
009.dental plaque
25
Dr Jaffar Raza Syed Page 1 Dental plaque “WHO specific but highly variable structural entity resulting from colonization and growing microorganisms on surfaces of teeth and consisting of numerous microbial species and strains embedded in an extracellular matrix” “Dental Plaque is an adherent intercellular matrix consisting primarily of proliferating microorganisms, along with a scattering of epithelial cells, leukocytes and macrophages.”
-
Upload
jaffar-syed -
Category
Health & Medicine
-
view
138 -
download
7
Transcript of 009.dental plaque
Dr Jaffar Raza Syed Page 1
Dental plaque
“WHO specific but highly variable structural entity resulting from
colonization and growing microorganisms on surfaces of teeth and consisting
of numerous
microbial species and strains embedded in an extracellular matrix”
“Dental Plaque is an adherent intercellular matrix consisting primarily of
proliferating microorganisms, along with a scattering of epithelial cells,
leukocytes and macrophages.”
Dr Jaffar Raza Syed Page 2
Composition of plaque.
A. Microorganisms: 500 distinct species:
• Bacterial
• Non-bacterial
(a) Mycoplasma
(b) Yeasts
(c) Protozoa
(d) Viruses
B. Host cells:
• Epithelial cells
• Macrophages
• Leukocytes
Dr Jaffar Raza Syed Page 3
C. Organic compounds:
• Polysaccharides
• Proteins
• Glycoproteins
• Lipid materials
D. Inorganic compounds:
• Calcium
• Phosphorous
• Fluoride
• Sodium
• Potassium
Dr Jaffar Raza Syed Page 4
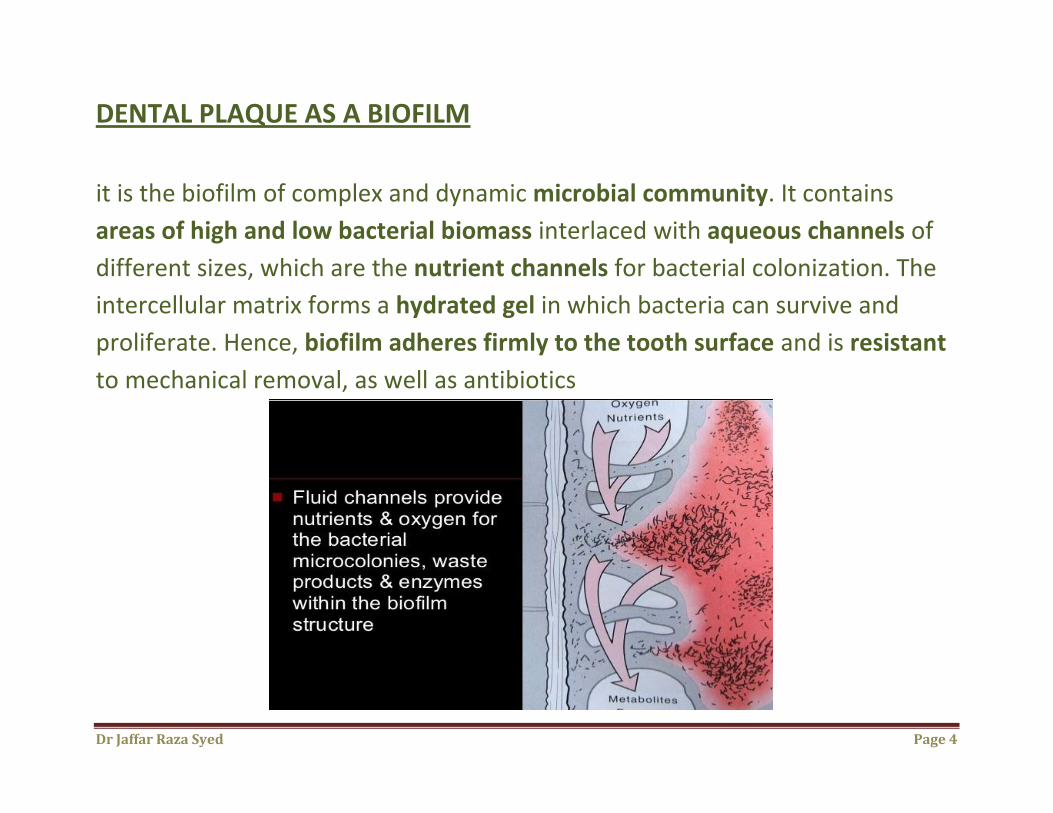
DENTAL PLAQUE AS A BIOFILM
it is the biofilm of complex and dynamic microbial community. It contains
areas of high and low bacterial biomass interlaced with aqueous channels of
different sizes, which are the nutrient channels for bacterial colonization. The
intercellular matrix forms a hydrated gel in which bacteria can survive and
proliferate. Hence, biofilm adheres firmly to the tooth surface and is resistant
to mechanical removal, as well as antibiotics
Dr Jaffar Raza Syed Page 5
TYPES OF DENTAL PLAQUE
plaque is differentiated into two categories, supragingival and subgingival
Supragingival plaque Coronal plaque
Marginal plaque
Subgingival plaque Attached plaque
Unattached subgingival plaque
Attached plaque can be tooth, epithelium and/or
connective tissue associated.
Dr Jaffar Raza Syed
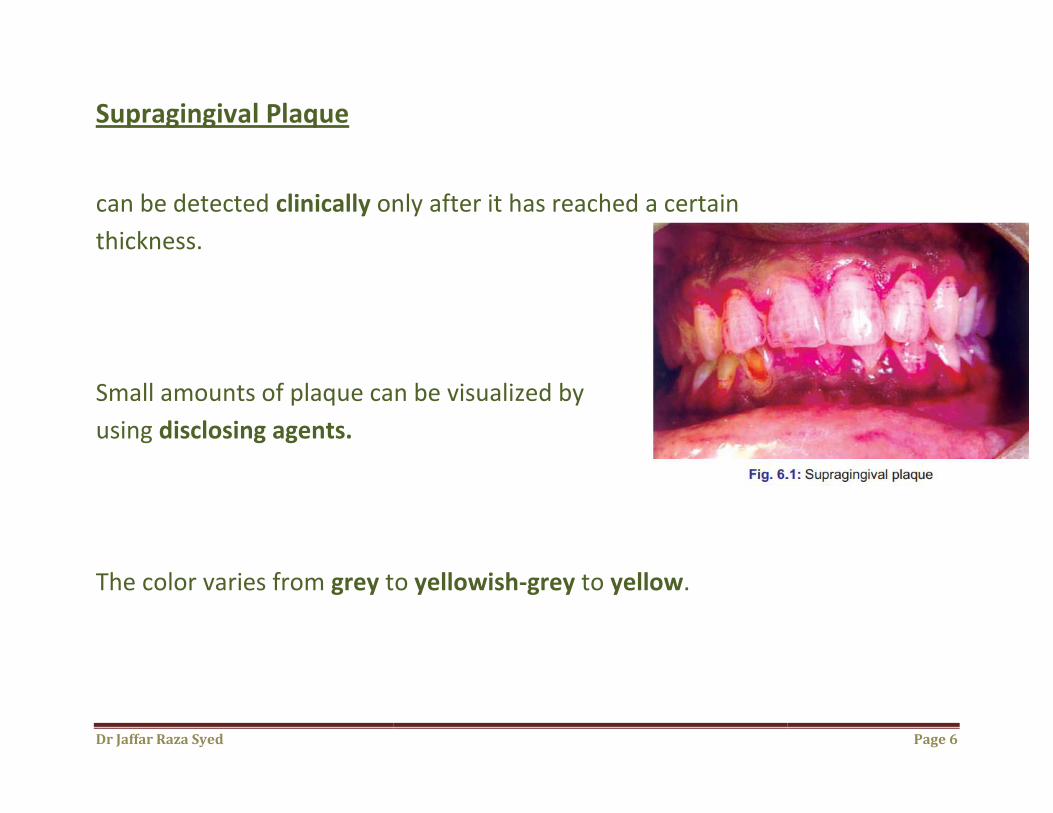
Supragingival Plaque
can be detected clinically only after it h
thickness.
Small amounts of plaque can be visuali
using disclosing agents.
The color varies from grey to
only after it has reached a certain
Small amounts of plaque can be visualized by
to yellowish-grey to yellow.
Page 6
Dr Jaffar Raza Syed Page 7
Subgingival Plaque
usually thin,
contained within the gingival sulci or periodontal pocket and thus cannot be
detected by direct observation.
identified only by running the end of a probe around gingival margin
Dr Jaffar Raza Syed
Page 8
Dr Jaffar Raza Syed
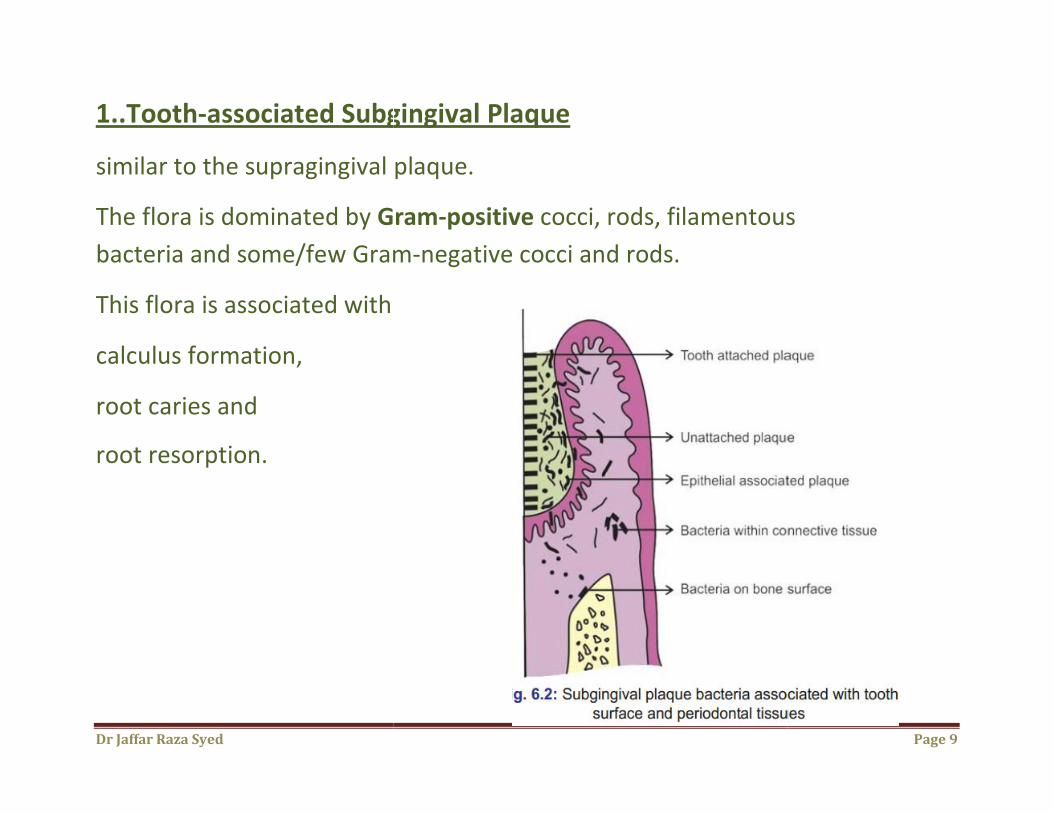
1..Tooth-associated Subgingival Plaque
similar to the supragingival plaque.
The flora is dominated by Gram
bacteria and some/few Gram
This flora is associated with
calculus formation,
root caries and
root resorption.
associated Subgingival Plaque
plaque.
Gram-positive cocci, rods, filamentous
w Gram-negative cocci and rods.
Page 9
cocci, rods, filamentous
Dr Jaffar Raza Syed
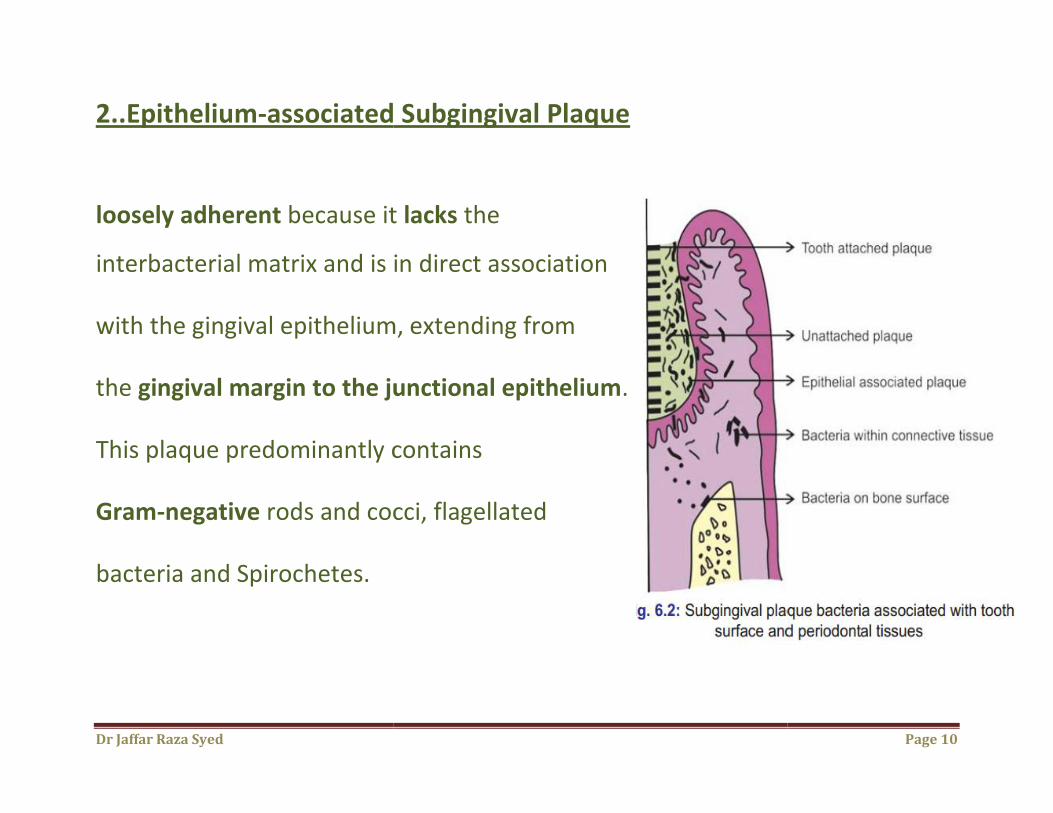
2..Epithelium-associated Subgingival Plaque
loosely adherent because it
interbacterial matrix and is in direct association
with the gingival epithelium, extending from
the gingival margin to the junctional epithelium
This plaque predominantly contains
Gram-negative rods and cocci, flagellated
bacteria and Spirochetes.
associated Subgingival Plaque
because it lacks the
interbacterial matrix and is in direct association
gingival epithelium, extending from
the junctional epithelium.
contains
rods and cocci, flagellated
Page 10
Dr Jaffar Raza Syed
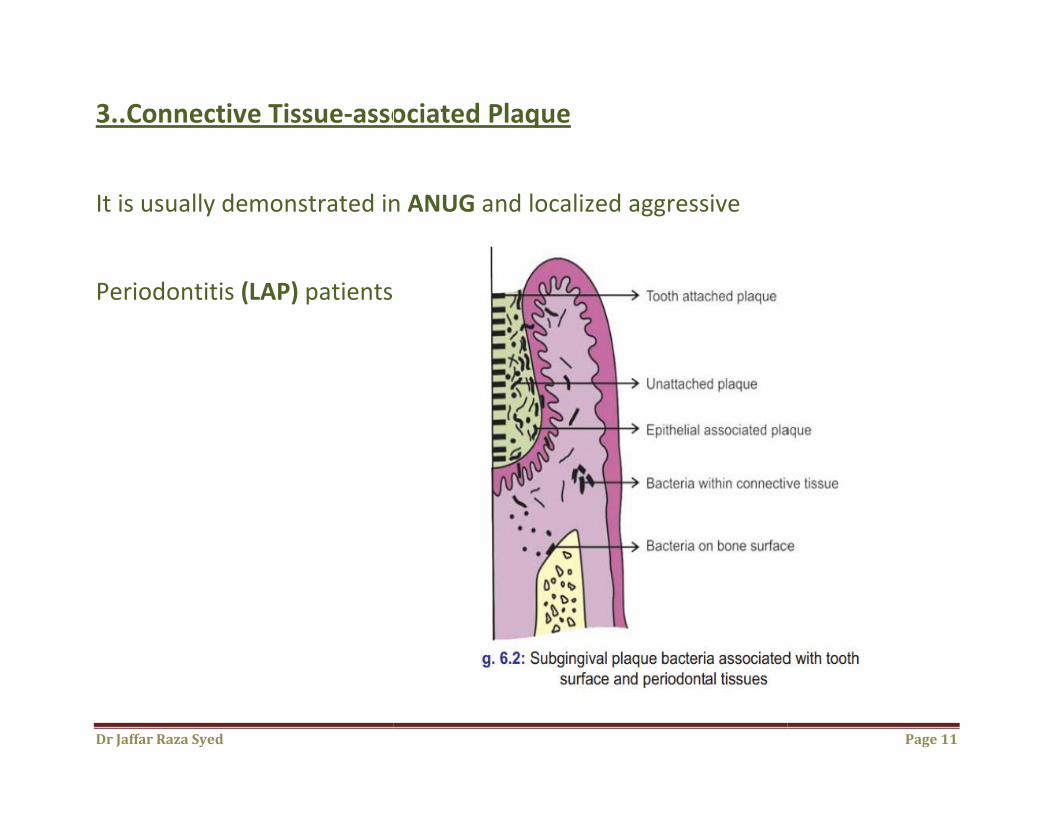
3..Connective Tissue-associated Plaque
It is usually demonstrated in
Periodontitis (LAP) patients
associated Plaque
It is usually demonstrated in ANUG and localized aggressive
Page 11
Dr Jaffar Raza Syed Page 12
Development Of Dental Plaque
Pellicle is the initial organic structure that forms on the surfaces of the teeth
and artificial prosthesis.
The first stage in pellicle formation involves adsorption of salivary proteins
to apatite surfaces.
The transition from pellicle to dental plaque is extremely rapid.
The first components include mainly cocci, epithelial cells and PMNL.
they form a monolayer within a few hours.
Dr Jaffar Raza Syed Page 13
the attached bacteria proliferate and form small colonies of cocci.
With time other types of microorganisms proliferate and form different
microcolonies.
Bacterial Adherence
During initial adherence, interactions occur mainly between specific bacteria
and the pellicle.

Dr Jaffar Raza Syed
1..Bacterial Attachment via Electrostatic Interactions
Oral bacteria bear an overall net negative charge
charged components of the bacterial surface and negatively
charged components of pellicle
such as calcium
Bacterial Attachment via Electrostatic Interactions
overall net negative charge, negatively
charged components of the bacterial surface and negatively
licle become linked by cations
Page 14
Dr Jaffar Raza Syed
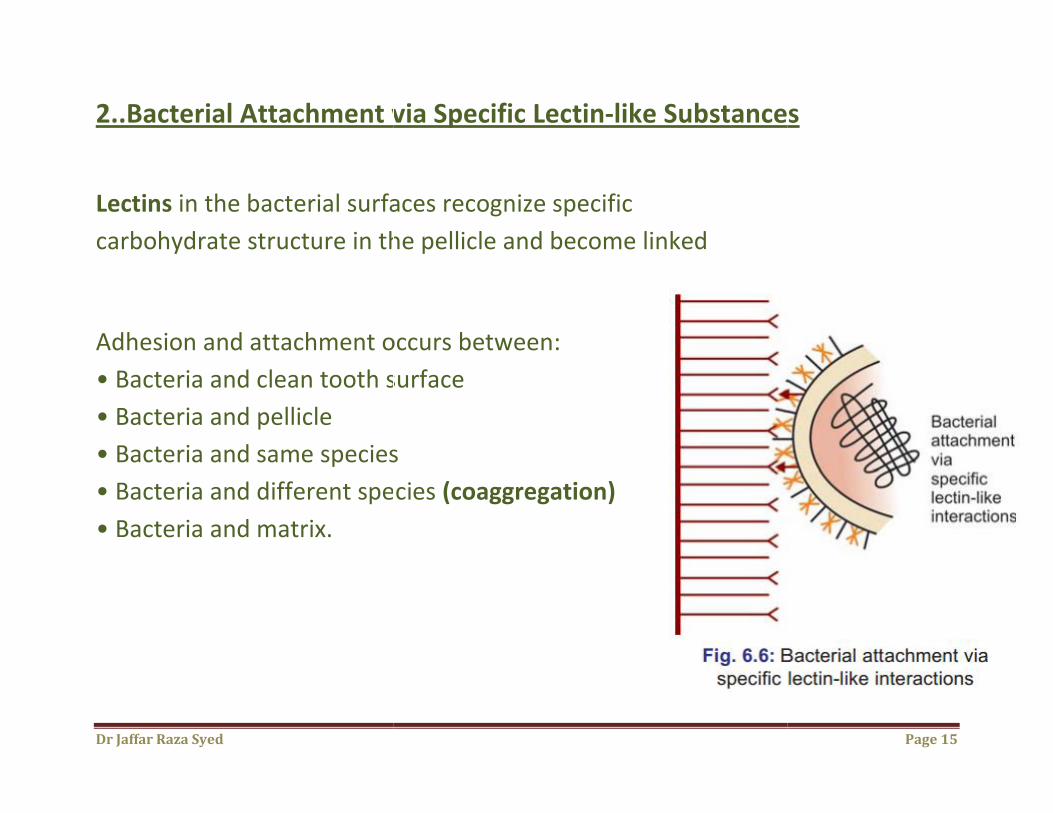
2..Bacterial Attachment via Specific Lectin
Lectins in the bacterial surfaces recognize specific
carbohydrate structure in the pellicle and become linked
Adhesion and attachment occurs between:
• Bacteria and clean tooth surface
• Bacteria and pellicle
• Bacteria and same species
• Bacteria and different species
• Bacteria and matrix.
Bacterial Attachment via Specific Lectin-like Substances
in the bacterial surfaces recognize specific
carbohydrate structure in the pellicle and become linked
occurs between:
• Bacteria and clean tooth surface
• Bacteria and same species
• Bacteria and different species (coaggregation)
Page 15
Substances
Dr Jaffar Raza Syed
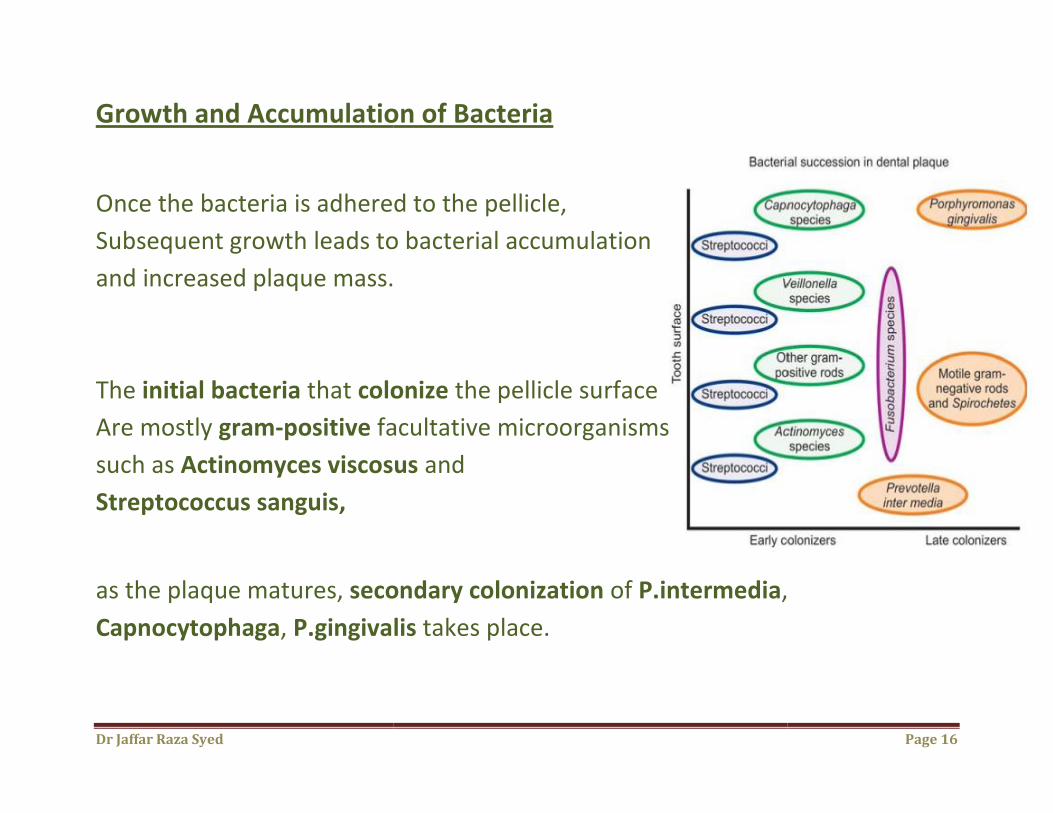
Growth and Accumulation of Bacteria
Once the bacteria is adhered to the pellicle,
Subsequent growth leads to bacterial accumulation
and increased plaque mass.
The initial bacteria that colonize
Are mostly gram-positive facultative microorganisms
such as Actinomyces viscosus
Streptococcus sanguis,
as the plaque matures, secondary colonization
Capnocytophaga, P.gingivalis
Growth and Accumulation of Bacteria
Once the bacteria is adhered to the pellicle,
growth leads to bacterial accumulation
mass.
colonize the pellicle surface
facultative microorganisms
Actinomyces viscosus and
secondary colonization of P.intermedia,
gingivalis takes place.
Page 16
,
Dr Jaffar Raza Syed Page 17
Plaque hypothesis
1..Non-specific plaque hypothesis:
Described by Walter Loesche in 1976.
“Periodontal disease results from the elaboration of noxious products by the
entire plaque flora.”
Shortcomings:
Some individuals with constant amount of plaque and calculus
never developed destructive periodontitis.
Some sites were not affected, whereas advanced disease was
found in adjacent sites.
Dr Jaffar Raza Syed Page 18
2..Specific plaque hypothesis:
Described by Walter Loesche in 1976.
“only certain plaque is pathogenic and its pathogenicity depends on the
presence of or increase in specific microorganisms.”
Shortcomings:
There were occasions when either disease was diagnosed in
the absence of the putative pathogens or when pathogens are
present with no evidence of disease.
Dr Jaffar Raza Syed Page 19
3..Modern version of specific theory:
Described by Socransky in 1979.
According to this theory, 6-12 bacterial species may be responsible
for the majority of cases of destructive periodontitis and additional
species may be responsible for small number of other cases.
Dr Jaffar Raza Syed Page 20
4..Unified theory:
Described by Theilade in 1986.
It is the modern version of non–specific and specific plaque hypothesis.
According to this theory all bacterial plaque may contribute to the pathogenic
potential of the subgingival flora to a greater or lesser extent. This
is due to its ability to colonize and evade host defenses and provoke
inflammation and tissue damage.
Dr Jaffar Raza Syed Page 21
5..Ecological plaque hypothesis:
According to this, any change in the nutrient status of a pocket, i.e. physical
and chemical change to the habitat are considered the primary cause for
overgrowth of pathogens.
Dr Jaffar Raza Syed Page 22
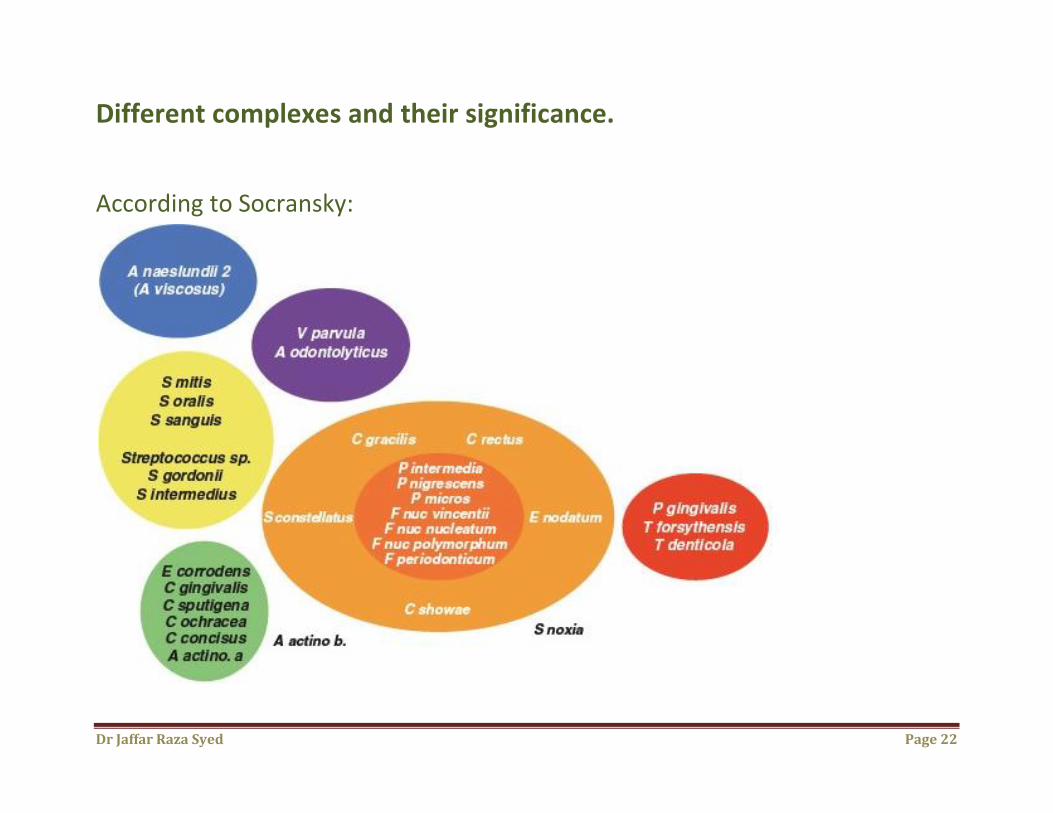
Different complexes and their significance.
According to Socransky:
Dr Jaffar Raza Syed Page 23
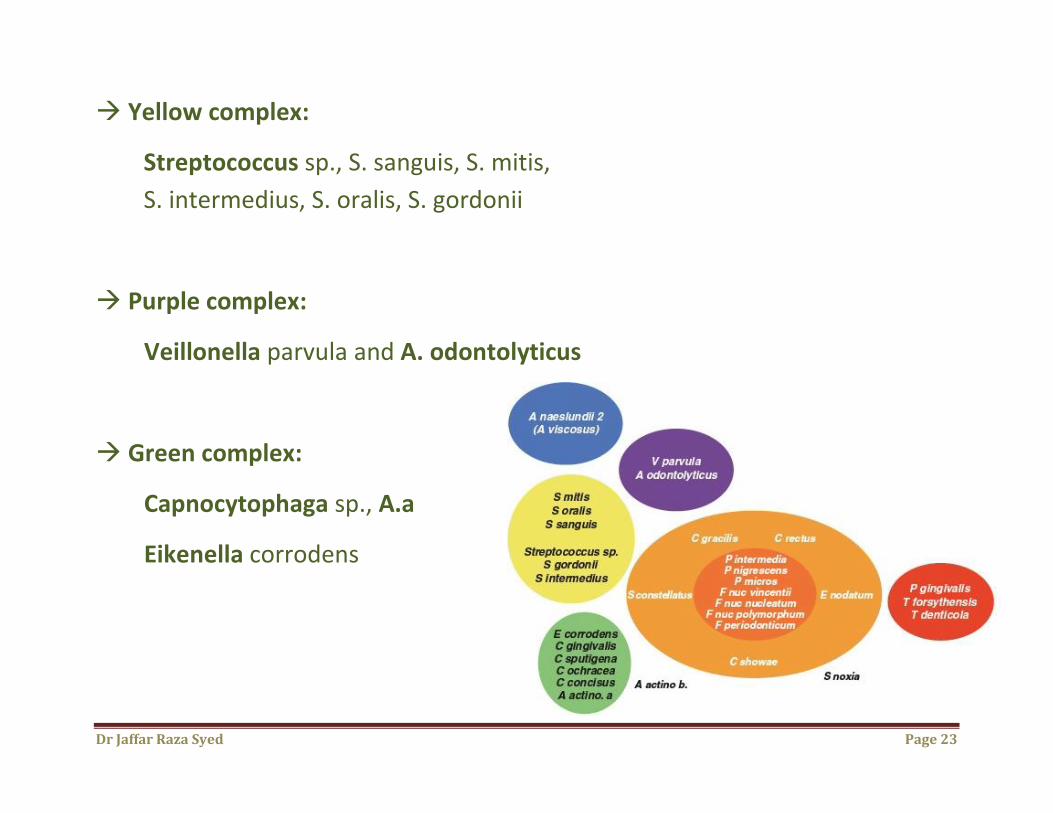
Yellow complex:
Streptococcus sp., S. sanguis, S. mitis,
S. intermedius, S. oralis, S. gordonii
Purple complex:
Veillonella parvula and A. odontolyticus
Green complex:
Capnocytophaga sp., A.a
Eikenella corrodens
Dr Jaffar Raza Syed Page 24
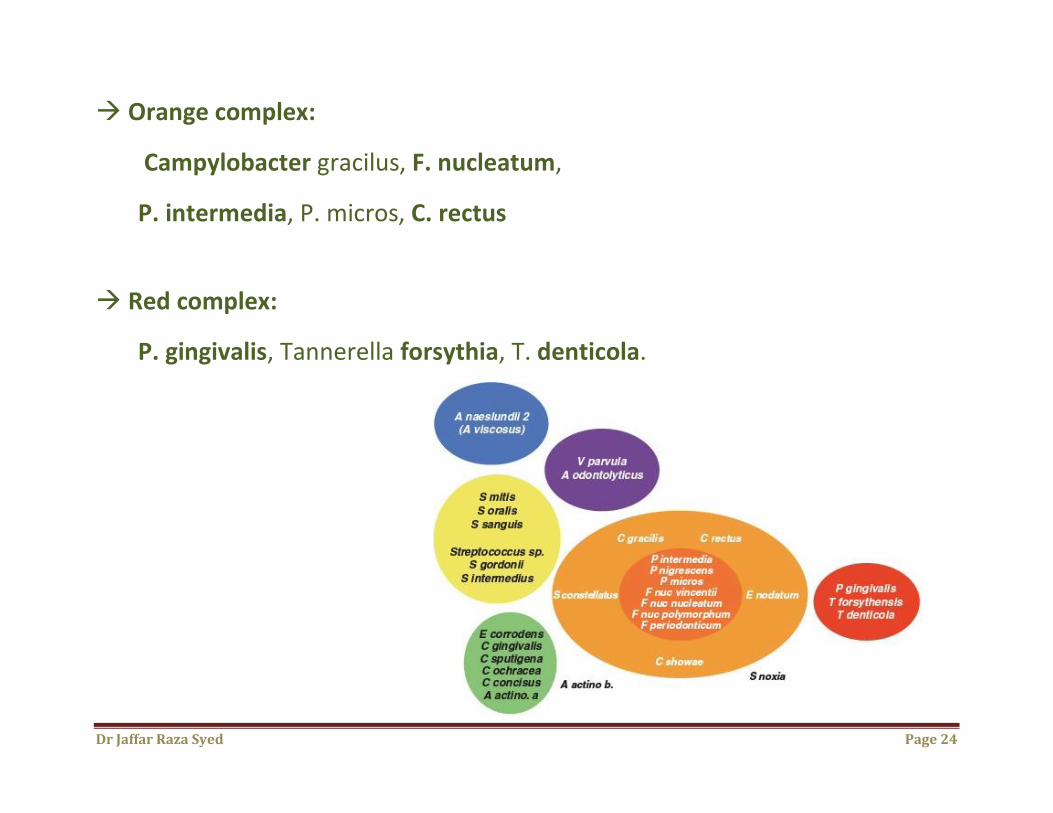
Orange complex:
Campylobacter gracilus, F. nucleatum,
P. intermedia, P. micros, C. rectus
Red complex:
P. gingivalis, Tannerella forsythia, T. denticola.
Dr Jaffar Raza Syed Page 25
Significance:
Early colonizers include members of yellow complexes, purple
complexes and green complexes.
Orange complex members are thought to bridge early colonizers.
Red complex members are associated with bleeding on probing and more
dominant at late stages in plaque development.
Green and orange complexes include species recognized as pathogens in
periodontal and non–periodontal infection.


















