
€¦ · Web viewChildren and Young People's Voice Project, Children with Disabilities, Jigsaw,...
48
Consultation on Quality Improvement Priorities 2014/15 Report January - February 2014
Transcript of €¦ · Web viewChildren and Young People's Voice Project, Children with Disabilities, Jigsaw,...

Consultation on Quality Improvement Priorities 2014/15ReportJanuary - February 2014

Consultation on Quality Improvement Priorities 2014-15
Staffordshire and Stoke on Trent Partnership Trust Consultation on Quality Improvement Priorities 2014-15 report January - February 2014Robin Sasaru, Quality Team ManagerChris McKeown, Effectiveness Officer
ContentsAim.......................................................................................................................................2
The consultation...................................................................................................................3
General comments received for each strategy.....................................................................6
Priority 1: Safety – Reducing Avoidable Pressure Ulcers.....................................................8
Consultation measures and questions..............................................................................8
Responses........................................................................................................................8
Priority 2: Experience – Customer Satisfaction..................................................................14
Consultation measures and questions............................................................................14
Consultation responses..................................................................................................15
Priority 3: Effectiveness – Improving Outcomes.................................................................21
Consultation measures and questions............................................................................21
Consultation comments...................................................................................................22
Priority 4: Effectiveness – Supporting Independence by Personalised Care......................27
Consultation measures and questions............................................................................27
Consultation comments...................................................................................................28
Priority 5: Safety – Workforce.............................................................................................32
Consultation measures and questions............................................................................32
Consultation comments...................................................................................................33
AimThe aim of this report is to
log all comments received during the consultation for the Quality Improvement Priorities 2014-15
highlight the Trust response to all comments received
Page 2 of 32

Consultation on Quality Improvement Priorities 2014-15
The consultationThe consultation ran from 20 January to 20 February 2014, and made use of the following mechanisms to disseminate and gain comment on the Quality Improvement Priorities 2014-15 consultation report:
Emailing stakeholders and inviting them to comment and forward the documents to their colleagues
Holding consultation sessions that included Partnership Trust staff, Clinical Commissioning Group leads, partner agencies and Trust members
Posting the consultation documents on the Trust internet site.
The substance of each consultation response is copied into this report, correcting for spelling where appropriate.
Names of respondents are not included, although comments have not been altered to strictly preserve anonymity unless explicitly requested.
Comments were aligned with the closest matching consultation question where possible.
Where possible all comments were incorporated into the final version. Table 1 logs the individuals and groups that were contacted for the consultation. In addition to the consultation comments, the Quality team made additional amendments to the draft to refine the measures and objectives, and check for consistency, readability and grammar.
We thank everyone who commented on these priorities. We appreciate the many insightful comments received that have strengthened our approach to quality improvement.
Page 3 of 32

Consultation on Quality Improvement Priorities 2014-15
Table 1: Consultation summaryCohort Who was contactedStaff, committees and groups
Effectiveness GroupEMTArticles in “the word” and Trust internet site via communicationsChief Operating OfficersProfessional LeadsQuality TeamEquality & Inclusion ManagerEngagement & Membership ManagerTrust Members
Service user representatives
Community Health Voice, HealthWatch Stoke, HealthWatch Staffordshire
Partner organisations
Keele UniversityStaffordshire UniversityShropshire and Staffordshire Area TeamSouth Staffordshire and Shropshire Healthcare NHS Foundation TrustBurton Hospitals NHS Foundation TrustMid Staffordshire NHS Foundation TrustNorth Staffordshire Combined Healthcare NHS TrustUniversity Hospital of North StaffordshireWest Midlands Ambulance ServiceAge UK (South Staffs), Chase Council for Voluntary Service, Lichfield & District Community and Voluntary Sector Support, Tamworth Centre for Voluntary Service, The Community Council of Staffordshire, South Staffordshire Community and Voluntary Action, Newcastle under Lyme Community and Voluntary Support, Staffordshire Moorlands Community and Voluntary Services, Voluntary Action Stoke on Trent (VAST), East Staffordshire Community and Voluntary Service, Lichfield and District CVS, Newcastle 50+ Forum, DEAF Vibe,Children and Young People's Voice Project, Children with Disabilities, Jigsaw, Staffordshire Fire and Rescue, Staffordshire Girl Guiding, Staffordshire Police 100 Club/Citizens Panel, Staffordshire Thru Care, Staffordshire UK Youth Parliament, Staffordshire Youth Action Kouncil (YAK), Staffordshire Youth Offending Service, Staffordshire Council for Youth Voluntary Services, North Staffs Young Carers, Newcastle Young People's Association (NYPA), Youth of the Moorlands Action Council (YOMAC), Rona Borland, Tamworth Early Years, West Midlands Consortium of Travellers, East Staffs District Forum, South Staffordshire District Youth Council (DYC), Stafford and Stone District Youth Forum, Tamworth District Youth Forum (TDYF), VOICE (Cannock Chase District Youth Forum), Young People Today (Lichfield District Youth Forum), Children & Young People (CYP) Partnership
Page 4 of 32

Consultation on Quality Improvement Priorities 2014-15
Cohort Who was contactedWerrington Patient Participation GroupStafford and Surrounds PPGKingsbridge Medical Practice PPGEast Staffordshire PPGsTrent Meadows PPGWeeping Cross PPGThe Donna Louise Children's Hospice TrustSt Giles HospiceKatharine House HospiceDouglas Macmillan HospiceHMP StaffordHMYOI BrinsfordHMYOI Swinfen HallHMP FeatherstoneHMYOI Werrington
Commissioning Stafford and Surrounds Clinical Commissioning GroupNorth Staffordshire Clinical Commissioning GroupStoke on Trent Clinical Commissioning GroupEast Staffordshire Clinical Commissioning GroupNHS South East Staffs and Seisdon & Peninsula Clinical Commissioning GroupCannock Chase Clinical Commissioning GroupLeicester City Clinical Commissioning GroupStaffordshire CouncilStoke on Trent City Council
Page 5 of 32

Consultation on Quality Improvement Priorities 2014-15
General comments receivedComments Response
All priorities link together and need to. A prologue is needed to say how they all are measured together/ against each other
As last year, our Quality Account 2013/14 will have information on how we decided our quality priorities, and this section will show how they link together.
Need to consult with patient groups alone – freedom to speak openly – current meeting imbalanced? May be different comments – staff, patients, commissioners.
We recognise the need to fully engage with service users, maximising their opportunities for involvement.
Further work will be undertaken to increase service user involvement in future consultations.
How are you going to address improving services for people with mental health conditions? – How are these priorities going to evidence this? – This is stated in the document.
Although this is an important area, we did not consider this to be one of our 5 quality improvement priorities for the Trust this year.
Nothing to object wouldn’t disagree with priorities BUT may be some gaps? Complaints (see notes)
(See the section on complaints)
Issue with ambulance service – arriving in time, early and late
This comment related to services that we do not provide.
Partnership working – whole patient journey. Transition.
Our focus on outcomes and personalisation will assist us in improving our services across the whole patient journey.
[Business Development Priorities] The Staffordshire Neurological Alliance would support all these as they were all shown to be improvement opportunities following our Quality Neurology audit in 2010.Particularly better post diagnostic counselling and psychological services are important in reducing excess morbidity in people with chronic neurological disorders
This comment related to services that we do not provide.
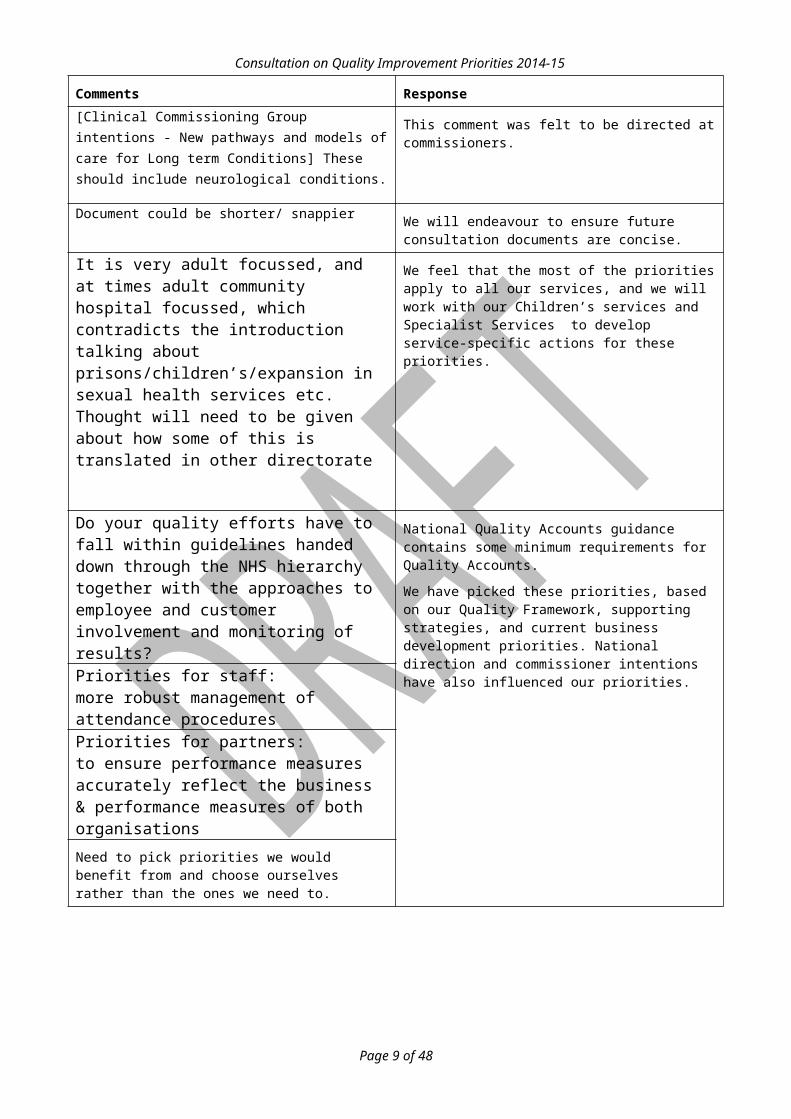
[Clinical Commissioning Group intentions - New pathways and models of care for Long term Conditions] These should include neurological conditions.
This comment was felt to be directed at commissioners.
Document could be shorter/ snappier We will endeavour to ensure future consultation documents are concise.
It is very adult focussed, and at times adult community hospital focussed, which contradicts the introduction talking about prisons/children’s/expansion in sexual health services etc. Thought will need to be given about how some of this is translated in other directorate
We feel that the most of the priorities apply to all our services, and we will work with our Children’s services and Specialist Services to develop service-specific actions for these priorities.
Page 6 of 32

Consultation on Quality Improvement Priorities 2014-15
Comments ResponseDo your quality efforts have to fall within guidelines handed down through the NHS hierarchy together with the approaches to employee and customer involvement and monitoring of results?
National Quality Accounts guidance contains some minimum requirements for Quality Accounts.
We have picked these priorities, based on our Quality Framework, supporting strategies, and current business development priorities. National direction and commissioner intentions have also influenced our priorities.
Priorities for staff:more robust management of attendance proceduresPriorities for partners:to ensure performance measures accurately reflect the business & performance measures of both organisationsNeed to pick priorities we would benefit from and choose ourselves rather than the ones we need to.
Page 7 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority 1: Safety – Reducing Avoidable Pressure UlcersConsultation measures and questions
Proposed measures for 2014/15 Proposed 2014/15 target
1A Number of pressure ulcers reported as grade 3 and 4 pressure ulcers and reported as serious incidents
Aim for Zero grade 2/3/4 avoidable pressure ulcers developed in our care1
1B Number of pressure ulcers reported as avoidable grade 3 / 4 pressure ulcers developed in our care and reported in our care and reported as serious incidents.
Zero grade 2/3/4 avoidable pressure ulcers developed in our care2
1C All pressure ulcers for people in our care and reported as adverse incident
Increase in number of incidents reported and reduction in the proportion of serious incidents / all reported incidents
Other measures we will use for Safety
1D Total number of adverse incidents reported (all incidents)
Quarterly increase in number of incidents reported
1E Percentage of reported incidents classified as serious incidents
Quarterly reduction in proportion of serious incidents / all reported incidents
Q1.1: Is the measure for ‘pressure ulcers reported as adverse incidents’ already covered by the more general measure ‘total number of adverse incidents reported’?
Q1.2: Do you agree with the minor changes made to the Quality Improvement Priority around Safety?
Q1.3: Should we include other measures? Should we delete any measures that are no longer appropriate?
1 Specific trajectory to be determined2 Specific trajectory to be determined
Page 8 of 32
Consultation on Quality Improvement Priorities 2014-15
Responses
Priority Comments Response
1 Medication error reporting – harm decreases.
The overall measures around numbers of incidents reported will also capture medication errors. Medication error information will be reviewed by our Medicines Management Committee.1 Consider adding medication errors,
reporting and levels of harm – In Clinical Commissioning Group planning guidance.
1 Should be measuring on outcomes not processes and be accountable for the measures.
We agree. A Grade 3/4 avoidable pressure ulcer developed in our care is a reflection of failure in our services. The number of adverse incidents reported is used as a measure of our safety culture.
1 “Eliminate” is the key word and needs to be worded to highlight this
We have changed the wording of the aim to “eliminate avoidable grade 3/4 pressure ulcers”
1 This is how we did against previous year – count as a reduction so would naturally expect this year’s result to [be less].
We will continue with our aim of eliminating avoidable pressure ulcers, and agree a tolerance as for 2013/14.
Our Quality Account will outline our progress in reducing avoidable pressure ulcers.
1 Use prologue to sell yourself.
Transparency is the focus at the minute.
Our Quality Account will openly and transparently show our progress against our priorities.
1 Achieve numbers and shows numbers but so what? What does this mean for pressure ulcers?
We feel that reducing avoidable pressure ulcers reflects an approach to care that is safety focussed, demonstrates that we implement learning and reflect on our practice.
1 Is it fair? Is everybody recording the same way? Inclusion of avoidable but not attributable has been included now but what teams know about this?
Our Tissue Viability Panel scrutinise all grade 3/4 pressure ulcers developed in our care, to ensure consistency of reporting. Feedback to teams is via our Safety and Effectiveness Operational Groups and all-staff communications, including our internal newsletter, “Quality Matters”.
We directly notify the team involved if we find an avoidable pressure ulcer developed in their care.
1 NICE guidelines on Pressure Ulcers in April 2014 due - what changes will need to be made as a consequence of this.
We have reviewed the draft guidance on prevention and management of pressure ulcers and sent our comments to NICE for consideration.
We do not feel that the guidance will change our overall aim to eliminate avoidable pressure ulcers.
1 Intravenous fluid therapy? Risk of administration, has this been addressed? NICE could provide more details [if] wanted.
There are important safety considerations around the use of Intravenous fluid therapy,
On consideration, this was not deemed as one of our top five improvement priorities for 2014/15.
Page 9 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
1 Order of proposed measures should be changed 1C, 1A, then 1B.
1C should be first
We have changed the order of the measures accordingly.
1A What is avoidable/ unavoidable? We adhere to national definitions for avoidable / non-avoidable pressure ulcers as set out at www.patientsafetyfirst.nhs.uk 3
1A Stronger prevention. We have changed the wording of the aim to “eliminate avoidable grade 3/4 pressure ulcers”
We have a Zero-tolerance action plan for eliminating pressure ulcers, which we will refresh for 2014/15.
1A Feeding back to source of lesion. We provide feedback to teams and partner agencies as part of our incident reporting system.
We also work closely with our partner agencies, including University Hospital NHS Trust (North Staffordshire) to monitor care of patients with pressure ulcers, using our incident reporting system. We also use the TRAC (Track Report Analyse Communicate) system to monitor pressure ulcers across our health economy.
1 How is learning from Root Cause Analyses and Tissue Viability panel changing practice? We really need to link priorities to demonstrate partnership working across same journey. Link to wider health economy. Need to be explicit about deterioration of pressure ulcers.
The learning from our Tissue Viability panels feeds into our Safety and Effectiveness Operational Groups, and is disseminated via our internal newsletter, “Quality Matters”.
We will report learning and improvements for 2013/14 in our Quality Account.
1B Are figures of Pressure Ulcers only taken from incident reporting?
Our incident reporting system is our primary record of pressure ulcers.
We also use the NHS safety thermometer to measure the prevalence of existing pressure ulcers.
Q1.1 Requires consistency around grading of pressure ulcers – especially grade 2. Depends to some degree on patient/ service user compliance.
We provide ongoing training for our staff on Pressure Ulcer identification, reporting and management.
As for all incidents, we are looking to see increased reporting for lower grade pressure ulcers, which demonstrates that our staff are providing safer care.
Q1.1 Keep in as grade 2 being removed want to keep focus on Pressure Ulcer reporting.
We feel that the reporting of grade 1/2 Pressure Ulcers is as equally important, as a reflection of our care.
We want the number of grade 1/2 pressure ulcers reported to increase, as our staff’s knowledge and awareness of pressure ulcer care increases, and they work to prevent these progressing to more serious Pressure Ulcers.
Q1.2 Yes
3 See http://www.patientsafetyfirst.nhs.uk/ashx/Asset.ashx?path=/PressureUlcers/Defining%20avoidable%20and%20unavoidable%20pressure%20ulcers.pdf
Page 10 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
We are concerned with eliminating all avoidable pressure ulcers developed in our care.
We want the number of grade 1/2 pressure ulcers reported to increase, as our staff’s knowledge and awareness of pressure ulcer care increases, and they work to prevent these progressing to a more serious Pressure Ulcer.
We will continue to capture data via our incident reporting system for grade 2 pressure ulcers, and act to prevent these becoming more serious. Techniques such as root cause analysis can help us to achieve this.
Grade 2 pressure ulcers show as relatively superficial damage to the skin and can happen very quickly even when care is in place. We want the number of grade 1/2 pressure ulcers reported to increase, as our staff’s knowledge and awareness of pressure ulcer care increases, and they work to prevent these progressing to more serious Pressure Ulcers.
Q1.2 Providing reporting of 2 and 3’s is consistent.
Q1.2 Yes but grade 2 pressure ulcers increase if grade 3 and 4 are reduced. If not including grade 2 we need to be more explicit about them.
Q1.2 Why have we excluded grade 2’s? Because it isn’t achievable? What are our aims for grade 2’s?
Q1.3 Community and hospitals should be separated- community can’t eliminate can only reduce. Need to be more explicit about community point of view.
We feel that a goal of eliminating avoidable pressure ulcers developed in our care should apply to our hospital and community services, and we recognise that eliminating avoidable pressure ulcers in the community is a more challenging ambition.
Our Quality Account will provide information about avoidable pressure ulcers in hospital services and in the community.
Q1.3 Could the organisation be more transparent about Pressure Ulcers in particular these that are attributable to the organisation and to other organisations/
We regularly report this through our governance structures. The measures include avoidable grade 3/4 pressure ulcers developed in our care.
Q1.3 Need to be aware of issues regarding obtaining pressure relieving equipment in community and hospitals. – Consistent across the trust
We agree.
Q1.3 Issues around workforce capacity regarding review of individuals and equipment provided.
We feel that our processes of care are also an important factor in improving quality, as well as ensuring adequate workforce capacity.
Q1.3 Measures to demonstrate we are treating them well – time to heal.
The focus of this measure is around safe processes of care that mean our service users do not suffer from avoidable grade 3/4 pressure ulcers.
We are continually improving the effectiveness of our pressure ulcer care (and other types of skin care). Our Tissue Viability service has produced papers on the effectiveness of therapeutic devices.
Page 11 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
1B Acquired in care is more difficult in community settings when patients may not be compliant with advice – or would this be then deemed ‘unavoidable’
We adhere to national definitions for avoidable / non-avoidable pressure ulcers as set out at www.patientsafetyfirst.nhs.uk 4
According to this definition, if “the individual person refused to adhere to prevention strategies in spite of education of the consequences of non-adherence” this would not be an avoidable pressure ulcer.
We recognise the increased challenges of eliminating avoidable pressure ulcers in the community.
1C If we are reducing pressure ulcers then there will be a reduction in reporting I would have thought?
A reduction in reporting of grade 3/4 pressure ulcers must be in the context of an overall increase in incident reporting – this demonstrates that an organisational safety culture is in place.
An increase in the number of reported grade 1/2 pressure ulcers should demonstrate that our staff are more proactive in providing high quality care of pressure ulcers.
Q1.1 Not if we want to reduce total pressure ulcers as that will presumably reduce reporting of these kinds of incidents as they will no longer occur.
Q1.1 Is number of incidents as important in demonstrating that we do something about those that are reported? Should there be a measure around action plans in place for SUIs?
It is important that we have robust systems for acting on incidents, including the development of action plans. However, we do not feel that measuring the number of action plans in place in itself will correlate with improvement in quality.
We feel that a grade ¾ avoidable pressure ulcer developed in our care is a reflection of failure in our services.
On reviewing the comments we decided to make the following amendments to the Safety priority:
Focus the reporting on grade 3/4 avoidable pressure ulcers developed in our care, which is a clearer single indicator of the safety of our care than the three previous overlapping measures.
We will continue to measure the total number of adverse incidents reports, and percentage of reported incidents classified as serious incidents, applicable to the Partnership Trust, which is in line with our current reporting to the Trust Board.
4 See http://www.patientsafetyfirst.nhs.uk/ashx/Asset.ashx?path=/PressureUlcers/Defining%20avoidable%20and%20unavoidable%20pressure%20ulcers.pdf
Page 12 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority 2: Experience – Customer SatisfactionConsultation measures and questions
Proposed measures for 2014/15 Proposed 2014/15 target
2A Friends and family test (Net Promoter Score)
Achieve and sustain +70 for all services
2B Health and social care compliments received by the Partnership Trust
Year on year increase in the number of compliments received
2C Percentage of complaints acknowledged within three working days
100% (health)
100% (social care)5
2D Percentage of complaints responded to within complaints NHS regulations timescales
100%
2E Patient Experience Surveys within Health and Social Care
At least 1000 responses each month from surveys in Health and at least 98 responses each month from surveys in social care for Integrated Health and Social Care Teams.
2F Implementation of comment cards for community services where service users don’t wish to use technological solutions
Comment cards available in all places where care is delivered
2G Number of complaints that were not responded to within 60 days
0
2H Percentage of complaints that are reviewed by our complaints panel
All high risk complaints
5% of all other complaints6
Q2.1: Do you agree with the changes made to the Quality Improvement Priority around Experience?
Q2.2 Rather than just report an overall friends and family score, should we also report by division? Should we also set a target for each division?
Q2.3: Should we include other measures? Should we delete any measures that are no longer appropriate?
5 Separated reporting for Health and Social care complaint due to differing systems and responsibilities for social care complaints.6 Target to be confirmed with complaints panel
Page 13 of 32

Consultation on Quality Improvement Priorities 2014-15
Consultation responsesPriority Comments Response
2 May be some gaps – how do we ensure that patients / service users know who to talk to when raising issues? – in particular when services are provided by different organisations. – is there a clear complaints system? – How do we ensure that organisations separate process collaborate?
Our complaints and PALS teams are publicised across the Trust and help service users to make complaints when these cross over organisational boundaries.
The Trust is subscribed as an active partner within the Health Economy Multi-Agency Protocol for complaints. Within this process complaints are case managed through a collaborative investigation and response by the nominated Lead Provider for the health economy complaint.
2 All about scores! Needs to be qualitative not just quantitative. Writing baseline data but so what? Needs to be written differently
Our Quality Account also provides qualitative information on service user experience, including complaint themes and trends.
2 Set Measures on outcomes – Be more patient explicit and treat patient not just the condition – patient feedback you said, we did. Staff feedback should then link to patient feedback to give a clearer picture.
We have “you said we did” display boards along with feedback for each teams net promoter score for public facing areas as part of our Experience strategy.
We will look to develop our staff Net Promoter Score in 2014/15 and link this information to service user feedback.
2 How can you capture results when providers collect the data in different ways?
Our experience team has been developing consistent methods for gaining service user feedback across all Trust services, and will continue this work in 2014/15.
The Trust does provide monthly reporting in accordance to the national reporting of the Health and Social Care Complaints Regulations.
2 Would like to know how many people we have surveyed vs population.
Working out a “population” figure for our variety of services may be problematic, and would not necessarily be comparable across our range of services.
We do not feel that a sample vs population calculation would add significant value to this quality improvement measure. However, each community team has a set monthly sample target.
2 Define a complaint. We adhere to national guidance on definitions of complaints, and we also report on PALs concerns which are resolved in 24 hours.
2 Need to ensure that the method of collection is robust – eg when you ask the question during intervention
Our experience team has been developing consistent methods for gaining service user feedback across all Trust services, and will continue work to ensure our methods are robust in 2014/15.
2 Need to be open about data – in particular broken down by service.
We will show our experience and complaints data by Division in our Quality Account.
2 Need to ensure the voice is heard rather that focus just on complaints.
We provide monthly Experience data on PALs concerns, Complaints, Comments and the User and Carer experience of our services to our Trust Board and Operational Groups.
Page 14 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
2A Friends and Family Test- more than score feedback follow on comments and actions
Each team receives monthly feedback on their Friends and Family test score along with user and carer’s feedback for improvement. We will report on highlights of actions taken as a result of service user feedback in our Quality Account.
We do not feel that measuring the number or completion of actions in itself will correlate with improvement in quality.
2A Needs more appropriate phrasing of the [question]
The Friends and Family Test is a national mandatory requirement for all NHS Providers. The question can now be framed for services or operational teams in accordance to the national parameters.
2A What does +70 mean to the layperson? As with previous Quality Accounts, we will provide a brief explanation of the Net Promoter Score calculation in the account.
2A Is this accurate? Eli-lite breakdown and ability to use. Challenge of non-English speaker to complete.
Our Experience Team will work to increase the availability of non-English survey tools and report on this in our Quality Account 2014/15
2A Is F&F test reported / displayed at each service? Meaning of this score displayed?
Each team receives monthly feedback on their Friends and Family Test score. We will report on highlights of actions taken as a result of service user feedback in our Quality Account.
We display “you said we did” boards along with feedback for each individual team. The net promoter score is displayed in public facing areas as part of our Experience Strategy
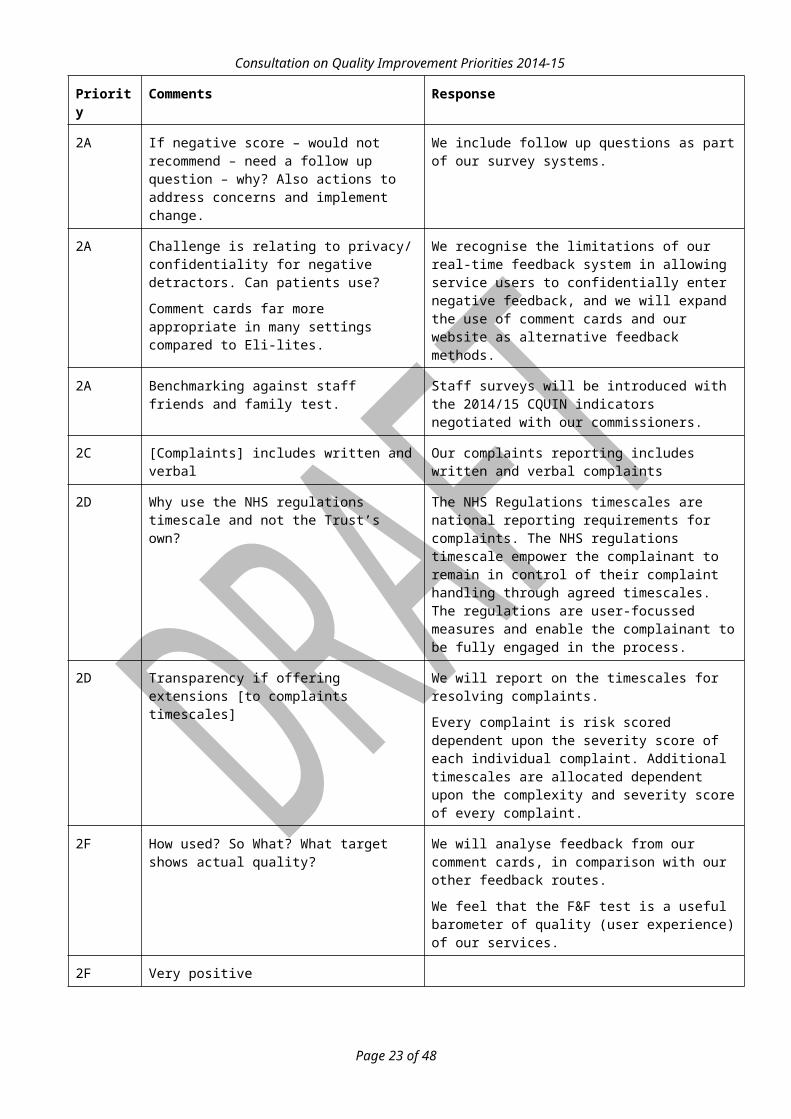
2A If negative score – would not recommend – need a follow up question – why? Also actions to address concerns and implement change.
We include follow up questions as part of our survey systems.
2A Challenge is relating to privacy/ confidentiality for negative detractors. Can patients use?
Comment cards far more appropriate in many settings compared to Eli-lites.
We recognise the limitations of our real-time feedback system in allowing service users to confidentially enter negative feedback, and we will expand the use of comment cards and our website as alternative feedback methods.
2A Benchmarking against staff friends and family test.
Staff surveys will be introduced with the 2014/15 CQUIN indicators negotiated with our commissioners.
2C [Complaints] includes written and verbal Our complaints reporting includes written and verbal complaints
2D Why use the NHS regulations timescale and not the Trust’s own?
The NHS Regulations timescales are national reporting requirements for complaints. The NHS regulations timescale empower the complainant to remain in control of their complaint handling through agreed timescales. The regulations are user-focussed measures and enable the complainant to be fully engaged in the process.
Page 15 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
2D Transparency if offering extensions [to complaints timescales]
We will report on the timescales for resolving complaints.
Every complaint is risk scored dependent upon the severity score of each individual complaint. Additional timescales are allocated dependent upon the complexity and severity score of every complaint.
2F How used? So What? What target shows actual quality?
We will analyse feedback from our comment cards, in comparison with our other feedback routes.
We feel that the F&F test is a useful barometer of quality (user experience) of our services.
2F Very positive
2F Comment card needs to be able to capture positive and negative comments.
Comment cards are designed as a simple generic feedback mechanism to allow comparisons between services.
They capture positive and negative comments.2F Could there be prompts on comment cards to
cover aspects re informed decisions – service effectiveness.
2F No comment cards seen by any of this group? Needs re launched, certainly NOT in all places where care is delivered. “You said, we did” gap in community? % in hospitals, again needs re-launched. Not sure if all current patient feedback tools have been to [the Experience Team] i.e. eclectic. Historical tools in use.
The Comment cards have been introduced through a staged approach. The initial roll out programme of the comment cards have been implemented in community teams
Our experience team has been developing consistent methods for gaining service user feedback across all Trust services, and will continue this work in 2014/15.
2F More focus on comments v complaints and how that is dealt with
We provide monthly reports on comments along with compliments which are reported to each community team. The PALS, Complaints, and Experience Teams work in collaboration with Operational teams to develop actions of improvement.
2H Is this in place yet? Still a feeling that pressure on clinical/ corporate staff to do complaints as part of their day job. Do we need to look at a separate team to handle them?
Our Customer Service team have introduced complaint case handlers who will assist and support staff who are investigating complaints, as part of the complaints process.
It is imperative that Managers and Team Leads capture the experience of users and carers accessing our services. Complaints should be viewed as a positive learning experience to drive actions of quality improvements.
Q2.1 Yes
Q2.2 Yes to both, otherwise corrective action is difficult
We report monthly data on the Friends and Family test by division.
Page 16 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
We provide monthly reports on comments along with compliments which are reported to each community team. The PALS, Complaints, and Experience Teams work in collaboration with Operational teams to develop actions of improvement
Q2.3 Friends and Family Test should be service focused NOT organisation focused.
Q2.3 Issues around capacity of investigating officers to undertake responses in the responses Could complaint investigators be outsourced?
All our staff are expected to learn from complaints in their area, including assisting with investigations and developing improvement plans as required.
It is imperative that our staff investigate, act on and learn from complaints. Complaints are a valuable source of feedback that can improve quality of services.
As a Trust we have outsourced internal complaint investigations for independence of complex complaints. Following lessons learnt through the introduction of Independent Investigations the Trust will still need to appoint an internal complaints lead who will provide support to the Independent Investigating Officer.
Q2.3 Excellence in customer service? The Trust is required to demonstrate compliance with 57 standards of the Customer Service Excellence. Independent validation of teams is reviewed by annual Independent onsite Customer Service Excellence assessors.
Q2.3 Do you have measures of “near misses” which may indicate organisational systemic weaknesses. If so what is the trend?
Our Safety priority includes the overall measure of number of incidents reported, (including “near misses”).
We analyse our incident data to look for systemic issues on a regular basis, and report significant findings to our Quality Governance Committee.
2F How will these be collected, who will be collecting these and from what time and funding will these come from i.e. budgets and who's time to hand out, explain, collate and manage?
Comment cards have been designed with self-addressed envelopes which glue at the sides into an envelope. Comment cards will be collated and analysed by the Experience team, and results will be fed back to each frontline team.
Q2.2 Yes I do think we need a divisional score but do we need targets NO!!!!!!!!! the results you get from your scores should indicate what needs to be happening, make decisions from that data do not start out with more than can be managed. this is a repeated issue, a new idea is set out, we must implement it, measure it and it must reach a target, all of this needs time and money to put in to place properly and that does NOT happen therefore it is only done half-heartedly and it becomes another example of not completely... just take the scores, measure and report them. If a problem becomes obvious then take that data and make the next objective from there.
Our desire is to improve the experience of our service users, and our measures and targets are driven by this desire.
We agree that measurement alone is not sufficient for improvement, and the burden of measurement must be minimised. We will use the NHS change model to help improve our services.
The set monthly target for our Net Promoter score / Friends and Family Test on our performance has been set by our Commissioners. This is included in the quality schedule for the Trusts commissioning contractual requirements.
Setting a reasonable target for each service will ensure that areas of lower quality are not “hidden in the average” overall Trust score.
Page 17 of 32

Consultation on Quality Improvement Priorities 2014-15
Page 18 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority 3: Effectiveness – Improving OutcomesConsultation measures and questions
Proposed measures for 2014/15
Proposed 2014/15 target
3A Number of teams demonstrating improvement in their outcome measures
All teams currently developing their outcome measures will have moved to their next level by the end of 2014/15 and will have as a minimum started collecting and analysing outcomes data (level 2a). Applicable teams:
Allied Health Professional teams
Therapy services teams
Children’s clinical teams
New teams will be participating in the outcome measures programme, and will have as a minimum a plan to develop evidence based outcome tools (level 1). Applicable teams:
Integrated Local Community Teams
Specialist Services teams
3B Average length of stay in community hospitals7
Monthly data not to exceed a median of 23 days throughout the whole year
Q3.1: Do you agree with the changes made to the Quality Improvement Priority around Effectiveness?
Q3.2: Should we include other measures? Should we delete any measures that are no longer appropriate?
7 This measure is routinely looked at as part of the Trust performance management suite of indicators, but is not directly related to outcome measures.
Page 19 of 32

Consultation on Quality Improvement Priorities 2014-15
Consultation commentsPriority Comments Response
3 “We want to provide effective services with positive outcomes for our service users.” – Is positive what the individuals want or what we think they want?
We agree, and we feel that this approach is covered by having two quality improvement priorities related to effectiveness; one for effective (service-based) outcomes and one for personalisation.
3 Should Improving Outcomes be broken down into 2 sections? 1) Improving outcomes for patient. 2) Monitoring/ evaluating of outcomes and what it means for staff. Quality impact assessment, would need to do a scoping exercise to identify additional resources required i.e. admin support, data base. Would it be one outcome or a number of outcomes?
3 How does this link to personalised care?
3 Linked to personalised health plan.
3A Links to personalisation see comments on priority 4.
3 “We want to provide effective services with positive outcomes for our service users.” – This is important but not conveyed in the priority measures. In the aim but not a measure. Could interweave with Priority 2 (customer satisfaction) to achieve this?
We feel that a first necessary step is to get our teams to consistently collect outcome data, and then move toward improving their outcomes during 2014/15.
Page 20 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
Many teams already use outcome measures, to track the progress of individual patients towards their clinical goal. It is less common for a team to analyse outcome measures across a cohort of similar patients to identify what is working well, and what improvements can be made.
Priority 2 (satisfaction) looks at a different dimension of quality, but some of the mechanisms for collecting and analysing data may overlap.
Monthly Ele-lite reports are disseminated to every Area Manager and Team Lead showing User Satisfaction levels relating to effectiveness of their services that they have received. This also includes involvement in care planning along with self- management programmes of empowerment.
3 So What? What does this improve for patients?
3 Link to NICE priorities and best practice We will encourage our teams to use outcome measures that are in line with evidence-based practice, including NICE priorities.3 Are the goals well set/ set in a SMART way,
personalised. Ensure can collect clear outcomes – refer to priority 4.
3 Should have ambition, how to measure the success and the process. This priority is about the process and how to reach the outcomes
First, we need robust and reliable systems to record outcomes. After this we can analyse and understand our outcomes, to enable improvement of our services.
3 Public can’t see the outcomes picked and why they have been picked.
We encourage our teams to use outcome measures in line with Evidence-Based Practice, and we will report the outcome measures we use in our Quality Account.
3 Define outcomes – Measure/ target is large and can’t say if it has been complete or not.
We will report progress of each team in developing outcomes in our Quality Account.
3 What does 41 teams mean? Is it a representative of the whole? Who is not taking part?
For 2013/14 our Children’s and Therapies teams participated in our outcomes programme. These teams will be listed in our Quality Account. We are proposing that all Integrated Locality Care Teams and specialist teams be involved in outcome measurement and improvement in 2014/15.
3 Need to understand where were we? Where are we now? Where do we want to be?
We regularly monitor the progress of our 41 participating teams in their use of outcome measures, and we will report this in our Quality Account.
3 A strength of outcome measures is that teams can design their own. Would this be possible if Integrated Locality Care Teams or would they need to work to a more generic set of outcomes – for example “I have a personalised support plan.”
Rarely do we need to design completely new measures – existing indicators have been “tried and tested” and can help us compare across services.
Page 21 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
3 The main concern is that Integrated Locality Care Teams in particular (plus Occupational Therapy) will be subject to this separate Quality Account. Team members will “buy in” to relevant measures – equally quality measures from two separate accounts can becomes a burden, not an enabler.
We produce one Quality Account for the Partnership Trust.
Our method for developing outcome measures involves frontline teams, so that we can develop relevant measures while minimising the burden on the team.
3 Mortality review- benchmarking – best practice – compliance, NICE etc., Quality standards.
We feel that achieving these essential governance processes represent “must-do” minimum standards for all our services, rather than quality improvement priorities.
3A “Applicable teams: Integrated Local Community Teams” – Integrated Locality Care Team?? Joint service spec for Integrated Locality Care Teams
Apologies for the typographical error. We have amended the priorities to consistently refer to our Integrated Locality Care Teams.
3A Communication and transition across services.
Our Effectiveness Team will share outcomes data with frontline teams, to allow for shared learning, and benchmarking where applicable.
3A Maybe list the teams involved now and who needs to be included in the future?
We will report team-by-team information on outcomes to our Effectiveness Group. We anticipate that all our frontline teams will be involved during 2014/15.
3A Need to ensure IT systems are in place to support staff to collect and analyse outcomes.
Our IT strategy will be looking at support for staff.
Our Effectiveness Team will provide assistance for analysing outcomes data.
3A Ensuring all teams have outcome measures. Focus on communities, plan for teams.
Our second phase of development for our Integrated Locality Care Teams will include mapping of community need to service provision.
Q3.1 Yes (x2)
Q3.1 Happy to remove (3B).
Q3.1 The risk is that team chase improvements – Key Performance Indicators – and not outcomes. Our framework is required, not two.
Our Quality Improvement Priorities are not intended to duplicate Key Performance Indicators, or replace the performance monitoring function. Our Quality Team and Performance Team will work together to ensure that work is not duplicated.
Q3.2 Benchmarking against other organisations, particularly with those teams at level 4 – outwards facing process for sharing and level 4 ambition for improvement.
We agree that benchmarking is useful to help share best practice and learning.
Our Effectiveness Team will encourage shared learning and benchmarking for comparable teams internally, and outward facing where possible.
Page 22 of 32
Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
Q3.2 More focus on social care - whole very health focus (and social care light) patient reported outcome measures need to be linked. Also bag of outcomes to suit everybody’s needs not just one.
We agree that our outcomes focus needs to encompass health and social care, which is why we have a quality priority looking at outcomes in terms of personalisation. We feel that the approach taken to develop outcome measures across our teams gives them flexibility to determine which set of outcome measures is most appropriate for the needs of their service users.
Q3.2 Service user considerations. What the outcomes is for the patient.
We will encourage teams to develop their outcome measures with full service user and stakeholder involvement, and also encourage the use of Patient Reported Outcome Measures.Q3.2 Need to identify what is a ‘good outcomes’
what is realistic and expectations. Take into account all stakeholders.
Q3.2 Map treatment timescales for recovery and effective outcomes for 3 / 4 pressure ulcers (relationship to priority 1 and 5)
While this is an important measure of the effectiveness of our services in relation to pressure ulcers, we feel that the relevant teams can include this in their outcome measures sets, rather than including it as a trust-wide outcome measure.
Q3.2 NICE, Quality standards compliance. Linkage PROMs.
Q3.1 Services or teams must demonstrate that outcomes have measurably and materially improved. Outcomes based commissioning is a fundamental part of NHS England’s, approach
I personally think this is a very short sighted method of NHS England and how to approach funding. This can be very effective in a limited number of services but this does not work well with all services. For example I work in adult physiotherapy, the majority of these community outpatients are a quick 20 min review appointment seen treated and notes written in that time, it’s very quick but a doable approach to funding that 20min slot. BUT I also work in paediatric physiotherapy and for example I saw a child with complex medical needs, on this past Friday I spent over 4 hours of my work time trying to deal with assessment, notes, letters to other health professionals and equipment issues for just this one patient. HOW can you justify giving the same sort of funding for those 2 individual physiotherapy patients?
With regard to demo outcomes that are measurable and materially improved..... it’s too sweeping of a policy and it does not apply to all services and I don’t feel that there are any options for those services that don’t have easy patients or answers.
It is not within the scope of this consultation to comment on national policy or commissioning decisions.
The evidence of improvement a patient makes towards their treatment goal is an important measure of the care we offer.
We feel that a focus on outcomes, rather than solely on activity, is a key way of measuring and improving the effectiveness of our services.
We also feel that all of our services should be focussing on improving the outcomes of the care they provide for their service users. In this respect, appropriate benchmarking with similar services (ie that provide services for similar cohorts of service users) would be a useful method of comparing the effectiveness of care.
Page 23 of 32

Consultation on Quality Improvement Priorities 2014-15
Page 24 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority 4: Effectiveness – Supporting Independence by Personalised CareConsultation measures and questions
Proposed measures for 2014/15 Proposed 2014/15 target
4A Service users who agree with key statements in “Making it Real” (e.g. “I have the information and support I need in order to remain as independent as possible”)
We are aiming to improve on the baseline. How the improvement will be measured is yet to be determined.
4B Percentage of people who receive directed support and / or direct payments
Achieve 70% by the end of the year
4C Percentage of people who feel that they were supported to make their own decisions about their social care and / or services
Maintain 85% through the whole year
4D Proportion of permanent admissions to residential or nursing care homes8
150 per 100,000
Q4.1: Rather than have a separate priority, should we include this measure as part of priority 3 (Effectiveness)?
Q4.2: As an Integrated health and social care organisation should we look to expanding the principles and method of “Making it real” across all services, rather than just those with a direct social care element?
Q4.3: Should we have a specific measure around personalisation?
Q4.4: Should we develop the effectiveness priority to include specific practice standards, in addition to personalisation?
8 This measure is routinely looked at as part of the Trust performance management suite of indicators, but is not directly related to personalisation.
Page 25 of 32

Consultation on Quality Improvement Priorities 2014-15
Consultation commentsPriority Comments Response
4 Are we being ambitious enough? Are we picking safe targets?
We develop and agree these targets with our commissioners.
4 Needs to be clear re: current % - how it relates to national guidance – are we meeting it?
4 Safeguarding/ adult protection (mental health) – how are we ensuring vulnerable adults are safe?
Our Head of Adult Safeguarding can provide more details on this query.
4A For people with dementia – these outcomes would be relevant to main family and carers
Our outcome measures for personalisation include surveying carers / relatives where appropriate.
On occasion personalisation of care includes “best interest” decisions for service users who lack capacity for decision making – these are handled according to a strict framework taking into account input from family and carers.
4B Should measure 70% of people for whom it is appropriate. Should the measures be separate?
This target is derived from a national indicator as part of the Adult Social Care Outcomes Framework. Our target of 70% reflects that not all service users would find this approach appropriate.
4B Receive SELF directed support We have corrected this typographical error.
4B Remove?? 70% of what? KPI not outcomes This target is derived from a national indicator as part of the Adult Social Care Outcomes Framework which are provide opportunities for us to benchmark our performance with comparable organisations, as well as charting improvement over time.
4B&C Need to be clear about what the % is? And what is the national average?
4B&C Swap order. We have changed the ordering to suit.
4C Agreed We are aiming for improvement in this area, and setting a baseline of maintenance at this point, as our targets are to be confirmed with our commissioners later in the year.
4C Should we get better? If achieving now is this a stretch?
4C A large portion of people may not have capacity so it is about their family/ carers.
4C 3A and 1B – surveys from county council. We receive our information for this indicator from the county council surveys and we are also looking to increase the sample size by additional surveys during 2014/15.
4C Definition of this – other information needs to be provided eg carers, dementia etc.
This nationally defined indicator is based on a monthly survey of eligible clients in receipt of services.
4D What is the current figure of proportion of permanent admissions? (therefore what is achievable/ Is it achievable?)
Given the comments received we feel that it can be removed from our top five quality improvement priorities.
Page 26 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
This is a national indicator as part of the Adult Social Care Outcomes Framework, and we will continue to monitor this measure monthly.
4D There are external factors not manageable by SSOTP that will prevent this? Pressure from family members?
4D Family members stuck in the middle – care home managers vs healthcare – users are not clear about who is responsible for what? Podiatry – it feels that you lose some rights to the NHS when you enter a private nursing home.
4D Is it about the length of stay in permanent care?
4D So what?! But may become more important if care at home becomes less affordable than care homes.
Q4.1 Interdependent of each other. Clear personalised goal setting, clear outcomes/ measurement – measure service user experience – umbrella across all = safe staffing levels.
After consideration we decided to keep two distinct priorities related to Effectiveness.
We will keep the priority around personalisation separate.
Q4.1 Yes – as personalisation is inherent in the life of Integrated Locality Care Teams in a case management and outcomes are a better measure. So much of the KPI system measures outputs, not outcomes. The proposed measured about, especially point one, are outcome measures.
Q4.1 Needs to be separate – acknowledgement of complexity of social care.
Q4.1 Separate – delivered by somebody else – council and social care as a statutory requirement – needs more focus – how we input that care. – needed internally for integration and organisation needs to be clear about the services we provide.
Q4.2 Yes it should be down to personal choice. Making it real is patronising.
“Making it real” is a national initiative via Think Local Act Personal, which marks progress towards personalised, community-based support. It is beyond the scope of this consultation to comment on whether the “making it real” term is patronising.
See www.thinklocalactpersonal.org.uk
We agree that the principles in “making it real” can be extended across all our services, and will work towards this during 2014/15.
Q4.2 Yes, should be integrated. “making it real has not been promoted at all in the last year in social care, hence Integrated Locality Care Teams would and should expand the vision of personalised services/ support plan to cover all people supported via Integrated Locality Care Teams/ support plan/ case management
Q4.3 Quality life measures. As part of our audit programme we will develop measures for personalisation during 2014/15.
We will consider quality of life as part of these measures, as well as personalised goal setting.
Q4.3 Yes, we need clear personalised goal setting in order to be able to measure outcomes linked to priority 3.
Page 27 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
Q4.3 How do we ensure that carers are supported as these are critical to ensuring patients/service users stay at home.
We agree. Support planning currently includes carer requirements. Our staff carry out joint client and carer assessments at the outset, and annual joint reviews.
We have a SC31 indicator that measures our performance in this area.
Our professional lead for social work can provide more information on this query.
Q4.3 For Integrated Locality Care Teams, the number of people with personalised support plan (including case management) could be a “holistic” measure across nursing and social care and could be supported by a couple of outcomes in the services
We agree.
As part of our audit programme we will develop measures for personalisation during 2014/15.
Q4.4 Are any of these measures relevant to people with dementia (their carers) for whom daily maintenance requirements are then met by informed carers. Should there be a separate question for carers/ people with dementia. Needs also to link with personalised “health budgets”
For our social care clients that suffer from dementia, our joint assessments recognise this.
Q4.4 Personalised goal planning, rather than just using a tool for the sake of it. Need to measure outcomes using appropriate tool. Use tools/ data analysis for continuous improvement.
We agree.
As part of our audit programme we will develop measures for personalisation during 2014/15.
Q4.2 Yes
Q4.3 Personalisation is relevant to health and social care
We agree.
Our Integrated Locality Care Teams include health and social care professionals.
Page 28 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority 5: Safety – WorkforceConsultation measures and questions
Proposed measures for 2014/15 Proposed 2014/15 target
5A Number of routine services that deliver against clinical standards in line with 7-day working according to national guidance
We will determine all relevant services that the national guidance on 7-day working applies to, and ensure that these services comply with the guidance for 7-day working.
5B Publish monthly staffing levels for our community wards, including agreed establishment, safe staffing level in relation to acuity, and actual staffing levels.
Staffing is always at a safe level in relation to shift-by shift service need, taking into account the demand on the service.9
5C Publish two acuity staffing establishment reviews, which look at safe staffing levels in community hospitals, during 2014/15
Reviews will make use of national guidance, professional body guidance and best practice on staffing levels, and will aim to demonstrate appropriate staffing establishment and skill mix, for the provision of safe care.
Q5.1: Should an additional priority for Safety become a Trust Quality Improvement Priority? If so, what targets and measures would be realistic?
Q5.2: Do you agree with the addition of a measure for safe staffing and its associated target? What should this measure focus on?
Q5.3: Do you agree with the addition of a measure for 7 day working?
9 Details on how this will be reported are to be developed by April 2014
Page 29 of 32

Consultation on Quality Improvement Priorities 2014-15
Consultation commentsPriority Comments Response
5 Empowering/ supporting staff – staff survey, “Friends and Family Test” for staff.
While we measure and monitor these aspects of quality, we did not consider them part of our top 5 quality improvement priorities.
5 Does this offer anything? We Know we have a deficit; We have to do it anyway. Think about how to make it unique to the Quality Account and how it will be completed.
We have removed 5A as a result of these comments, recognising the additional work required to design clear indicators of our progress toward 7-day working.
5 Organisation needs to define what a 7 day service entails.
5 Need to be clear about what 7 day working/ services means – what is the model of delivery?
5 Is Monday – Friday the same as Saturday and Sunday? Or is the weekend a different service eg on call reduced working hours etc.
5 Is there demand for specific services for 7 day – need to think about how we would provide the service.
5A Isn’t about individual choice/ Would people want to see physiotherapist on a Sunday? Wouldn’t it be better to extend working days and have a shift?
5A Is this about health?
5B Should be for community teams also? Behind this is developing local clinical nursing leadership. Accountability. Safety culture – linked to Keogh. Too big to do community services in year 1.
We recognise the value of developing 7-day working across all our services, although the high priority areas for 2014/15 mainly relate to our community hospitals.
5B&C “community wards/hospitals” – ALL services
Q5.1 Yes
Q5.1 Staffing in community – skill mix and numbers: demand is vital to safety targets,
Our safe staffing monitoring will include a professional judgement from the frontline on whether a service is safe, based on the current shift staffing and the demand on the service.
Q5.1 Safety of staff and quality could be called in jeopardy
Q5.2 Yes – additional measures for quality of staff
Q5.2 Need to move away from the target being the numbers and keep personal e.g. if there is a 1:1 patient in. Services and staffing needs to be flexible and competent.
Q5.2 Yes
Page 30 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
Q5.3 Yes - there is a gap for community services and lack of clarity around measures/ tools that could be used to be the achievable measures. Links in with [the Transformation Team’s] workforce analysis tool that is being piloted in Integrated Locality Care Teams and is beginning to be used in therapies. Need to ensure that streams of work are more inter related i.e. not silo. Does everyone know for example all the streams of work that the transformation team are leading on and how do they link in with the quality framework/ priorities.
We are taking a programme approach for 7-day working as we recognise the scope and long term nature of this work across the whole Trust.
Q5.3 Yes – additional measures for quality of staff.
Q5.3 The only way to keep people out of hospital and in the community is by having a 7day service.
We agree that our community services play a vital role in supporting hospitals to deliver 7-day working.
Q5.3 Relevant to whole organisation not just community hospitals. What is impact of 7 days on community services? Achievable aims for the year.
We are taking a programme approach for 7-day working as we recognise the scope and long term nature of this work across the whole Trust.
Q5.2 Sounds like another situation of reporting and think of all the ways to fiddle the results. If you want to know how many people are on a ward then do spot checks and make sure those that are doing the spot checks are truthful.
I think this will just be another report that staff will have to fill in when really what health care staff want to do is TREAT patients and not do more paperwork. If those that want to know then get on a ward and find out, unannounced.
Of course we all want the reassurance that more staff will be on a ward and that is not where the funding is being cut back but i am not sure this is the best method of capturing the data.
Our reporting requirements of front line staff are driven by our priorities – not the other way round.
We feel that recording of quality care is an integral part of demonstrating and delivering quality care.
In line with our Quality Framework, we want to empower our community hospital staff to deliver high quality, and one of the ways we will do this is by asking them whether they feel that their service is at a safe staffing level on a shift-by-shift basis.
Q5.3 I think you are ref to 7 day working across the board in all services... health care needs are 7 day but not all services will be access no matter what on all days of the week. Even people that work don’t want out patient physiotherapy on a Sunday morning.
I think it’s a cheap method of not paying your staff in truth.
We agree that 7-day working is not about providing all our services every day, but providing the right care at point and time of need.
We feel that 7-day working will provide our staff opportunity for working flexibly.
7-day working is not a cost-saving initiative or way to squeeze more work out of our staff, but involves providing a quality service based on need.
Page 31 of 32

Consultation on Quality Improvement Priorities 2014-15
Priority Comments Response
Q5.1 Do you have measures of “near misses” which may indicate organisational systemic weaknesses. If so what is the trend?
Also measuring trends in litigation case numbers and costs would be useful
Our incident reporting system captures incidents, including “near misses”, and these are reported via our governance structures.
We monitor incident trends regularly, including reports to our Trust Board.
We review trends in litigation internally on a quarterly basis, due to the confidential nature of this area.
Q5.2 This is very hospital and nursing based – what about other services, e.g. community nursing where it is less easy to define ‘safe’ staffing levels – as a community Trust it seems odd there is no mention of this.
We recognise the value of developing 7-day working across all our services, although the high priority areas for 2014/15 mainly relate to our community hospitals.
Q5.3 No – we are not commissioned to deliver this in a number of services and would require investment.
Our plans for implementing 7-day working will include appropriate investment, and dialogue with our commissioners.
Our work in this area will also be according to the national timescales for implementation of 7-day working.
5 Priorities for service users:ensuring appropriate staffing levels are maintain in custodial healthcare settings to ensure full delivery of contracted services
Priorities for staff:providing cover for LTS staff in a custodial setting for within directorate resources in clinical community settings
Priorities for partners:to ensure commissioners consider the impact of H/C staffing on prison regimes within custodial environments
While we agree that appropriate staffing levels in custodial healthcare settings are important we did not feel this specific aspect would be one of our top 5 quality priorities for 2014/15.
However, we are conducting a workforce development review (commencing April 2014) for prison healthcare services staffing levels and skill mix.
Page 32 of 32


















