and 2b)
– Per the 7th edition of the TNM classification of malignant tumors, Stage IV NSCLC is classified as any T, any N, and M1
– Diagnosis of squamous NSCLC was histologically or cytologically confirmed from brushing, washing or needle aspiration of a defined lesion, but not from sputum cytology alone
• Targeted enrollment: 920 patients
• Argentina • Australia • Austria • Belgium • Brazil • Canada • Chile • Colombia • Czech
Republic • Denmark • France • Germany
• Hong Kong • Hungary • Ireland • Israel • Italy • Korea • Mexico • Netherlands • Peru • Poland • Portugal • Romania • Russian
Federation
Table 2a. Inclusion criteria
Squamous cell NSCLC
Stage IV or recurrent† NSCLC
ECOG Performance Score of 0 or 1
Table 2b. Exclusion criteria
Brain metastases
Autoimmune disease
Presented at the American Society of Clinical Oncology 2012 Annual Meeting, June 1–5, 2012; Chicago, IL, USA
• Singapore • South Africa • Spain • Sweden • Switzerland • Taiwan • Thailand • Turkey • United
Kingdom • United States
CA184-104 study design • Induction phase
– Two cycles of chemotherapy (PC; paclitaxel [175 mg/m2] plus carboplatin [AUC = 6], followed by PC plus ipilimumab (10 mg/kg) or PC plus placebo every 3 weeks
� 4 cycles of ipilimumab or placebo
� Up to 6 total cycles of PC
– Randomized 1:1 PC/ipilimumab or PC/placebo
• Maintenance phase
– Patients without progressive disease after the induction phase offered ipilimumab (10 mg/kg) or placebo q12w starting at Week 25 until progressive disease, per mWHO
Current as of April 11, 2012 (www.clinicaltrials.gov)
Treatment stopping criteria • Unacceptable toxicity
• Clinical deterioration
• Confirmed disease progression
References 1. Hodi FS, et al. N Engl J Med. 2010;363:711–23. 2. Robert C, et al. N Engl J Med. 2011;364:2517–25. 3. YERVOY™ (ipilimumab) [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2011. 4. Fong L, et al. J Clin Oncol. 2008;26:5275–83. 5. Lynch T, et al. Presented at the 2010 European Society for Clinical Oncology Annual Meeting;
October 8–12, 2010; Milan, Italy. Abstract 375PD. 6. Lynch T, et al. Presented at the 2011 World Congress for Lung Cancer; July 3–7, 2011;
Amsterdam, Netherlands. Abstract 701. 7. Reck M, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in
extensive-disease small cell lung cancer: results from a phase II trial. Presented at the 2011 World Congress of Lung Cancer; July 3–7; Amsterdam, Netherlands. Abstract 1365.
8. Hoos A, et al. Semin Oncol. 2010;37:533–546. 9. Wolchok JD, et al. Clin Cancer Res. 2009;15:7412–7420. 10.Eisenhauer EA, et al. Eur J Cancer. 2009;45:228–247. 11. Miller AB, et al. Cancer. 1981;47:207–214.
Martin Reck,1 Haolan Lu,2 Greta Gribkoff,2 Sabine Maier,2 Rachel McGovern,2 Jean-Marie Cuillerot,2 Thomas Lynch3
1Hospital Grosshansdorf, Grosshansdorf, Germany; 2Bristol-Myers Squibb Company, Wallingford, CT, USA; 3Yale Cancer Center and Smilow Cancer Hospital, New Haven, CT, USA
Acknowledgments • The patients and their families • The study sites enrolling patients to the trial • StemScientific, for providing support services for writing, editorial, studio, and production; funded by Bristol-Myers
Squibb
Clinical support • Prior data from a phase 2 study in advanced NSCLC and extensive-disease
small cell lung cancer (CA184-041)5-7 showed activity of ipilimumab and support ongoing phase 3 (CA184-104) evaluation in squamous NSCLC
– CA184-041 utilized a phased schedule of ipilimumab and paclitaxel/carboplatin (PC) (ipilimumab started after 2 cycles of PC)
– Study endpoints were assessed using both modified WHO (mWHO) and immune-related response criteria (irRC)
� irRC evolved from WHO criteria to capture outcomes of patients treated with ipilimumab1,8-11
– Primary endpoint, immune-related progression-free survival (irPFS), was met for phased ipilimumab administration in patients with NSCLC
� Addition of ipilimumab to PC significantly prolonged irPFS, but not mWHO-PFS
� Clinically relevant prolongation of OS with addition of ipilimumab
� Activity appeared to be most pronounced in patients whose NSCLC was of squamous histology
– Addition of ipilimumab did not worsen toxicity associated with PC, and irAEs were managed using protocol-specific guidelines
– Absolute lymphocyte count was not affected by PC, suggesting that PC has no effect on ipilimumab activity
Mechanism of action
Table 1. Endpoints‡ Primary outcome measure:
OS§,ll
Secondary outcome measures: OS in patients who receive at least one dose of blinded study drug
PFS (mWHO)
Best Overall Response Rate (mWHO)
!"
Ipilimumab 10 mg/kg every 12 wks
Placebo every 12 wks
Tumor assessment: Every 12 weeks
Randomization to Wk 24
NSCLC stage IV
squamous PS ��
SCREENING INDUCTION MAINTENANCE FOLLOW-UP
Day -28 to randomization
2 cycles PC Wks 1, 4
Ipilimumab 10 mg/kg + PC Wks 7, 10, 13, 16
Placebo + PC Wks 7, 10, 13, 16
Tumor assessment: Wks 7, 13, 19, and 25
Wk 25*
Follow-up every 12 wks for survival
CA184-104 study design: treatment flow
!"#$#%&'()'*+,-&#./+/0.1#2#$#'+,3)*45+/4),1#!6#$#-7&*)/7&'+%8#3)09:&/;#%+-:4/+<&:#=>?*@A*B#C#-+'9)%:+/4,#DE6$F1#GHI.J#$#G&&HI.J"
Figure 1. Mechanism of action for ipilimumab
A, co-stimulation via CD28 ligation transduces T-cell activating signals; B, CTLA-4 ligation on activated T cells downregulates T-cell responses; C, blocking CTLA-4 ligation enhances T-cell responses4
#$%&'("$)*"+,-."(&"/,"'0*$(,*"-&11&23)4"
-3)$135$(3&)"&-"6&)(,)("
ECOG = Eastern Cooperative Oncology Group; TNM = tumor, node, and metastasis; M1 = distant metastasis
* Further information on enrolling in this trial and participating study sites is available on www.clinicaltrials.gov, identifier: NCT01285609.
† Recurrent disease after patient received curative surgery. ‡ Exploratory endpoints included immune-related PFS, best overall response, and disease-control rate.
§ Assessed until 705 death events have occurred; an interim analysis at 528 events is planned. ll705 events out of 920 randomized patients will be needed to ensure 90% power to detect a statistically significant difference in OS between treatment arms with a Type I error rate of 5% based on a 2-sided log-rank test.
KL,3.#0%),#%')@'&..4M".&+.&#)'#DL#:&+34,@#/)#34.-),/4,0+/4),"
7!"8&*,"(&"/,"
0+&93*,*"
!,-,+,)6,."(&"/,"+,)':/,+,*;'0*$(,*"
† Recurrent disease after patient received curative surgery.
R
Squamous Cell NSCLC, stage IV. Primary EP: OS
UghIJQ*2((482.*(-7A."?"#*KEIJG_*

?"2B%/02'j'0+.9$,'+8")k%'?@A<M?@A7<M?@A7:'')/0%$2B89/'09'%P2&%')..+/%'$%B9>/)89/'
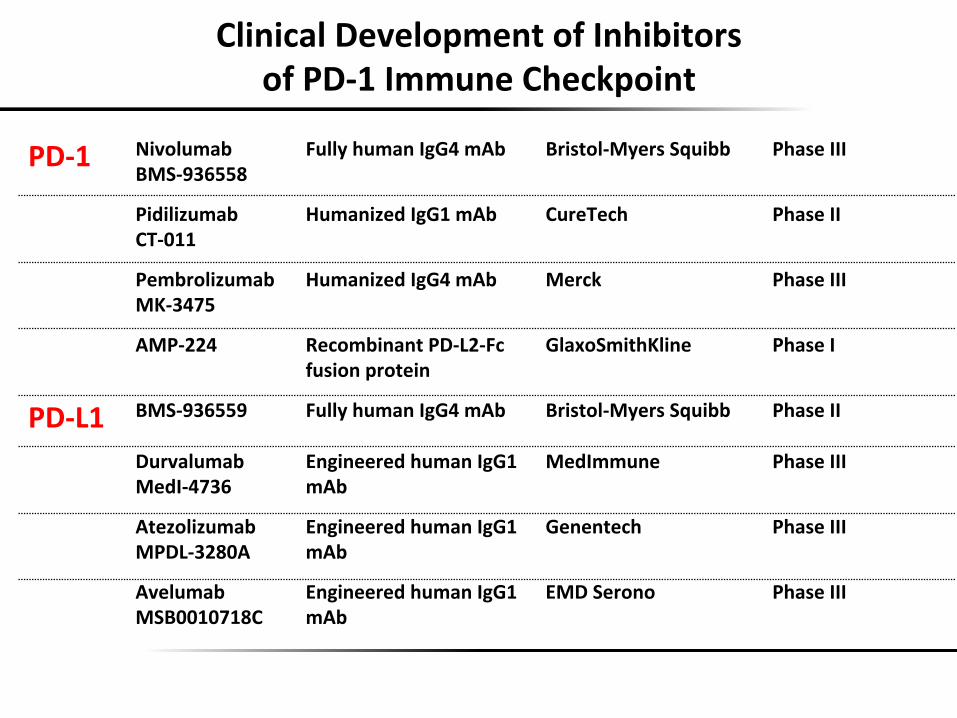
ClinicalDevelopmentofInhibitorsofPD-1ImmuneCheckpoint
PD-1 NivolumabBMS-936558
FullyhumanIgG4mAb Bristol-MyersSquibb PhaseIII
PidilizumabCT-011
HumanizedIgG1mAb CureTech PhaseII
PembrolizumabMK-3475
HumanizedIgG4mAb Merck PhaseIII
AMP-224 RecombinantPD-L2-Fcfusionprotein
GlaxoSmithKline PhaseI
PD-L1 BMS-936559 FullyhumanIgG4mAb Bristol-MyersSquibb PhaseII
DurvalumabMedI-4736
EngineeredhumanIgG1mAb
MedImmune PhaseIII
AtezolizumabMPDL-3280A
EngineeredhumanIgG1mAb
Genentech PhaseIII
AvelumabMSB0010718C
EngineeredhumanIgG1mAb
EMDSerono PhaseIII

PD-1axisimmunotherapyforNSCLC
1. Alookatdatafromearlytrials
2. Evidence-baseddataforan8-PD-1monotherapy
3. Currentevidenceforbiomarker-basedselec8on
4. Upfrontperspec8vesforan8-PD-1therapy

4)P9"+.23'*12,%'<'bUC$,'[nD'/F<:^c'
•! O?'*M"4"*)"2>$.9*A4"?4"2?"#W*_Yi*)2#*L0_*A4$-4*?)"42A$"'* F"j&/"4Q*\5+*IJG_*
?,9@)A!*,8B>A8,!!9:*)F>A!1.!?>8!
%%!1.L!

?%.3$9")k+.23'*12,%'<'&202'bY%C/90%A;;<D'/F=^Ec'
F24-&Q*UB\!*IJG_W*C-4$2Q*BC!+*IJG_*
?$9*9$89/'5B9$%'
o<p' <A=^p' qE;p'
<;KTp ''''''<lKEp'' '=EK:p''''''WW'U^K:p ''''''UTKlp '''''''''':UK:p '?$%P2"%/B%'
' ' ' ' ' ' '?@A7<'%g*$%,,)9/'

!B8P)0C')/'*$%0$%20%&'*28%/0,'
4)P9"+.23' ?%.3$9")k+.23' !0%k9")k+.23' @+$P2"+.23' !P%"+.23'
U' GIh' Yk_G' Gk_' IIH' GHY'
SS*Cl827-8'*U-&*ClE'
*Gki*GHi'
*ILE_i*Ghi'
*Iki*IGi'
*IGi*GLi'
GYi'
;48/*4".*PB*P..*/42#"'*F42#"*L:Y'
*YGi*YEki'
*kGi*hE_i'
*KKi*GGi'
*_Ji*Hi'
*kki*GIi'
SS*O;1aG*m*O;1aG*a'
*GKi*GLi'
*YIi*Zc_Ji[*GJi*ZnGi['
*LYi*65I:L*-4*
X5*I:L'
F"j&/"4*CQ*\*5.$&*+&(-.*IJG_W*LL`*IJJYaIJGIW*T"43'?*SQ*U2?84"*IJGYW*_G_`*_KLakW*C-4$2*\5Q*BC!+*IJGLW**F24-&*BQ*UB\!*IJG_W*LkI`*IJGHaIHW*S$%>$*UQ*PC5+*IJG_W*F8."9*1\Q*PC5+*IJG_*
Gki*GHi
ILE_i*Ghi
Iki*IGi
IGi*GLi
GYi
YEki hE_i GGi Hi GIi
YIi*Zc_Ji[*GJi*ZnGi[
LYi*65I:L*-4X5*I:L
PD-1axisimmunotherapyforNSCLC
1. Alookatdatafromearlytrials
2. Evidence-baseddataforan8-PD-1monotherapy
3. Currentevidenceforbiomarker-basedselec8on
4. Upfrontperspec8vesforan8-PD-1therapy

5%B9/&'")/%',)/>"%'2>%/0'B1%.901%$2*C').*$9P%,',+$P)P2"'
X)"*#2?232'"*N-4*2*'84>$>2.*2#>2&?2/"*-N*I&#*.$&"*()"7-?)"42A9*$'*'72..*2&#*32'"#*-&*-&.9*-&"*'?8#9*-N*#-("?2]".*>'*<C5*
C)"A)"4#Q*\*5.$&*+&(-.*IJJJ*

?9*"2$'50+&C'
d2&'?""&,$'?"Q*BC!+*IJG_*

?9*"2$I'?@A7<',B9$)/>*
•! O6*'(-4"#*2'**%$B%/02>%'9#'0+.9$'B%"",*******A-'$V>"*0*2&9*$&?"&'$?9*•! -6*'(-4"#*2'**%$B%/02>%'9#'0+.9$'2$%2'''''''M$?)*A-'$V>"*("..'*0*2&9*$&?"&'$?9*
•! O6U'9$'-6U'g*X5*o*_Ji*-4*65*o*GJi*O;a1Gm*•! O6:MU'9$'-6:MU'g*X5*-4*65*o**_i*O;a1Gm*•! O6<M:MU'9$'-6<M:MU*g*X5*-4*65*o**Gi*O;a1Gm*•! O6;'9$'-6;'g*g*X5*-4*65*p**Gi*O;a1Gm*******qEE&-?*2(?82..9*&"/2V>"**
CAGYI*6T5*2''9Q*CA4$&/*<$-'($"&("**

?9*"2$I'R5')/'-OO'*9*+"289/'
d2&'?""&,$'?"Q*BC!+*IJG_*

d2&'?""&,$'?"Q*BC!+*IJG_*
?9*"2$I'R5'3C'?@A7<'%g*$%,,)9/'

T"43'?Q*12&("?*IJG_*
?%.3$9")k+.23'P,K'@9B%02g%"'#9$'*$%P)9+,"C'0$%20%&'?@A7<'*9,)8P%'2&P2/B%&'45676'bY%C/90%A;<;c'

?%.3$9")k+.23'P,K'@9B%02g%"'#9$'*$%P)9+,"C'0$%20%&'?@A7<'*9,)8P%'2&P2/B%&'45676'bY%C/90%A;<;c'
B//!4)F,A(8!M@(7!4NGO1!(:?>:*!B*>B>*F>A!8D>*,!>=!CD'4*'&*")-"*P!
T"43'?Q*12&("?*IJG_*
?':.>MN>' ' '<;K='.9'@9B%02g%" ''' '''LKE'.9'Q%!/P.1J!BR/P///6*
?'<;'.>MN> '<:KT'.9'@9B%02g%" ''' '''LKE'.9'Q%!/PS1J!BT/P///1!
?':.>MN>' ' 'UK^'.9'@9B%02g%" ''' '=K;'.9'Q%!/P66J!BR/P/.*
?'<;'.>MN> '=K;'.9'@9B%02g%" ''' '=K;'.9'Q%!/P.UJ!BR/G//V!

?%.3$9")k+.23'P,K'@9B%02g%"'#9$'*$%P)9+,"C'0$%20%&'?@A7<'*9,)8P%'2&P2/B%&'45676'bY%C/90%A;<;c'
T"43'?Q*12&("?*IJG_*
4)F,A(8!M@(7!4NGO1!(:?>:*!B*>B>*F>A!8D>*,!>=!EFD'4*'&*")-"*;'
?':.>MN>' ' '<=K^'.9'@9B%02g%" ''' '''LK:'.9'Q%!/PWVJ!BR/P///-*
?'<;'.>MN> '<TKU'.9'@9B%02g%" ''' '''LK:'.9'Q%!/PW/J!BT/P///1!
?':.>MN>' ' 'EK;'.9'@9B%02g%" ''' '=K<'.9'Q%!/PWUJ!BR/P///1*
?'<;'.>MN> 'EK:'.9'@9B%02g%" ''' '=K<'.9'Q%!/PWUJ!BT/P///1!
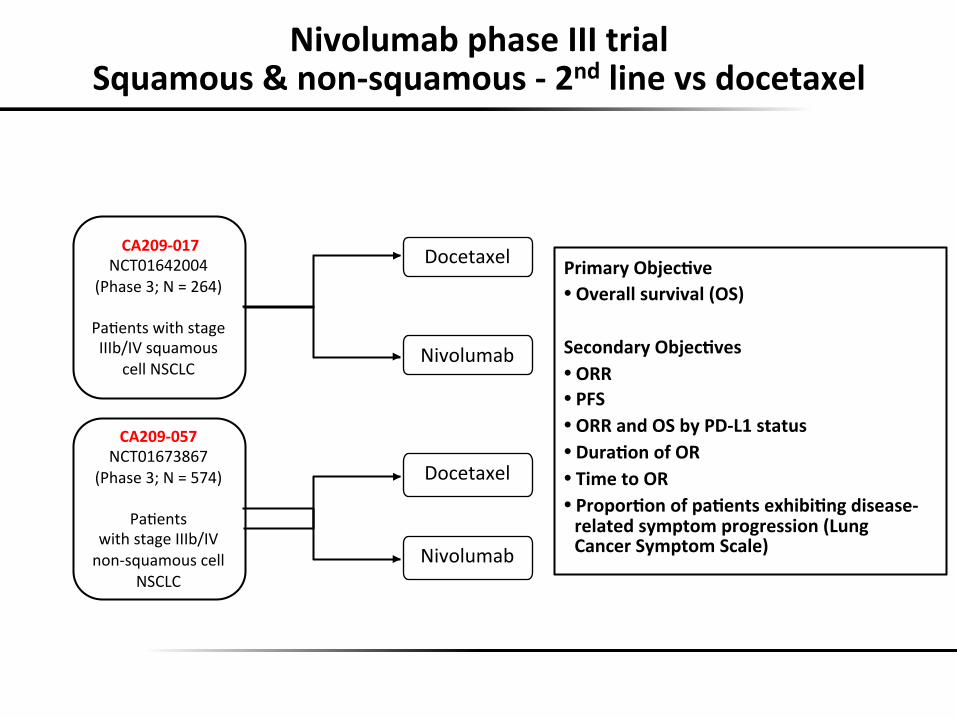
PrimaryObjec8ve• Overallsurvival(OS)SecondaryObjec8ves• ORR• PFS• ORRandOSbyPD-L1status• Dura8onofOR• TimetoOR• Propor8onofpa8entsexhibi8ngdisease-relatedsymptomprogression(LungCancerSymptomScale)
Docetaxel
Nivolumab
Docetaxel
Nivolumab
CA209-017NCT01642004
(Phase3;N=264)
PaVentswithstageIIIb/IVsquamous
cellNSCLC
CA209-057NCT01673867
(Phase3;N=574)
PaVentswithstageIIIb/IVnon-squamouscell
NSCLC
NivolumabphaseIIItrial
Squamous&non-squamous-2ndlinevsdocetaxel

RP%$2""'5+$P)P2"'b6!:;^A;<Tc'
4)P9"+.23''/F<UE'
@9B%02g%"''/F<UT'
.R5'.9''Zh_i*56[*
^K:'ZkELLQ*GIEKI[*
lK;'Z_EIhQ*kELh[*
s'%P%/0,' GJL* GII*
'mWF;Kl:'b;K=LD';KL<ct'GF;K;;;='
!$&$787*N-..-Ma8A*N-4*'84>$>2.`*GH*7-&?)'*•! C84>$>2.*M2'*7-&$?-4"#*8&V.*#"2?)*-4*M$?)#42M2.*-N*(-&'"&?**
Docetaxel 18-month OS rate=13%
OS
(%)
Time (months)
0 6 14 25 37 51 57 69 86 113 135 0 Nivolumab Number of Patients at Risk
0 4 7 11 17 22 33 46 69 104 137 Docetaxel 1
Nivolumab 18-month OS rate=28%
100 90 80 70 60 50 40 30
10 0
20
33 27 24 21 18 15 12 9 6 3 0 30
SS`*IJi*>'*hi*
<42)7"4*"?*2.E*UB\!*IJG_*
.R5'.9''Zh_i*56[*
^K:'ZkELLQ*GIEKI[*
lK;'Z_EIhQ*kELh[*
NivolumabSS`*IJi*>'*hi*

\eB2BC'3C'?@A7<'\g*$%,,)9/'b6!:;^A;<Tc'
<42)7"4*"?*2.E*UB\!*IJG_*

<:A.9'R52 <LA.9'R53
4)P9'b/'F':^:c' @9B'b/'F':^;c' 4)P9'b/'F':^:c' @9B'b/F':^;c'
.R5D'.9,' <:K:' ^K=' GIEI* hEY*
<AC%2$'R5'$20%D'p' _G* Lh* _G* Lh*
<LA.9'R5'$20%D'p' 0* 0* Lh* IL*
49K'9#'%P%/0,D'/M4' GhJ:IhI* IIL:IhJ* IJK:IhI* ILK:IhJ*
mW'b^lp'6-c'F';KTU'b;KE^D';KL^c'G'F';K;;<E'
mW'b^Ep'6-c'F';KT:'b;Kl;D';KLLc'?9,0A19B'G''H';K;;;^B'
!$&$787*N-..-Ma8A*N-4*GIa7-*+C*42?"Q*GLEI*7-'W*N-4*GHa7-*+C*42?"Q*GkEG*7-'*
100 90 80 70 60 50 40 30
10 0
20
27 18 15 9 6 21 12 3 0 24 30
Nivolumab Docetaxel
Number of patients at risk (18-mo OS)b 292 233 195 171 148 128 107 55 4 27 290 244 194 150 111 89 61 23 4
0 0 6
Nivolumab Docetaxel
Nivolumab Docetaxel
Number of patients at risk (12-mo OS)a 292 232 194 169 146 123 62 32 0 9 290 244 194 150 111 88 34 10 0 5
18-mo OS rate = 23%
18-mo OS rate = 39%
1-yr OS rate = 39%
1-yr OS rate = 51%
Time (Months)
OS
(%)
WWI'<:p'P,'^p'
RP%$2""'5+$P)P2"'b6!:;^A;ETc'
<-4/)2"$*"?*2.E*UB\!*IJG_*
.R5D'.9, <:K:' ^K='
<AC%2$'R5'$20%D'p' _G Lh
32 09
WWI'<:p'P,'^p'

\eB2BC'3C'?@A7<'\g*$%,,)9/'b6!:;^A;ETc'

6")/)B2"'0$)2"' R5'2""' R5'/9/'5u66' R5',`+2.9+,'
;-("?2]".*>'*<C5' k*>'*YEK* UP* UP*
;-("?2]".*>'*O"7' kEh*>'*HEL* H*>'*hEL* kEY*>'*KEI*
;-("?2]".*>'*B4.-V&$3*ZX2$.-4[' HEI*>'*_EY* UP* UP*ZIYi[**
;-("?2]".*4278($48723*>'*;-("?2]".*ZS">".['
GJE_*>'*hEG* GGEG*>'*hEk* hE_*>'*HEI*
;-("?2]".*&$&?"&$3*>'*;-("?2]".*Z187"a18&/aG['
GJEG*>'*hEG**
GIEK*>'*GJEL* HEK*>'*HEk*
U$>-.8723*>'*;-("?2]".' UP* GIEI*>'*hEY* hEI*>'*KEJ*
P?"%-.$%8723*>'*;-("?2]".' GGEY*>'*hE_* UP* UP*
@9B%02g%"'$2/&9.)k%&'$%,+"0,')/'<E'C%2$,'
U$>-.8723*>'*;-("?2]". UP* GIEI*>'*hEY* hEI*>'*KEJ*hEI*>'*KEJ*

m9J%P%$I'09g)B)0Cv'
O9g)B)0C' 4)P9"+.23'',`+2.9+,'p'
@9B%02g%"',`+2.9+,''p''
!#28/)3',`+2.9+,'p'
@9B%02g%"'M'W2.+B)$+.23'p'
P..' _h' Hk' hL' hH'
F42#"**LaY' H' _H' _k' kh'
F42#"*_' J' I' I' _'
F42#"**LaY H _H _k kh

O1%'&%")B20%'32"2/B%'9#')..+/901%$2*C'_'2+09)..+/%')/w2..289/'
5)27A$2?Q*P&&*+&(-.*IJG_*

!&P%$,%'\P%/0']2/2>%.%/0'
5)27A$2?Q*P&&*+&(-.*IJG_*

YI*U$')$&-*"?*2.E*UB\!*IJG_*
!2&#".Q*\*U"84-.*C($"&("*IJGYW*1@83.$*"?*2.Q*\*6778&-?)"4*52&("4*IJG_*W**
!/8_?@A<_W%"20%&')$!\'&+$)/>'62/B%$'-..+/901%$2*C'
*

PD-1axisimmunotherapyforNSCLC
1. Alookatdatafromearlytrials
2. Evidence-baseddataforan8-PD-1monotherapy
3. Currentevidenceforbiomarker-basedselec8on
4. Upfrontperspec8vesforan8-PD-1therapy

\g*$%,,)9/'9#'?@A7<'),'1%0%$9>%/%9+,'2/&'P2$)%,'J)01'2/839&C'+,%&'
!(128/).$&Q*\P!P*+&(-.-/9*IJGK*BG1LU*g*5"..*C$/&2.$&/*X"()&-.-/9*COGYI*g*CA4$&/*<$-'($"&("*

?@A7<'*9,)8P)0C'),'2'w%g)3"%'B9/B%*0'

m)>1'.+0289/2"'3+$&%/'*$%&)B0,'$%,*9/,%'09'*%.3$9")k+.23')/'45676'
Rizvi, Science 2015
GX!?:()F>A)<!<>)9!@8!@?B>*()A(J!;:(!?)C!A>(!;,!=,)8@;<,!!!!!!D:**,A(<C!@A!>:*!9)@<C!B*)DFD,!

?@<'!3,')/'x'9/B9>%/%A2&&)B0%&'y'45676'_'\eB2BC'9#'?%.3$9")k+.23')/'N%C',+3>$9+*,'
T"..72&&Q*r515Q*IJG_*
>* >* >*

O$%20.%/0'\h%B0'9/'RP%$2""'5+$P)P2"'2BB9$&)/>'09'5+3>$9+*'b6!:;^A;ETc'
<-4/)2"$*"?*2.E*UB\!*IJG_*

-/f"0$289/'J)01'O-7,')/'45676'
B+$$%/0"C'/9'''',02/&2$&)k289/D'8,,+%'.)>10'3%'2'").)8/>'#2B09$z'
<4273$..2Q*\5+*IJGK*

\.3$2B)/>'B9.*"%g)0C'09'+/&%$,02/&'B1%BN*9)/0')/1)3)89/'
d2&*P.."&*"?*2.Q*C($"&("*IJG_*

Areweeverreadytoselectpa8ents?
ComplexityofimmunesurveillanceandescapemightpreventusfromidenFfyingasimple&uniquepredicFvebiomarker.
Image from J. Allison

PD-1axisimmunotherapyforNSCLC
1. Alookatdatafromearlytrials
2. Evidence-baseddataforan8-PD-1monotherapy
3. Currentevidenceforbiomarker-basedselec8on
4. Upfrontperspec8vesforan8-PD-1therapy
Z-W6mI'!0%k9")k+.23')/'?@A7<{'*28%/0,'
<"''"Q*BC!+*IJG_*

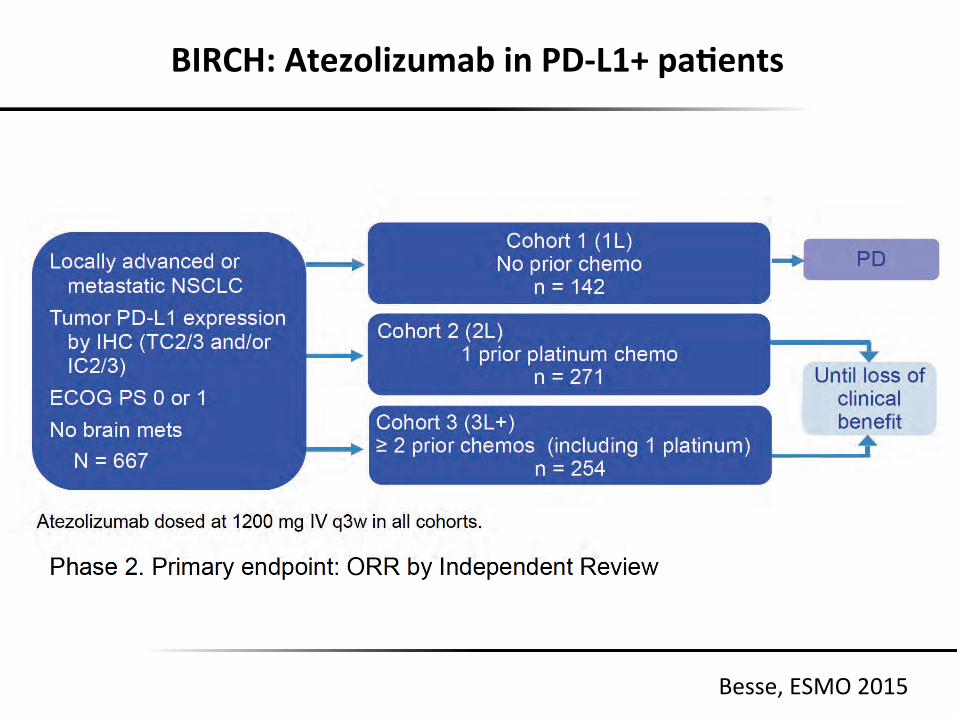
BIRCH:AtezolizumabinPD-L1+pa8ents
Besse,ESMO2015
0
10
20
30
1L 2L 3L+
26% 24%
27%
19% 17% 17%
TC2/3 or IC2/3 TC3 or IC3
OR
R, %
N=115 N=253 N=267 N=139 N=65 N=122
BIRCH:ObjecFveResponseRateTC3orIC3SubgroupvsTC2/3orIC2/3SubgroupbyCohort

PhaseIIItrialsin1st-lineadvancedNSCLC(selected)
Nivolumab
Pembrolizumab
MEDI4736
SOC=standard of care. ClinicalTrials.gov. http://www.clinicaltrials.gov/. Accessed August 2015.
KEYNOTE-042 Pembrolizumab
SOC chemotherapy Primary endpoint: OS PD-L1+ NSCLC
N = 1240
Primary endpoints: OS, PFS
Treatment-naïve or recurrent NSCLC N = 1980 CheckMate 227
Nivolumab
Nivolumab + ipilimumab
Platinum-based chemotherapy
Primary endpoint: PFS Treatment-naïve or recurrent PD-L1+ NSCLC N = 535 CheckMate 026
Nivolumab
Investigator’s choice chemotherapy
KEYNOTE-024 Pembrolizumab
Platinum-based chemotherapy Primary endpoint: PFS PD-L1 strong NSCLC
N = 300
Atezolizumab
IMpower 111 Atezolizumab
Gemcitabine + cisplatin or carboplatin Primary endpoint: PFS Stage IV squamous PD-L1+ NSCLC
N = 400
IMpower 150
Atezolizumab + carboplatin + paclitaxel
Bevacizumab + paclitaxel + carboplatin
Primary endpoint: PFS Stage IV non-squamous NSCLC N = 1200 Atezolizumab + bev. + paclitaxel + carboplatin
IMpower 130 Atezolizumab + carboplatin + nab-paclitaxel
Carboplatin + nab-paclitaxel Primary endpoint: PFS Stage IV non-squamous NSCLC
N = 550
IMpower 110 Atezolizumab
Carboplatin or carboplatin + pemetrexed Primary endpoint: PFS Stage IV non-squamous PD-L1+ NSCLC
N = 400
IMpower 131
Atezolizumab + carboplatin + nab-paclitaxel
Carboplatin + nab-paclitaxel
Primary endpoint: PFS Stage IV squamous NSCLC N = 1200 Atezolizumab + carboplatin + paclitaxel
Primary endpoint: PFS Advanced NSCLC N = 675
MYSTIC
MEDI4736
MEDI4736 + tremelimumab
SOC chemotherapy
IPI + Paclitaxel/Carboplatinà IPI
Pbo + Paclitaxel/Carboplatin à Pbo Primary endpoint: OS Squamous NSCLC
N = 920 CA184-104
IPI + Paclitaxel/Carboplatinà IPI
Pbo+ Paclitaxel/Carboplatin à Pbo Primary endpoint: OS Squamous NSCLC
N = 867 CA184-153
Ipilimumab
Ant
i-PD
-1/P
D-L
1 A
nti-
CTL
A-4

_K*
m9J'&9'J%'9P%$B9.%'0$%20.%/0'$%,),02/B%')/'01%,%'*28%/0,'i'
S$%>$*"?*2.EQ*12&("?*+&(-.-/9*IJG_*
q'T;p'62/'J%'%g*%B0'2'*90%/82"'$9"%'#9$')..+/901%$2*C')/'01),'*28%/0'*9*+"289/i''

TumorImmuneProfiletounderstandtheimmunemodeofac8onofPD-1/PD-L1blockade
• Serialon-treatmentbiopsies• Neoadjuvanttrials(worldwide)
• DurvalumabinNSCLCstageIIIA(SAKK16/14)• mRNAvaccineinresectableNSCLC(Basel)• NivolumabinStageII-IVRCC• PembrolizumabinTNBC• PembrolizumabinStageIII/IVmelanoma• Pembrolizumabinrectalcancer

_H* S$%>$Q*r515*IJG_*
\P9"P)/>',C/%$>),8B')..+/901%$2*C'B9.3)/289/,'_'B9/B9.)02/0'6O7!A='2/&'?@<'3"9BN2&%'b61%BN.20%';<:c'

_h*_h*!"."4-Q*U2?*S">*52&("4*IJG_*
O4->$#"#*39*1E*<83"&#-4NQ*O2?)-.-/9*=C<*
6@L'
?@<'
/9/A)..+/9>%/)B' )..+/9>%/)B'
•! 12(,*-N*$778&"*2(V>2V-&*
•! 12(,*-N*()"7-,$&"'*
•! ;"&'"*'?4-72*•! 6778&-a
'8AA4"''$>"*-&(-/"&"*"]A4"''$-&*
•! B]A4"''$-&*-N*$&)$3$?-49*4"("A?-4'*
•! X*("..*"])28'V-&*
•! O4"'"&("*-N*4"/8.2?-49*$778&"*("..'*
\P9"P)/>',C/%$>),8B')..+/901%$2*C'B9.3)/289/,'J)01',02/&2$&'9#'B2$%'09''$%*$9>$2.'01%'0+.9$'%/P)$9/.%/0'

-..+/901%$2*C'/90'J9$N)/>'i'_'B1%BN'C9+$'.)B$93)902'z'
C$>2&Q*C($"&("*IJG_W*d"V%-8Q*C($"&("*IJG_*

TakeHomeMessages
• RemarkablyexciVngandeffecVvedrugs!
• IsitrighttoexcludePD-L1negaVvepaVents?
• Biomarker–complex,needsmoreresearch
• Datafromlargephase3studiesareawaited
• CureinNSCLC–haveprogressed,butnotthereyet!

9++,%4/4&$()/'(4%-*4/'I$//'2"')'(*$6()/'-4'-8"'"<"%-,)/'+)1-"*.'4<"*'()%("*;'
O<>C9!a!3<9!b1U22!c!-/11d!














![Research Paper Tumor hypoxia modulates podoplanin/CCL21 ......MDA-MB-231 breast cancer cells, expression of CCR7 drives metastases into lymph nodes [13]. This also occurs in melanoma](https://static.fdocuments.in/doc/165x107/600da90c94b102310c3f3dc9/research-paper-tumor-hypoxia-modulates-podoplaninccl21-mda-mb-231-breast.jpg)



