
00005768-900000000-98478
20
. . . Published ahead of Print Prospective Evidence for a Hip Etiology in Patellofemoral Pain Brian Noehren 1 , Joseph Hamill 2 , and Irene Davis 3 1 Division of Physical Therapy, University of Kentucky, Lexington, KY 2 Department of Exercise Science, University of Massachusetts, Amherst, MA 3 Spaulding National Running Center, Harvard University, Cambridge, MA Accepted for Publication: 7 December 2012 Medicine & Science in Sports & Exercise® Published ahead of Print contains articles in unedited manuscript form that have been peer reviewed and accepted for publication. This manuscript will undergo copyediting, page composition, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered that could affect the content. Copyright © 2013 American College of Sports Medicine ACCEPTED
-
Upload
luis-goncalves -
Category
Documents
-
view
3 -
download
0
description
Articulo Fisioterapia Deportiva
Transcript of 00005768-900000000-98478

. . . Published ahead of Print
Prospective Evidence for a Hip Etiology in Patellofemoral Pain
Brian Noehren1, Joseph Hamill2, and Irene Davis3
1Division of Physical Therapy, University of Kentucky, Lexington, KY2Department of Exercise Science, University of Massachusetts, Amherst, MA
3Spaulding National Running Center, Harvard University, Cambridge, MA
Accepted for Publication: 7 December 2012
Medicine & Science in Sports & Exercise® Published ahead of Print contains articles in unedited manuscript form that have been peer reviewed and accepted for publication. This manuscript will undergo copyediting, page composition, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered that could affect the content.
Copyright © 2013 American College of Sports Medicine
ACCEPTED

Prospective Evidence for a Hip Etiology in Patellofemoral Pain
Brian Noehren1, Joseph Hamill2, and Irene Davis3
1Division of Physical Therapy, University of Kentucky, Lexington, KY; 2Department of Exercise
Science, University of Massachusetts, Amherst, MA; 3Spaulding National Running Center, Harvard
University, Cambridge, MA
Address for correspondence:
Brian Noehren PT, Ph.D.
Assistant Professor
University of Kentucky
Division of Physical Therapy
Wethington Bldg. Rm. 204D
900 S. Limestone
Lexington, KY 40536-0200
Phone: 859-218-0581 Fax:859-323-6003
[email protected] [email protected]
Medicine & Science in Sports & Exercise, Publish Ahead of PrintDOI: 10.1249/MSS.0b013e31828249d2
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

The authors do not have any conflict of interests to report.
This study was funded by a Dept of Defense grant DAMD17-00-1-0
Running title: Prospective evaluation of patellofemoral pain
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

Abstract:
Purpose: Patellofemoral pain (PFP) is the leading cause of knee pain in runners. Proximal and distal
running mechanics have been linked to the development of PFP. However, the lack of prospective
studies limits establishing a causal relationship of these mechanics to PFP. The purpose of this study
was to prospectively compare running mechanics in a group of female runners who went on to
develop PFP compared to healthy controls. It was hypothesized that runners who go on to develop
PFP would exhibit greater hip adduction, hip internal rotation, and greater rear foot eversion.
Methods: 400 healthy female runners underwent an instrumented gait analysis and were then
tracked for any injuries that they may have developed over a 2 year period. Fifteen cases of PFP
developed which were confirmed by a medical professional. Their initial running mechanics were
compared to an equal number of runners who remained uninjured.
Results: We found that female runners who developed PFP exhibited significantly greater hip
adduction (p=0.007). No statistically significant differences were found for the hip internal rotation
angle (p=0.47) or rearfoot eversion (p=0.1).
Conclusions: The finding of greater hip adduction in female runners who develop PFP is in
agreement with previous cross sectional studies. These results suggest that runners who develop PFP
utilize a different proximal neuromuscular control strategy than those who remain healthy. Injury
prevention and treatment strategies should consider addressing these altered hip mechanics.
Key words: anterior knee pain, running, kinematics, hip
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
INTRODUCTION:
Patellofemoral pain (PFP) is the most common running related injury, affecting up to 2.5
million runners in the United States alone (6, 27). It is defined as pain along the retro or peri-patellar
region that is exacerbated by weight bearing activities such as running, squatting, and going up and
down stairs. Patellofemoral pain accounts for 43% of injuries military recruits suffer from, as well as
up to 25% of office visits to primary care sports medicine physicians (7, 28). Patellofemoral pain
also disproportionately affects women over men (4). Unfortunately, even at a 5-20 year follow up,
many of these individuals continue to experience pain, which has been related to a decrease in
physical activity including running (3, 17, 25). Emerging evidence suggests that patellofemoral pain
earlier in life increases the risk of developing patellofemoral osteoarthritis later in life (30). The long
term decrease in physical activity has significant healthcare consequences such as an increased risk
for developing diabetes and cardiovascular disease (2). Thus, identifying the potential underlying
mechanics that result in PFP is critical to effectively treat and prevent this chronic condition.
Patellofemoral pain is largely believed to be a stress injury. Malalignment between the patella
and the femur that reduces the contact area leads to increased patellar contact stress (21). Evidence
from a growing number of cross sectional studies suggests that females with PFP run with greater hip
internal rotation and hip adduction(19, 24, 31). Both motions have been shown in experimental
models to increase the amount of stress on the lateral aspect of the patella, and with repetitive
exposure, may result in pain (11, 14). Rear foot eversion has also been hypothesized to be related to
PFP. Excessive rear foot eversion has been associated with increased knee flexion and a greater
tendency towards knee abduction or genu valgus (16). Increased knee flexion results in greater
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

patellofemoral compressive loads which can increase overall contact stress. Genu valgus is
associated with increased Q angle, increasing the lateral component of the quad force and increasing
the tendency for lateral tracking. This results in greater loads on the lateral aspect of the
patellofemoral joint (29). While many potential mechanisms have been proposed there have to date
been few studies that have assessed the proximal and distal contribution of altered mechanics in
female runners with PFP.
In summary, both hip and foot mechanics have been associated with PFP in retrospective studies.
However, these studies cannot discern between cause and effect. Prospective studies are needed to
help further elucidate biomechanical causes of PFP in runners. In fact, the need for such studies has
been strongly advocated by numerous authors (1, 6, 13). There is growing awareness of the
significant healthcare effects that result from chronic pain conditions such as PFP. Prospective
studies of the underlying mechanics that result in PFP will assist in providing the foundation for
interventions for runners with PFP. Thus, the purpose of this study was to assess the gait mechanics
of female runners who go on to develop PFP compared to a healthy control group who did not
develop any injuries. We hypothesized that female runners who go on to develop PFP would have
greater hip adduction, hip internal rotation, and rearfoot eversion. when compared to a healthy
runners who did not develop PFP.ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

METHODS:
The participants in this study were part of a larger, prospective investigation of lower
extremity injuries in 400 female runners. All participants were between the ages of 18-45, free from
any current injuries, rear foot strikers, and running a minimum of 20 miles a week. Prior to
participation, each subject signed a consent form approved by the University’s Human Subjects
Compliance Committee. Based upon the hip transverse plane data from a previous cross sectional
study an a apriori power analysis was completed with (α=0.05, β= 0.15) a minimum of 13 subjects
was needed for this study (19). Following the initial screening and consent, an instrumented gait
analysis was conducted on all study participants. Anatomical markers were placed over the iliac
crests, greater trochanters, medial and lateral femoral epicondyle, medial and lateral malleoli, first
and fifth metatarsal heads and the front end of the shoes. The first and fifth metatarsal head markers
as well as medial and lateral malleoli were used to define the foot coordinate system. The coordinate
system of the shank was defined from the medial and lateral malleoli markers as well as medial and
lateral femoral epicondyle markers. For the femur’s coordinate system the markers placed on the
medial and lateral femoral condyle, the greater trochanter as well as from a virtual marker which was
determined as 25% of the distance between the trochanters was used. Lastly the pelvis was defined by
the bilateral greater trochanter markers and the markers placed on the iliac crests. Tracking markers
for the pelvis were placed on the space between the 5 th lumbar vertebrae and the sacrum, and the
anterior superior iliac spines. In addition, a molded thermoplastic shell with four markers was
attached to the proximal thigh and distal shank. Three markers were placed on the heel counter of the
shoe, two markers along the vertical bisection of the heel and one on the lateral side of the heel. We
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

have previously shown that the between day reliability as assessed with intraclass correlation
coefficients for the joint angles derived from these markers ranges from fair for hip internal rotation
(0.54-0.58), and rearfoot eversion (0.63-0.71) up to excellent for hip adduction (0.69-0.95) (9, 18).
All participants wore a standard neutral running shoe (Nike, Air Pegasus). Participants then ran along
a 25 meter run way at a speed of 3.7 m/s (± 5%). striking a force plate at its center. Kinematic data
were collected at 120 hz with a 6 camera Vicon 512 motion analysis system (Vicon, Centennial, CO,
USA) and low-pass filtered at 8 Hz with a fourth-order zero lag Butterworth filter. Force data was
sampled at 1080 hz and low-pass filtered at 50 Hz with a fourth-order zero lag Butterworth filter.
Five acceptable trials were collected during the stance phase of running.
Following the biomechanics data collection, a detailed injury history was recorded. For the
next two years, participants reported any running related injuries and their monthly mileage. Only
injuries reported as PFP that were clinically diagnosed by a physician, physical therapist or athletic
trainer were included in the analysis. The diagnosis by the clinician had to include a
determination that the symptoms were related to the patellofemoral joint and not another
structure. Individuals with the diagnosis of patella tendon tendonitis, fat pad syndrome, or
iliotibial band syndrome were excluded from the study. In addition, the PFP group could not have
had a previous episode of PFP. They also had to experience pain for at least 2 months before they
were included in the PFP group. The mechanism of injury had to be related to running, and not
pain do to trauma or that occurred or started in other activities. The control group was age and
mileage matched to the PFP group and consisted of individuals who were free from any previous
episodes of PFP. In addition, those in the PFP group had to be free of any previous history of hip or
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

knee injuries as we did not want to be including mechanics that may have resulted from PFP. The
injured leg of the PFP group was compared to the same limb of the control group.
The joint angles were then calculated using Visual3D software (C-motion, Rockville, MD).
Contact was defined as the point when the vertical ground reaction force exceeded 20 Newtons. Toe
off was defined when the force went below 20 Newtons. Discrete variables were extracted from each
individual trial.
Data were statistically analyzed using SPSS (SPSS inc, Chicago, IL). Independent t-tests
were conducted (alpha 0.05, trend = 0.0.5 <alpha < 0.10) to test the hypotheses. The kinematic
variables of interest were peak rear foot eversion, hip adduction and hip internal rotation. All data
were extracted from the individual trials of time series data. Curves were then time normalized and
averaged across 5 trials per subject and then across the subjects in each group. Therefore, the discrete
values reported may not be reflected in the time normalized and averaged data.
RESULTS:
Of the 400 runners followed, 38 reported anterior knee pain. Of these, 34 cases were running-related
with 15 being medically diagnosed and included in the data analysis. The PFP group and control
group were equally matched for age (27 sd 10 years vs, 27 sd 10 years) and monthly mileage (165 sd
53 km vs, 165 sd 43 km). The kinematic curves of the variables of interest are presented in Figure 1.
We found that the PFP group had a significantly greater hip adduction angle (p=0.007). No
significant differences were found though in rear foot eversion (p=0.10) (Table 1). The PFP group
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

did have more hip adduction and less rear foot eversion throughout the entire stance period (Figure
1). While the PFP group landed in more hip internal rotation, this difference was non-significant
(p=0.47) (Figure 1).
DISCUSSION:
The purpose of this study was to assess the lower extremity mechanics in runners who go on to
develop PFP. We found that runners who went onto develop PFP exhibited some of the same
mechanics that have been noted in retrospective studies (19, 31). This included a significantly greater
hip adduction angle. We did not find any differences in the hip internal rotation or rearfoot eversion
angle. These results provide the first prospective evidence on the role of gait mechanics in female
runners who develop PFP.
The finding of significantly greater hip adduction in the PFP group further supports that of
other cross sectional studies (19, 31). Increased hip adduction has been shown to concentrate the
contact stress on the lateral aspect of the patella (11). Contract stress on the patella has also recently
been shown to be greater in patients with PFP (8). While the patellar cartilage is aneural, such
repetitive stress can irritate the subchondral bone, which is innervated, and result in pain (10, 21). To
reduce load on the hip abductor muscles as the result of greater hip adduction angle the participants
with PFP may have potentially used compensatory trunk mechanics which may alter the center of
mass and ultimately the loads on the knee (21). In fact, a recent study reported that female runners
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

with PFP exhibited a compensatory ipsilateral trunk lean (19). The inclusion of trunk mechanics may
have lent additional insight on the findings of the current study.
Increased femoral rotation has also been shown to increase contact stresses on the lateral facet
of the patella (14). However, the transverse plane findings were not as compelling as those in the
frontal plane. While the PFP group landed with more hip internal rotation on average, this difference
was not statistically significant. There has been some disagreement in the literature regarding hip
rotation in runners with PFP (12,14, 28). This may be due to differences in methods, marker sets and
populations. However, the transverse plane has generally been noted to be sensitive to errors and
tends to be most variable of all planes of motion (22). This increased variability makes it difficult to
detect differences between groups.
We hypothesized that rearfoot eversion would be increased in the PFP group as it has been
associated with genu valgus which can result in misalignment between the patella and the femur,
increasing contact stress (16). It is possible that this was a compensatory mechanism to counter the
medial collapse of the lower extremity associated with increased hip adduction. Interestingly, while
there are many references to the relationship between foot pronation and PFP, there is very little
evidence of this in the literature (1). One recent study found an increase in rear foot motion in a
group of runners with PFP (19). The 2 degree increase was associated with a moderate effect size,
but was not significant. Most studies of foot mechanics have focused on the rear foot. However,
Lundberg et al noted that majority of rear foot eversion occurs at the mid-foot (15). In fact, these
authors note that there is twice as much talonavicular eversion than subtalar eversion (15).
Unfortunately, the difficulty in accurately measuring mid-foot motion has precluded its study in
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

relation to PFP. It is interesting to note that foot orthotic devices, designed to minimize pronation,
have been effective in reducing pain in patients with PFP (21). It is entirely possible that they are
having their greatest effect at the mid-foot through their support of the arch. The development of
dynamic imaging techniques, such as biplane fluoroscopy, where joint motions between individual
bones can be assessed, will help to advance our knowledge in this area. The results are also
surprising in light of the studies that have reported significant pain reduction with foot orthotic
devices designed to reduce foot pronation (5, 26).
Based upon the findings of this study, it appears that the largest and most consistent
differences between those who go on to develop PFP and those who do not are in hip adduction.
While we did not assess hip strength in these individuals, weakness of the hip abductors is often
associated with increased hip adduction and PFP (12). However, recent studies have suggested that
strengthening the hip muscles does not lead to improvements in hip mechanics during running (23,
32). However, neuromuscular re-education through gait retraining has been successfully to alter
faulty hip mechanics during running (27). Additionally improvements in pain and function were
reported in these patients PFP, many who have not responded to standard physical therapy (20).
More importantly, these improvements have persisted beyond the intervention, suggesting the
underlying cause was addressed. This current study further highlights the role of increased hip
adduction in the development of PFP.
The current study provides the first prospective evidence of a hip etiology in female runners
who go onto develop PFP. The need for prospective studies assessing gait mechanics in patients with
PFP was advocated in a systematic review of biomechanical risk factors for PFP (2). Additionally,
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

this need was highlighted within the published expert consensus statement from the international PFP
conference (1, 6). These prospective data agree with the findings of cross sectional studies, which
also found greater hip adduction (19, 31) in runners with PFP. Similar agreement between
retrospective and prospective data on running mechanics of individuals with iliotibial band syndrome
has been reported (31,32). These results together begin to infer that the mechanics seen following
recovery of an injury are consistent with those seen prior to the injury. While prospective studies are
the gold standard for defining causal relationships, they are costly and difficult to conduct. This
suggests that retrospective studies of mechanics associated with running could be informative of the
cause of the injury.
The study, while compelling, is not without limitations. Our subject numbers were limited by
our purposeful strict inclusion criteria. We only included runners who initially had no history of PFP,
as we did not want a prior injury to possibly influence baseline mechanics. Additionally, we only
included runners whose PFP was diagnosed by a medical professional. This helped to assure this was
a significant problem and helped to increase the validity of the diagnosis. These runners were also
very well matched with the controls in terms of age, as well as mileage run. Because the sample size
estimation was based off of potential differences in hip mechanics we may have been limited in
our ability to detect differences in rearfoot mechanics. Also the use of the greater trochanter
markers to help define the hip joint centers may have resulted in a less accurate positioning of
the hip joint coordinate system and thus increased the variability of the joint angles
particularly in the transverse plane. By comparison a recent cross sectional study using
functional hip joint centers and a different kinematic model was able to show a significant
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

difference in transverse plane mechanics between those with and without PFP (19).
Collectively though these studies do indicate that hip mechanics whether they be in the frontal
or transverse plane are altered in female runners with PFP.
In conclusion, the results from the study provide the first prospective evidence of a hip
etiology in females who go onto develop PFP. These results suggest that injury prevention and
rehabilitation programs should address abnormal hip mechanics to prevent the development and/or
recurrence of PFP.
Conflict of interest: The authors have no conflict of interest to report. The results of the present
study do not constitute endorsement by ACSM.
Acknowledgements: This study was funded by a Dept of Defense grant DAMD17-00-1-0
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

REFERENCES:
1. Barton CJ, Levinger P, Menz HB, and Webster KE. Kinematic gait characteristics associated with
patellofemoral pain syndrome: A systematic review. Gait & Posture. 2009;30(4):405-16.
2. Blair SN, Sallis RE, Hutber A, and Archer E. Exercise therapy – the public health message. Scandinavian
Journal of Medicine & Science in Sports. In press.
3. Blond L, and Hansen L. Patellofemoral pain syndrome in athletes: a 5.7-year retrospective follow-up
study of 250 athletes. Acta Orthop Belg. 1998;64(4):393-400.
4. Boling M, Padua D, Marshall S, Guskiewicz K, Pyne S, and Beutler A. Gender differences in the incidence
and prevalence of patellofemoral pain syndrome. Scand J Med Sci Sports. 2009:725-30.
5. Collins N, Crossley K, Beller E, Darnell R, McPoil T, and Vicenzino B. Foot orthoses and physiotherapy in
the treatment of patellofemoral pain syndrome: randomised clinical trial. BMJ. 2008;337:a1735.
6. Davis IS, and Powers CM. Patellofemoral pain syndrome: proximal, distal, and local factors, an
international retreat, April 30-May 2, 2009, Fells Point, Baltimore, MD. J Orthop Sports Phys Ther.
2010;40(3):A1-16.
7. Devereaux MD, and Lachmann SM. Patello-femoral arthralgia in athletes attending a Sports Injury Clinic.
Br J Sports Med. 1984;18(1):18-21.
8. Farrokhi S, Keyak JH, and Powers CM. Individuals with Patellofemoral Pain Exhibit Greater
Patellofemoral Joint Stress: A Finite Element Analysis Study. Osteoarthritis and Cartilage. In Press.
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

9. Ferber R, Davis IM, Williams DS, and Laughton C. A comparison of within- and between-day reliability of
discrete 3D lower extremity variables in runners. Journal of Orthopaedic Research. 2002;20(6):1139-45.
10. Goodfellow J, Hungerford DS, and Woods C. Patello-femoral joint mechanics and pathology. 2.
Chondromalacia patellae. J Bone Joint Surg Br. 1976;58(3):291-9.
11. Huberti HH, and Hayes WC. Patellofemoral contact pressures. The influence of q-angle and
tendofemoral contact. J Bone Joint Surg Am. 1984;66(5):715-24.
12. Ireland ML, Willson JD, Ballantyne BT, and Davis IM. Hip strength in females with and without
patellofemoral pain. J Orthop Sports Phys Ther. 2003;33(11):671-6.
13. Lankhorst NE, Bierma-Zeinstra SM, and van Middelkoop M. Risk factors for patellofemoral pain
syndrome: a systematic review. J Orthop Sports Phys Ther. 2012;42(2):81-94.
14. Li G, DeFrate LE, Zayontz S, Park SE, and Gill TJ. The effect of tibiofemoral joint kinematics on
patellofemoral contact pressures under simulated muscle loads. J Orthop Res. 2004;22(4):801-6.
15. Lundberg A, Svensson OK, Bylund C, Goldie I, and Selvik G. Kinematics of the ankle/foot complex--Part 2:
Pronation and supination. Foot Ankle. 1989;9(5):248-53.
16. McClay I, and Manal K. A comparison of three-dimensional lower extremity kinematics during running
between excessive pronators and normals. Clin Biomech (Bristol, Avon). 1998;13(3):195-203.
17. Nimon G, Murray D, Sandow M, and Goodfellow J. Natural history of anterior knee pain: a 14- to 20-year
follow-up of nonoperative management. J Pediatr Orthop. 1998;18(1):118-22.
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

18. Noehren B, Manal, K., Davis, I.,. Improving between-day kinematic reliability using a marker placement
device Journal of Orthopaedic Research. 2010;28:1405-10.
19. Noehren B, Pohl MB, Sanchez Z, Cunningham T, and Lattermann C. Proximal and distal kinematics in
female runners with patellofemoral pain. Clin Biomech (Bristol, Avon). 2012;27(4):366-71.
20. Noehren B, Scholz J, and Davis I. The effect of real-time gait retraining on hip kinematics, pain and
function in subjects with patellofemoral pain syndrome. British Journal of Sports Medicine.
2011;45(9):691-6.
21. Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J
Orthop Sports Phys Ther. 2010;40(2):42-51.
22. Ramsey DK, and Wretenberg PF. Biomechanics of the knee: methodological considerations in the in vivo
kinematic analysis of the tibiofemoral and patellofemoral joint. Clin Biomech (Bristol, Avon).
1999;14(9):595-611.
23. Snyder KR, Earl JE, O'Connor KM, and Ebersole KT. Resistance training is accompanied by increases in hip
strength and changes in lower extremity biomechanics during running. Clin Biomech (Bristol, Avon).
2009;24(1):26-34.
24. Souza RB, and Powers CM. Differences in hip kinematics, muscle strength, and muscle activation
between subjects with and without patellofemoral pain. Journal Orthopedics Sports Physical Therapy.
2009;39(1):12-9.
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

25. Stathopulu E, and Baildam E. Anterior knee pain: a long-term follow-up. Rheumatology (Oxford).
2003;42(2):380-2.
26. Swart NM, van Linschoten R, Bierma-Zeinstra SMA, and van Middelkoop M. The additional effect of
orthotic devices on exercise therapy for patients with patellofemoral pain syndrome: a systematic
review. British Journal of Sports Medicine. In press.
27. Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, and Zumbo BD. A retrospective case-
control analysis of 2002 running injuries. Br J Sports Med. 2002;36(2):95-101.
28. Thijs Y, Van Tiggelen D, Roosen P, De Clercq D, and Witvrouw E. A prospective study on gait-related
intrinsic risk factors for patellofemoral pain. Clin J Sport Med. 2007;17(6):437-45.
29. Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical
model. J Orthop Sports Phys Ther. 1987;9(4):160-5.
30. Utting MR, Davies G, and Newman JH. Is anterior knee pain a predisposing factor to patellofemoral
osteoarthritis? Knee. 2005;12(5):362-5.
31. Willson JD, and Davis IS. Lower extremity mechanics of females with and without patellofemoral pain
across activities with progressively greater task demands. Clin Biomech (Bristol, Avon). 2008;23(2):203-
11.
32. Willy RW, and Davis IS. The effect of a hip-strengthening program on mechanics during running and
during a single-leg squat. J Orthop Sports Phys Ther. 2011;41(9):625-32.
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

FIGURE LEGEND
Figure 1: Ensemble curves for the PFP (dotted line) and control group (solid line) for a) hip
adduction angle, b) hip internal rotation angle, and c) rearfoot eversion. Hip adduction, hip internal
rotation angle, and rearfoot eversion angle are positive. Error bars represent half a standard deviation.
A B
C
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
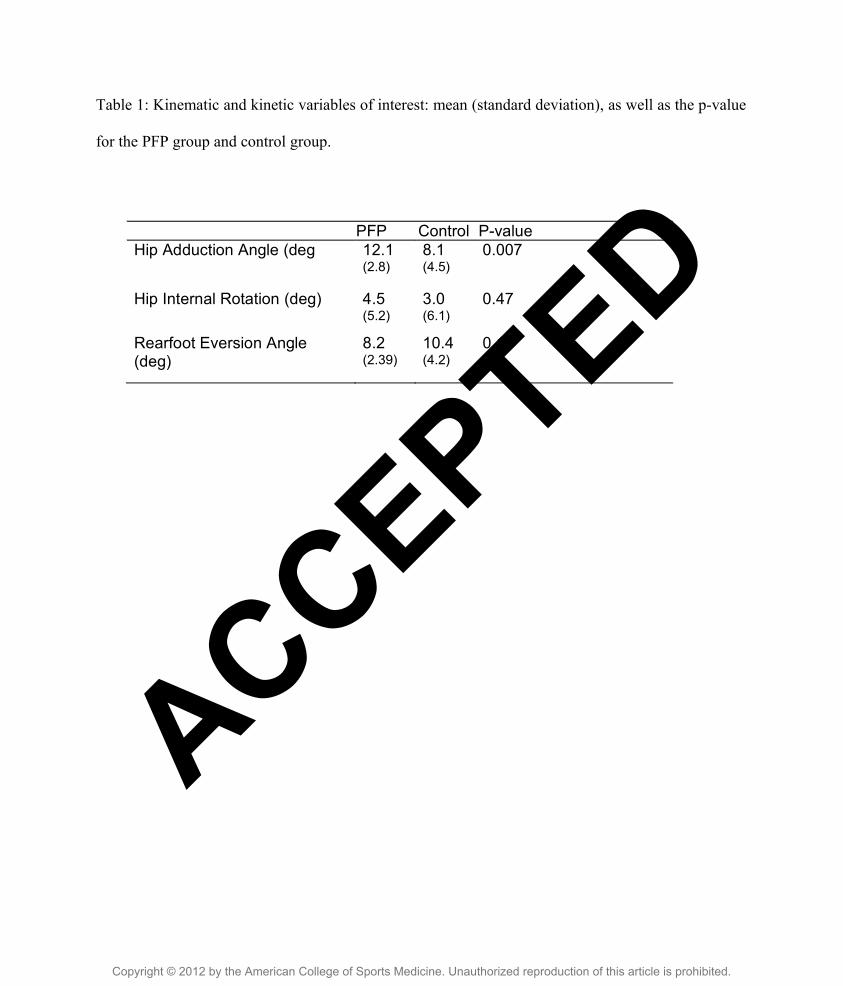
Table 1: Kinematic and kinetic variables of interest: mean (standard deviation), as well as the p-value
for the PFP group and control group.
PFP Control P-value Hip Adduction Angle (deg 12.1
(2.8)
8.1 (4.5)
0.007
Hip Internal Rotation (deg) 4.5 (5.2)
3.0 (6.1)
0.47
Rearfoot Eversion Angle (deg)
8.2 (2.39)
10.4 (4.2)
0.1
ACCEPTED
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.






