| Slide 1 of 25 April 2007 Training Workshop on Pharmaceutical Development with focus on Paediatric...
111
| Slide 1 of 25 April 2007 Training Workshop on Pharmaceutical Development with focus on Paediatric Formulations Protea Hotel Victoria Junction, Waterfront Cape Town, South Africa Date: 16 to 20 April 2007 Pharmaceutical Development
-
Upload
trent-aston -
Category
Documents
-
view
215 -
download
2
Transcript of | Slide 1 of 25 April 2007 Training Workshop on Pharmaceutical Development with focus on Paediatric...

| Slide 1 of 25 April 2007
Training Workshop on Pharmaceutical Development
with focus on Paediatric Formulations
Protea Hotel
Victoria Junction, Waterfront
Cape Town, South Africa
Date: 16 to 20 April 2007
Pharmaceutical DevelopmentPharmaceutical Development

| Slide 2 of 25 April 2007
Pharmaceutical Development:Pharmaceutical Development:
Bioavailability and bioequivalence in Paediatric medicine
Presenter: Jean-Marc AIACHEEmeritus Professor,
Auvergne University,
Faculty of Pharmacy,
28 Place Henri Dunant
63000 Clermont-Ferrand, France

| Slide 3 of 25 April 2007
Pharmaceutical DevelopmentPharmaceutical Development
Outline and Objectives of presentation
Definitions and relevance to paediatric medicines
Relevance of paediatric pharmacokinetics
Measurement
Regulatory Aspects
Formulation Strategies
Ethical considerations in design and conduct of bioavailability studies in children

| Slide 4 of 25 April 2007
Definitions and relevance to paediatric medicines
Definitions and relevance to paediatric medicines
Bioavailability
Bioavailability means the rate and extent to which the active substance or active moiety is absorbed from the pharmaceutical form and becomes available at the site of action … (in the general circulation)” EMEA CPMP/EWP/QWP 1401/88 date for coming in operation January 2002

| Slide 5 of 25 April 2007
F.D.A definitionF.D.A definition

| Slide 6 of 25 April 2007
Comparison of definitionsComparison of definitions
The rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action. (21 CFR 320.1. US)
The rate and extent to which the active ingredient or active moiety is delivered from a pharmaceutical form and becomes available in the general circulation (CPMP/EWP/QWP/1401/98, EU)
(practical definition for substances intended to exhibit a systemic effect)

| Slide 7 of 25 April 2007
F.D.A(cont..)F.D.A(cont..)
So this determination must be considered as a value of the
performance of the drug dosage form, quite as a parameter of the dosage form.

| Slide 8 of 25 April 2007
F.D.A(cont..)F.D.A(cont..)

| Slide 9 of 25 April 2007
F.D.A (cont..)F.D.A (cont..)

| Slide 10 of 25 April 2007
Bioavailability: why?Bioavailability: why?Where is the place of
Bioavailability in the future of a dosage form in the human being?

| Slide 11 of 25 April 2007
L.A.D.M.E.R. systemL.A.D.M.E.R. system

| Slide 12 of 25 April 2007
Technological (galenicals!) Factors of B.ATechnological (galenicals!) Factors of B.A
DDFRelease
Free APIDissolution
Dissolved API Absorbed drug
Absorption

| Slide 13 of 25 April 2007
Drug Product
Release
Drug released
Dissolution
Dissolved drug
AbsorptionAbsorbed drug
Type of DDF
Manufacturing process
Excipients
Physical-chemical Prop of API.
Solubility
Dissol. Rate
crystals
Subject, race, age, sex, disease,…

| Slide 14 of 25 April 2007
relevance to paediatric medicinesrelevance to paediatric medicines
The technological factors have the same influence in Adults and children ,except for dissolution rate due to the difference of volume of liquids for example…and taste of DF which increase the gastric secretion (Pavlov …)
Physiological factors influencing BD: They are fundamentally different from adults.
Age ,race, metabolism state, particularly the A.D.M.E phenomena in children

| Slide 15 of 25 April 2007
Modification of absorption phenomenaModification of absorption phenomena
Oral Route :Rate of intestinal absorption decreased in the newborn.
Gastric pH:
* no HCl in the newborn until the end of the first month
** the level of gastric secretion of adults is reached only after four to six years.
This can explain:
*the low absorption of weak acid like Phenobarbital and Aspirin and
**a better absorption of weak basic substances.

| Slide 16 of 25 April 2007
Oral RouteOral Route
Gastric emptying rate is decreased in the newborn
The half- life is about 90 minutes. At six to eight months this value reach the adults value,80 min.
the synthesis of biliary acid is quite of the half of adult value.
This can explain the law absorption of lipid soluble substances, essentially vitamins A.,E,.D and K.
The bacteria in the colon come later after the birth and depend on the type of food.
The milk which is used largely generally reduces the absorption of some products by adsorption;

| Slide 17 of 25 April 2007
Rectal routeRectal route
The absorption is convenient in case of oral intolerance and overall if the drug is administered in solution, like enema for the treatment of convulsions with diazepam or midazolam.
The absorption is not so good after suppositories administration.

| Slide 18 of 25 April 2007
Intramuscular routeIntramuscular route
The absorption rate is low and hazardous in the newborn due to low blood flow rate in the muscles, a low amount of muscle masses and low motor function of the baby.

| Slide 19 of 25 April 2007
Cutaneous administrationCutaneous administration
The skin absorption is more important in the newborn than in adults.
This can be explain by the elevated ratio between the skin area and the weight, and by the elevated hydratation of the stratum corneum.
But this route is essentially used for topical application and not for systemic activity
The dosage form must be a administered
on a non injured skin .

| Slide 20 of 25 April 2007
Other ModificationsOther Modifications
Distribution Volume:
The water soluble drugs will be prescribed at high doses (amino glycosides, theophyllin, aminosides, penicillin, cephalosporin, phénytoïn, vancomycin, bétalactamines …) in premature newborn.
The lipid soluble drug (diazepam, Phenobarbital…) will be prescribed at lower doses (high peak ,low VD)
Protein Binding
Evolution of metabolism organs.

| Slide 21 of 25 April 2007
ConsequencesConsequences
i.e., in the newborns absorption and elimination are reduced, distribution volume increased. So the time between 2 doses is large and it is to be noted that highly protein bounded drug must be discarded.
i.e. in the babies, the metabolism is accelerated, distribution volume is high. So the single dose must be more elevated but dosing interval smaller than in adults

| Slide 22 of 25 April 2007
QuestionQuestion
Do we have to do Bioavailability studies in babies and in general in children?
yes

| Slide 23 of 25 April 2007
Question Question
Study of all dosage forms?
yes

| Slide 24 of 25 April 2007

| Slide 25 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 26 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 27 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 28 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 29 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 30 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 31 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 32 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 33 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 34 of 25 April 2007
Clinical InvestigationClinical Investigation

| Slide 35 of 25 April 2007
PharmacokineticsPharmacokinetics

| Slide 36 of 25 April 2007
PharmacokineticsPharmacokinetics

| Slide 37 of 25 April 2007
PharmacokineticsPharmacokinetics

| Slide 38 of 25 April 2007
Dose calculation:area/weight.Normogram
Dose calculation:area/weight.Normogram

| Slide 39 of 25 April 2007

| Slide 40 of 25 April 2007

| Slide 41 of 25 April 2007
ProtocolProtocol

| Slide 42 of 25 April 2007
ProtocolProtocol

| Slide 43 of 25 April 2007
SubjectsSubjects

| Slide 44 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 45 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 46 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 47 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 48 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 49 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 50 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 51 of 25 April 2007
Ethical issues in pediatric studiesEthical issues in pediatric studies

| Slide 52 of 25 April 2007
BioequivalenceBioequivalence
“Bioequivalence is the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study.”
Bioavailability and Bioequivalence Studies for Orally Administered Drug Products — General Considerations Food and Drug Administration October 2000

| Slide 53 of 25 April 2007
BioequivalenceBioequivalence
“This definition emphasizes the use of pharmacokinetic measures in an accessible biological matrix such as blood, plasma, and/or serum to indicate release of the drug substance from the drug product into the systemic circulation.
This approach rests on an understanding that measuring the active moiety or ingredient at the site of action is generally not possible and, furthermore, that some relationship exists between the efficacy/safety and concentration of active moiety and/or its important metabolite or metabolites in the systemic circulation.”Bioavailability and Bioequivalence Studies for Orally Administered Drug Products — General Considerations Food and Drug Administration October 2000

| Slide 54 of 25 April 2007
BioequivalenceBioequivalence
Pharmacodynamic studies are not recommended for orally administered drug products when the drug is absorbed into the systemic circulation and a pharmacokinetic approach can be used to assess systemic exposure and establish BE.”Bioavailability and Bioequivalence Studies for Orally Administered Drug Products — General Considerations Food and Drug Administration October 2000

| Slide 55 of 25 April 2007
Comparison of definitionsComparison of definitions
Pharmaceutical equivalents or pharmaceutical alternatives whose rate and extent of absorption do not show a significant difference when administered at the same molar dose of the therapeutic moiety under similar experimental conditions, either single dose or multiple dose. (27 CFR 320.1(e)).
Two medicinal products are BE if they are pharmaceutical equivalents or pharmaceutical alternatives and if their Bioavailabilities after the administration of the same molar dose are similar to such degree that their effects, with respect to both efficacy and safety, will be essentially the same (CPMP/EWP/QWP/1401/98, EU)

| Slide 56 of 25 April 2007
Definitions (CPMP/EWP/QWP/1401/98, EU)Definitions (CPMP/EWP/QWP/1401/98, EU)
Pharmaceutical equivalents:– Same amount active substance– Same dosage forms
Pharmaceutical alternatives:– Same amount of active moiety– In different chemical form or– Different dosage form

| Slide 57 of 25 April 2007
Bioequivalence : Why?Bioequivalence : Why?
“Prescribability refers to the clinical setting in which a practitioner prescribes a drug product to a patient for the first time. In this setting, the prescriber relies on an understanding that the average performance of the drug product has been well characterized and relates in some definable way to the safety and efficacy information from clinical trials.
Switchability refers to the setting in which a practitioner transfers a patient from one drug product to another. This situation arises with generic substitution, as well as with certain post approval changes by an innovator or generic firm in the formulation and/or manufacture of a drug product. Under these circumstances, the prescriber and patient should be assured that the newly administered drug product will yield comparable safety and efficacy to that of the product for which it is being substituted.”
“Guidance for Industry Average, Population, and Individual Approaches to Establishing Bioequivalence” Aug 1999

| Slide 58 of 25 April 2007
Bioequivalence: WhenBioequivalence: When
To compare 2 dosage forms administered by the same way, but with formulation or Manufacturing Process different ,in the same company.
To compare 2 dosage forms of formulation and M.P unknown: ”Generics”

| Slide 59 of 25 April 2007
What is a GenericWhat is a Generic
1st definition given in France(1963) by the Trade Minister:
“Copy of a drug product ,the production and marketing of which are allowed after the patent caducity”.
It contains the same API, the same excipients, has the same therapeutic effects and /or secondary and is administered by the same route: TRUE COPY

| Slide 60 of 25 April 2007
Definitions (CPMP/EWP/QWP/1401/98, EU)Definitions (CPMP/EWP/QWP/1401/98, EU)
Essentially similar products: – Same qualitative-quantitative composition in active substances– Same dosage form*– Bioequivalent– *By extension for IR products the concept also applies to
different oral forms (tablets and capsules) with same active substance.
– In France all the Essentially similar product to an innovator are classified in a Generic family of” XXX”

| Slide 61 of 25 April 2007
Bioequivalence on what???Bioequivalence on what???
On a general point of view for all dosage forms for routes of administration!!

| Slide 62 of 25 April 2007
FDA / EMEA recommendationsFDA / EMEA recommendations

| Slide 63 of 25 April 2007
FDA / EMEA recommendationsFDA / EMEA recommendations

| Slide 64 of 25 April 2007
Bioequivalence : How?Bioequivalence : How?

| Slide 65 of 25 April 2007
Methods for assessing BE1
USA
Pharmacokinetic study
Pharmacodynamic study
Comparative clinical study
In vitro study
1.GUIDANCE FOR INDUSTRY
Bioavailability and Bioequivalence Studies for Orally Administered Drug Products — General Considerations
Methods for assessing BE1
UE
Alternatively to classical BA studies
using pharmacokinetics end points to
assess BE, other types of studies can be
envisaged, e.g. human studies with
clinical or pharmacodynamic end-points,
studies using animal models or in vitro
studies as long as they are appropriately
justified and/or validated1.Note for guidance on the investigation of BA and BE (CPMP/EWP/QWP/1401/98, EU)

| Slide 66 of 25 April 2007
ParametersParameters

| Slide 67 of 25 April 2007
ParametersParameters

| Slide 68 of 25 April 2007
ParametersParameters

| Slide 69 of 25 April 2007
ParametersParameters

| Slide 70 of 25 April 2007
ParametersParameters

| Slide 71 of 25 April 2007
ParametersParameters

| Slide 72 of 25 April 2007
Nevirapine was readily absorbed (> 90 %) after oral administration in healthy volunteers and in adults with HIV-1 infection.A 3-way crossover study compared the bioavailability from three production/commercial scale batches with varying dissolution profiles. All three batches were bioequivalent with respect to systemic exposure (AUC). The significantly different values for Cmax and tmax were considered not to be clinically relevant.In studies 1100.1231 and 1100.896 in which the suspension was administered directly using a syringe, it was demonstrated that the suspension and tablet formulations were comparably bioavailable with respect to extent of absorption. In study 1100.1213 the suspension was administered in a dosing cup without rinsing. The suspension intended for marketing was bioequivalent to the suspension used during clinical trials but was not bioequivalent to the marketed tablets. This could be attributed to incomplete dosing of the two suspensions since there was about 13 % of the dose remaining in the cup.
Example: NevirapineExample: Nevirapine

| Slide 73 of 25 April 2007
ExampleExample
It has been later determined in a single dose study in 9 patients aged between 9 months and 14 years administered after an overnight fast (3 patients per dose level equivalent to 7.5 mg/m², 30.0 mg/m² and 120.0 mg/m²).
Based on adult experience, a comparable lead-in period of two weeks was suggested for paediatric population. A 4 mg/kg dose is proposed for all children regardless the age. Although no particular study has been performed to find the optimal lead-in dose, this dose was considered acceptable considering the enzyme induction to achieve initial antiretroviral activity.
The final recommended doses for the different ages are therefore the following:
Patients from 2 months to 8 years, 4 mg/kg once daily for 2 weeks followed by 7 mg/kg bid
Patients from 8 years to 16 years are 4 mg/kg once daily followed by 4-mg/kg bids.

| Slide 74 of 25 April 2007
Bioequivalence: Compulsory???Bioequivalence: Compulsory???
Drug dependence and DF dependence

| Slide 75 of 25 April 2007
J P C
PermeabilitySolubility andDissolution rate In vivoLuminal degradation
•Same dissolution profile•Formulation components do not alter permeability or intestinal transit
Amidon GL. Lennernas H. Shah VP. Crison JR. A theoretical basis for a biopharmaceutic drug classification: the correlation of in vitro drug product dissolution and in vivo bioavailability. Pharm. Res. 12(3):413-20, 1995

| Slide 76 of 25 April 2007
Class I: HS/HP
Verapamil, Propranolol Metoprolol
Class II: LS/HP
Carbamazepine, Ketoprofen, Naproxen
Class III: HS/LP
Ranitidine, Cimetidine, Atenolol
Class IV: LS/LP
Furosemide, Hydrochlorothiazide
Per
mea
bili
ty
Volume of aqueous buffer to dissolve the highest dose
BCS classificationBCS classification

| Slide 77 of 25 April 2007
Permeability classificationPermeability classification
What is a good permeability?
How can we estimate intestinal permeability?
)()( hg EEFaF 11Eg= gut first-pass effects
Eh= liver first-pass effects

| Slide 78 of 25 April 2007

| Slide 79 of 25 April 2007
(2 ) 1 nA
aF e Absorption number An
( )eff res
resabs
P TAn T
R T
A high Permeability value ensures that the drug is completely absorbed during its residence time in intestine. (in absence of formulation factors)

| Slide 80 of 25 April 2007
Solubility: How much is enough?
Dissolution and solubility in what?

| Slide 81 of 25 April 2007
Average physiological pHs in GI tract. Fasted/fed
Average physiological pHs in GI tract. Fasted/fed
Sitefasted
Stomach1.4 - 2.1
Duodenum4.9 - 6.4
Jejunum4.4 - 6.5
Ileum6.5 - 8.0
Adapted from Dressman et al. Pharm.Res 15(1) 11-22(1998)

| Slide 82 of 25 April 2007
Average physiological pHs in GI tract. Fasted/fed
Average physiological pHs in GI tract. Fasted/fed
Sitefastedfed
Stomach1.4 - 2.13.0 - 7.0
Duodenum4.9 - 6.45.1 - 5.2
Jejunum4.4 - 6.55.2 - 6.2
Ileum6.5 - 8.06.8 - 8.0
Adapted from Dressman et al. Pharm.Res 15(1) 11-22(1998)

| Slide 83 of 25 April 2007
High solubility:– When the active substance is highly soluble, the product could
be in general exempted from in vivo BE studies.– The amount contained in the highest dose strength of an IR
product is dissolved in 250 mL of each of three buffers within the range of pH 1-8 at 37ºC (preferably pH 1.0, 4.6, 6.8)
Exemption criteria of IN VIVO studies UE

| Slide 84 of 25 April 2007
Solubility: Dose/solubility ratio and Do dose number
Solubility: Dose/solubility ratio and Do dose number
D/S Gives the volume necessary to dissolve the given dose of the active substance
Do
250D
DoCs
Drug solubility
Dose
High solubility ensures that solubility is not likely to limit the dissolution and therefore absorption.

| Slide 85 of 25 April 2007

| Slide 86 of 25 April 2007

| Slide 87 of 25 April 2007
Dissolution rate: Dn dissolution number
Dissolution rate: Dn dissolution number
2
3 s resres
diss
C TDDn T
Tr
Diffusivity5*10-6 cm2/s
Particle radius~25m
Solubility mg/mL
Density~1.2mg/mL
Residence timein small intestine~180 min
Time required forComplete dissolution
Rapid dissolution ensures that in vivo dissolution is not likely to be the rate limiting step

| Slide 88 of 25 April 2007
UE-EMEA
Rapid dissolution:– Demonstrate similarity of
dissolution profile between test and reference in each of three buffers within the range of pH 1-8 at 37ºC (preferably pH 1.0, 4.6, 6.8).
– In cases where more than 85% of the active substance are dissolved within 15 minutes, the similarity of dissolution profiles may be accepted as demonstrated.
Exemption criteria of IN VIVO studies
USA-FDA
Rapidly dissolving– When no less than the 85% of
the labeled amount of the drug substance dissolves within 30 mins using USP apparatus I (100 rpm) or II (50 rpm) in a volume of 900 mL or less in each of the following media 0.1 N HCL, (or SGF without enzymes) pH4.5 buffer, pH 6.8 buffer or SIF (without enzymes).

| Slide 89 of 25 April 2007
Biowaiver: permission to use dissolution test as a surrogate of pharmacokinetic data: Dissolution test: In vitro Bioequivalence
Biowaiver: permission to use dissolution test as a surrogate of pharmacokinetic data: Dissolution test: In vitro Bioequivalence
High solubility, pH 1-8 (6.8)
Linear and complete absorption
Rapid dissolution (T85<30min, pH=1.0,4.6,6.8)
Excipients well established (not large doses)
Risk of therapeutic failures
High solubility, pH 1-7.5 (6.8)
High permeability (Fabs>90%)
Rapid dissolution (T85<30min, pH=1.2,4.5,6.8)
Excipients currently approved for IR Dosage Forms (FDA Inactive Ingredients List)
Non-NTI drugs
EMEA/CPMP and FDA/BCS

| Slide 90 of 25 April 2007
Classify WHO Essential DrugsClassify WHO Essential Drugs
Readily available data (solubility)
Easily Implemented Estimation (permeability)
Provisional Classification

| Slide 91 of 25 April 2007
WHO and US DrugsWHO and US Drugs
WHO
325 Medicines
260 Drugs
123 Oral IR
US
200 Drug Products
141 Oral
43 on WHO List

| Slide 92 of 25 April 2007
Descriptive TermParts of solvent required forSolubility range,Solubility
assigned,
(Solubility Definition)1 part of solutemg/mlmg/ml
Very soluble (vs)Less than 11000 and over1000
Freely soluble (fs)From 1 to 10100 to 1000100
Soluble (s)From 10 to 3033 to 10033
Sparingly soluble (sps)From 30 to 10010 to 3310
Slightly soluble (ss)From 100 to 10001 to 101
Very slightly soluble (vss)From 1000 to 10,0000.1 to 10.1
Practically insoluble (pi)10,000 and overLess than 0.1 0.01
Merck SolubilitiesMerck Solubilities

| Slide 93 of 25 April 2007
Solubility ClassificationSolubility Classification
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
Dose number ≤ 1.0 Solubility ≤ 0.1 mg/ml Solubility ≤ 0.01 mg/ml No solubilityinformation
Per
cen
tage
of
imm
edia
te-r
elea
se o
ral d
rugs
WHO
US
High Solubility Drugs250
s
DDo
C

| Slide 94 of 25 April 2007
Solubility ConclusionsSolubility Conclusions
Majority of Drugs of the WHO list are High Solubility (Do<1)

| Slide 95 of 25 April 2007
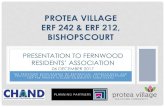
Human jejunum permeability (x10-4 cm/s)0 2 4 6 8 10 12
Hum
an fr
actio
n ab
sorb
ed (%
)
0
20
40
60
80
100
120
Trend line
D-glucoseVerapamil Piroxicam Phenylalanine Cyclosporin Enalapril Cephalexin Losartan Lisinopril Amoxicillin Methyldopa NaproxenAntipyrine Desipramine PropanololAmiloride Metoprolol Terbutaline MannitolCimetidine Ranitidine Enalaprilate Atenolol Hydrochlorothiazide
Human Jejunal Permeability Data BaseHuman Jejunal Permeability Data Base

| Slide 96 of 25 April 2007
WHO Essential DrugsWHO Essential Drugs
67% of WHO IR drugs are High Solubility
68% of US Top 200 drugs are HS
In Vitro Dissolution BE standard is applicable to the majority of WHO Drugs
Easily implemented, routinely conducted

| Slide 97 of 25 April 2007
What to do for children??What to do for children??
Use of BCS for API
Study of the dosage form in vitro whatever the BCS of the API if there is a reference as the innovator and comparison with sharpness of the dissolution curves and results. There is a dissolution device for all the dosage form and a lot of possibility for media!!
Correlation IVIVC to be developed, but no extrapolation of adult data to children, except in case of proof!!!
It seems better to privilege the PD bioassays than PK with sampling in children if it possible and so to facilitate the determination of exposure /activity with M.AC. than exposure /plasmatic levels, essentially for antibiotics ,antiviral, anticancer drugs.

| Slide 98 of 25 April 2007
Proposed BE DissolutionProposed BE Dissolution
BCS ClassDrug Solubility pH 1.2Drug Solubility pH 6.8Drug PermeabilityPreferred Procedure
IHighHighHigh>85% Dissolution in 15 min., pH = 6.8.
II-AHighLowHigh>85% Dissolution in 15 min., pH = 1.2.
II-BLowHighHigh
>15 min at pH=1.2, then 85% Dissolution in 30 min., pH = 6.8; F2>50; 5 points minimum; not more than one point > 85%.
II-CLowLowHigh>15 min at pH=1.2; then 85% Dissolution in 30 min., pH = 6.8 plus surfactant*; F2>50; 5 points minimum, not more than one point > 85%.
IIIHighHighLow>85% Dissolution in 15 min., pH = 1.2, 4.5, 6.8.
IV-AHighLowLow>85% Dissolution in 15 min., pH = 1.2.
IV-BLowHighLow
>15 min. at pH = 1.2; then 85% Dissolution in 30 min., pH = 6.8,; F2>50; 5 points minimum.; not more than one point > 85%.
IV-CLowLowLow
>15 min at pH=1.2; then 85% Dissolution in 30 min., pH = 6.8 plus surfactant*; F2>50; 5 points minimum, not more than one point > 85%.

| Slide 99 of 25 April 2007
Recent Examples of BA and BIE trials Recent Examples of BA and BIE trials
Sponsored by:National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)Information provided by:National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)ClinicalTrials.gov Identifier:NCT00436878Purpose
The purpose of this study is to test the effects of large food portions on children's eating. Experiment 1 will test the effect of portion size on children's consumption of sweetened beverages; we hypothesize that serving large beverage portions will increase the amount of energy children consume from this food. Experiment 2 will test the effects of portion size on children's intake of fruits and vegetables (FV) affect intake whether such effects are moderated by children's FV preferences and; we hypothesize that serving large fruit and vegetable portions will produce increases in children's intake of these foods, particularly for children who like fruit and vegetables. Experiment 3 will evaluate how food energy density affects children's response to large portions; we hypothesize that large portions will have the greatest influence on children's energy consumption when foods are energy dense. Experiment 4 will begin to address perceptual mechanisms by which large portions affect children's eating.

| Slide 100 of 25 April 2007
Ibuprofen Effective for Acute Musculoskeletal Pain Relief in Children CME
News Author: Laurie Barclay, MDCME Author: Charles Vega, MD, FAAFP Disclosures
Release Date: March 13, 2007; Valid for credit through March 13, 2008
Credits Available
Physicians - maximum of 0.25 AMA PRA Category 1 Credit(s)™ for physicians;Family Physicians - up to 0.25 AAFP Prescribed credit(s) for physicians
March 13, 2007 — In a group of children randomly assigned to ibuprofen, acetaminophen, or codeine, ibuprofen was the most effective for treating the pain of acute musculoskeletal injuries, according to the results of a study reported in the March issue of Pediatrics.
"Our goal was to determine which of 3 analgesics, acetaminophen, ibuprofen, or codeine, given as a single dose, provides the most efficacious analgesia for children presenting to the emergency department with pain from acute musculoskeletal injuries," write Eric Clark, MD, from the University of Ottawa in Ontario, Canada, and colleagues. "Although there have been studies comparing the pain relief provided by different oral analgesics in children postoperatively, there are no published randomized, controlled trials examining the use of common oral pain medications for children with acute musculoskeletal injury in the ED [emergency department]."
This study enrolled 336 children age 6 to 17 years with pain from a musculoskeletal injury to the extremities, neck, and back that occurred in the preceding 48 hours before presentation in the emergency department. These children were randomized to receive a single oral dose of 15 mg/kg of acetaminophen, 10 mg/kg of ibuprofen, or 1 mg/kg of codeine. Children, parents, and evaluators were blinded to group assignment, and the main endpoint was change in pain from baseline to 60 minutes after treatment with study medication, measured with a visual analog scale.
Of 336 patients randomized, 300 were included in the analysis of the primary outcome (100 in the acetaminophen group, 100 in the ibuprofen group, and 100 in the codeine group). Age, sex, final diagnosis, previous analgesic given, and baseline pain score were similar in the 3 groups.
At 60 minutes, improvement in pain score was significantly greater in the ibuprofen group (mean decrease, 24 mm) than in the codeine group (mean decrease, 11 mm) and acetaminophen group (mean decrease, 12 mm). More patients in the ibuprofen group achieved adequate analgesia (visual analog scale, < 30 mm) at 60 minutes than in the other 2 groups.

| Slide 101 of 25 April 2007
HIV Pharmacology Workshop: The dangers of breaking up tablets for paediatric dosing
printer friendly versionsend to friendglossarycomment Yasmin Halima, Monday, May 01, 2006Further evidence that dividing adult Triomune tablets for use by children may result in under-dosing was presented last week at the HIV Pharmacology Workshop in Lisbon, and the workshop also heard the first bioequivalence data on a paediatric tablet formulation of Triomune, called Pedimune.
Triomune (a fixed dose combination of stavudine (d4T), lamuvdine (3TC) and nevirapine) is the cheapest regimen available in much of sub-Saharan Africa, and is commonly prescribed to adults. Attempts have been made to estimate doses for children by halving and quartering tablets, but it is unclear if these doses are correct.
A European-African study involving the Radboud University and Nijmegen University in the Netherlands, two African hospitals in Malawi and Zambia respectively and the UK Medical Research Council (MRC) was carried out. The aim of the study was to investigate whether Triomune tablets that are routinely divided for administration, deliver the same active ingredients, particularly in children who are malnourished.
Tablets are difficult to split, the drugs are not equally distributed and there are no formal recommendations on how to divide them with the distinct possibility of under-dosing.

| Slide 102 of 25 April 2007
Bioavailability study results for new paediatric tablets for oral suspension, and caution against splitting adult doses
Polly Clayden, HIV i-Base
All discussion concerning obstacles to paediatric scale up - both at this conference and to date - has highlighted the lack of easily stored, low cost, age appropriate antiretroviral formulations for children.
As an interim measure many programmes prescribe divided adult fixed dose combinations (FDCs) but this is not without problems, and can yield suboptimal levels of nevirapine, particularly in very young children (see below). Obviously FDCs for children will be a welcome development.

| Slide 103 of 25 April 2007
Paediatric FDCs
At the pharmacology (PK) workshop in Lisbon earlier this year, independent investigators presented bioavailability data for Indian generic manufacturer Cipla’s Pedimune Baby and Pedimune Junior FDC tablets of NVP, 3TC and d4T, which led them to conclude that it would be acceptable to begin testing PK and dosing requirements of these formulations in African children even though the formal bioequivalence study by Cipla has not yet been completed. [1, 2]
Another Indian generic company, Ranbaxy has developed two new paediatric formulations of tablets for oral suspension (TFOS) “designed to disintegrate quickly into a uniform suspension in small volume of liquid media like water”.
A poster from Singla and co-workers from Ranbaxy described the formulation development of Triviro-LNS kid (3TC 20mg /nevirapine 35mg/d4T 5mg) and Triviro-LNS kid DS (3TC40mg / nevirapine 70mg / d4T 10mg) – which will provide NIH recommended doses of the drugs for children weighing 9-31kg. [3]
And in an oral presentation Manish Vermer reported findings from the company’s bioavailability study of a single dose of the Triviro-LNS kids DS formulation compared to reference propriety liquid formulations. [4]
The investigators reported that the tablet has: a break line, “to enhance accuracy of dosing”; “a pleasant orange flavour” and requires no specific measuring device or refrigeration. Time to dispersion is 40 seconds in a small amount of water.
The bioavailability study was an open label, single dose crossover study conducted in 36 fasting HIV negative adult males.
The investigators reported that the geometric mean ratios (% Test/Reference) of log-transformed parameters of AUC, Cmax and 90% confidence intervals were within 80 -125% interval, see Table 1.
They wrote “Therefore the two treatments were considered to be similarly bioavailable and they concluded “Ranbaxy’s novel paediatric triple ARV TFOS could be used in place of individual liquid formulations.”

| Slide 104 of 25 April 2007
MedlinePlus related topics: Thyroid DiseasesGenetics Home Reference related topics: Thyroid Diseases
Study Type: InterventionalStudy Design: Treatment, Randomized, Open Label, Active Control, Crossover Assignment, Bio-equivalence Study
Official Title: Generic vs. Name-Brand Levothyroxine: Assessment of Bioequivalence Using TSH as a Marker in Children With Permanent Hypothyroidism
Further study details as provided by Children's Hospital Boston:
Primary Outcomes: Thyroid Stimulating Hormone MeasureExpected Total Enrollment: 40
Study start: June 2006; Expected completion: January 2008Last follow-up: January 2008; Data entry closure: January 2008
This study is an unblinded, randomized controlled cross-over study, which involves taking 2 different forms of levothyroxine sequentially over a 16 week period. Subjects will have a total of 3 visits over this time period. At the first visit, subjects are randomized to rec

| Slide 105 of 25 April 2007

| Slide 106 of 25 April 2007
Purpose
This is a randomized, double-blind, multi-centered study to compare 6 months of medical treatment with digoxin or propranolol in infants with SVT Background: SVT is the most common sustained arrhythmia of infancy. Neither digoxin nor propranolol has been evaluated for pediatric use in a controlled trial in the context of SVT, yet both medications are used frequently.
Specific aims of the study:
To determine whether propranolol and digoxin differ in the:
Incidence of recurrent SVT in infants after 6 months of treatment with propranolol or digoxin
Time to first recurrence of SVT in infants treated with propranolol or digoxin.
Incidence of adverse outcomes in infants treated with propranolol or digoxin.
Condition InterventionPhaseSupraventricular Tachycardia in Infants Drug: digoxin and propranololPhase IIIMedlinePlus consumer health information
Study Type: InterventionalStudy Design: Treatment, Randomized, Double-Blind, Active Control, Single Group Assignment, Bio-equivalence Study
Official Title: Multicenter Study of Antiarrhythmic Medications for Treatment of Infants With Supraventricular Tachycardia

| Slide 107 of 25 April 2007
Asthma and gastroesophageal reflux disease (GERD) are common disorders, which although are not usually lethal, both have high morbidity, and high healthcare costs.
Recent studies have demonstrated that asthma and GERD often co-exists, and that this co-existence is more frequent than just chance. Therefore, studies that characterize
associations between these conditions, and, help in the development of interventions will positively impact the outcomes of these patients, which are critically needed .
Subjects that participate in this study are required to be between the ages of 4-11 years old. This protocol proposes to enroll 50 children with asthma, on inhaled steroids who have poor asthma control, defined on the basis of frequent symptoms, excessive beta-agonists
use, or frequent asthma episodes .The purpose of this research study is to:
Determine, whether children with symptomatic, poorly controlled, asthma assigned to treatment with a PPI( Proton Pump Inhibitor), have fewer asthma episodes than similar
participants assigned to placebo for a similar duration of time Determine whether children treated with Lansoprazole ( i.e., proton pump inhibitor) : have a longer time to first exacerbation, have improved lung function, improved asthma symptom
scores, improved quality of life, decreased rescue inhaler use, or other asthma medications, reduced emergency room/urgent care/ physician office visits that are asthma
related .Determine whether a subgroup of symptomatic asthmatics, who show a greater benefit
from PPI’s, can be identified .

| Slide 108 of 25 April 2007
Ranbaxy presents bioequivalence data on two paediatric fixed dose triple combination tablets
printer friendly versionsend to friendglossarycomment Edwin J. Bernard, Thursday, August 17, 2006Two fixed dose triple combination water-dispersible tablets produced by generic manufacturer Ranbaxy providing half- and quarter-doses of nevirapine, lamivudine and stavudine for paediatric use are bioequivalent to their proprietrary liquid formulations in adults, according to a study presented to the Sixteenth International AIDS Conference in Toronto on August 16th. The two formulations have already been approved by the Indian government, and have been submitted to the World Health Organisation (WHO) for inclusion on their pre-qualification list.
Several recent initiatives have begun to address the issue of lack of paediatric formulations in low-income countries, first highlighted two years ago at the Fifteenth International AIDS Conference in Bangkok by Médecins Sans Frontières (MSF) director Daniel Berman.

| Slide 109 of 25 April 2007

| Slide 110 of 25 April 2007
ConclusionConclusion
A new way for the future and a long way to solve all the issues….

| Slide 111 of 25 April 2007
Further referencesFurther references
Yu LX et al. Biopharmaceutics Classification System: The scientific basis for biowaiver extensions. Pharm Res 2002 19(7).
Polli J.E et al. Summary Workshop Report: Biopharmaceutics Classification System- Implementation Challenges and Extension Opportunities. J Pharm Sci 2004 93(6)
Vogelpoel H. et al. Biowaiver monographs for IR solid oral dosage forms based on BCS literature data: Verapamil HCl, Propranolon HCL and Atenolol. 2004 J Pharm. Sci. 93(8)
Lindenberg et al.: Classification of orally administered drugs on the WHO model list of essential medicines according to the biopharmaceutics classification system. Eur. J. Pharm. Biopharm. 58: 265-278, 2004