
+ Principles of Assessment. + Neuropsychological Assessment of Mental State Any patient who has a...
52
+ Principles of Assessment
-
Upload
dustin-austin -
Category
Documents
-
view
213 -
download
0
Transcript of + Principles of Assessment. + Neuropsychological Assessment of Mental State Any patient who has a...

+
Principles of Assessment

+Neuropsychological
Assessment of Mental State Any patient who has a known brain lesion from tumor,
trauma, or cerebrovascular accident, as well as any with suspected psychiatric and organic disease should have a screening mental status evaluation to document any cognitive or emotional changes.
Many patients who have mild aphasia or memory deficits after craniotomy, who have increased irritability and decreased ability to concentrate after head trauma, or who have marked emotional lability following infectious neurologic disease are released from the hospital without recognition of these cognitive and emotional deficits.

+Neuropsychological
Assessment of Mental State
Such patients frequently become emotionally frustrated, have difficulty with social readjustment, and are unable to carry out the demands of home and vocation.
Early recognition of the neurobehavioral sequelae of a known neurologic disorder will help us explain the totality of the patient’s disability to family and possibly employers.
Mental status screening is extremely important in patients who initially present with or who are brought to us by their families with vague behavioral complaints of memory problems, difficulty in concentration, declining interest in family or work to determine the possibility of organic brain disease.

+Neuropsychological
Assessment of Mental State Bedside or office mental status examination is very
effective in diagnosing organic disease and for evaluating major areas of deficit.
By its nature, the examination is qualitative, and is not meant to replace standardized quantitative testing for evaluating subtle deficits, planning for comprehensive rehabilitative efforts, and assessing improvements in performance.
Mental status testing should be performed in an orderly way, with assessment of basic processes, such as the level of consciousness, attention, and vigilance first, and the higher-level functions such as abstract reasoning and special cognitive functions tested last.

+Neuropsychological
Assessment of Mental State The goal of the mental status examination is to
determine: Level of consciousness; Orientation to person, place, and time; Attention span; Concentration; Memory; Insight; Judgment; and Ability to calculate
Common mental status assessment instruments are the Mini-Mental Status Examination (MMSE) and the St. Louis University Mental Status Examination(SLUMS).

+Neuropsychological
Assessment of Mental State The goal of the mental status examination is to
determine: Level of consciousness; Orientation to person, place, and time; Attention span; Concentration; Memory; Insight; Judgment; and Ability to calculate
Common mental status assessment instruments are the Mini-Mental Status Examination (MMSE) and the St. Louis University Mental Status Examination(SLUMS).

+MMSE
The Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 2097) is an 11 item tool that can be used to systematically and thoroughly assess mental status in five areas of cognitive function: orientation, registration, attention and calculation, recall, and language.
The maximum score is 30; a score of 23 or lower is indicative of cognitive impairment.
The MMSE takes only 5-10 minutes to administer and is therefore practical to use repeatedly and routinely.

+SLUMS
The MMSE is commonly used as a screening tool to detect dementia.
However, it performs poorly in identifying persons with mild neurocognitive disorder.
The SLUMS consists of 11 items that screen for aspects of cognition that include orientation, short-term memory, calculations, naming of animals, clock drawing, and recognition of geometric figures.
It is free and takes about seven minutes to administer the SLUMS.

+SLUMS
Scores range from 0 to 30, with scores of 27-30 considered normal in a person with a high school education.
Scores between 21 and 26 suggest a mild cognitive disorder, and scores between 0 and 20 indicate dementia.
The SLUMS is superior to the MMSE in identifying people with more mild cognitive problems that don't yet rise to the level of dementia.

+Case History/Interview Focus
Assessment techniques used across disorders of communication include case history, hearing screening, interview, orofacial examination, and speech and language sampling.
Using the patient’s medical chart and interviews with family members, obtain information on the onset and recovery from stroke or other clinical condition.
Consider the results of medical neurodiagnostic techniques.

+Case History/Interview Focus
Consider the results of available psychological, cognitive, physical therapy, and related assessment information.
Consider the client’s current medical condition and prognosis.
Collect biographical information, including education, occupation, literacy, and premorbid intellectual and communication skills, as well as current family communication patterns.

+Ethnocultural Considertions
Factors related in an individual’s cultural, ethnic, social, and personal variables may affect assessment of communication disorders.
During the interview process, explore:o how the client’s culture views communication and
communication disorders;o how the client’s culture views the etiology, effects,
and social significance of neurological disorders; o how the family views assessment and treatment and
what expectations they have of clinical services; and

+Ethnocultural Considertions
o the extent to which a member of a cultural group is different from the majority group (e.g., an African-American who does not speak a Black English dialect).
Select standardized tests that have, in their standardization process, sampled the ethnocultural group to which the client belongs.
If culturally appropriate standardized tests are not available, design client-specific assessment procedures.
If client is bilingual/multilingual, use trained interpreters in the assessment process and determine whether a communication disorder exists in the primary language, the secondary language, or both.

+Goals of Assessment for Focal
Disorders
Following a mental status examination, the goals of speech and language assessment will depend upon the period of time since onset of the neurological insult and the questions that need to be answered.
In early stages (acute) following neurological onset, the goal of assessment is to make a brief assessment of language skills.
Once the patient’s physical condition improves and stabilizes medically, the goal is to make a more thorough assessment of communication skills.

+Goals of Assessment for Focal
Disorders
If one suspects aphasia, assess expressive, receptive, and gestural communication, in order to identify initial treatment targets.
If one suspects a right hemisphere disorder, evaluate for perceptual and attentional deficits, as well as assess communication disorders associated with right hemisphere syndrome, in order to support or justify a diagnosis of right hemisphere disorder and to identify initial treatment targets.

+Assessing Specific
Communication Skills
Specific communication skills can be assessed through clinician-assembled diagnostic protocols, or through administration of standardized tests of aphasia.
When selecting a standardized test, consider the one that is appropriate for the client, practical, or preferred because of your experience with it.
Standardized tests of aphasia and/or client-specific assessment protocols usually have a common/standard set of procedures for assessing receptive and expressive language, as well as associated motor speech disorders.

+Assessing Specific
Communication Skills
When selecting or designing an assessment protocol to use with left hemisphere focal disorders, consider the following:oObtain a language (discourse) sample.oAssess auditory comprehension deficits, moving from simple to complex tasks.
oAssess verbal fluency, including phrase length, speech rate, rhythm and intonation, grammaticality, speech articulation.
oAssess repetition skills at single word, multisyllabic, and phrase/sentence levels.

+Assessing Specific
Communication Skills
o Assess word finding and naming skills.o Assess the use of sentence structures and
types, including morphological features.o Assess understanding or usage of gestures.o Assess reading problems, including
comprehension of silently read material and oral reading.
o Assess writing problems, including graphomotor skills and written expression.
o Assess pragmatic communication problems.

+Assessing Specific
Communication Skills
When selecting or designing an assessment protocol to use with right hemisphere focal disorders, consider the following:oleft-sided neglect and attentional deficits;odisorientation;oconstructional impairmentoaffective deficits;odenial of illness;oimpaired inference;oimpaired reasoning, planning, organizing, and problem-solving skills;

+Assessing Specific
Communication Skills
o problems in logical reasoning; ando other behavioral deficits;
In terms of communication ability, take a conversational speech sample and assess:
o Prosodic problems;o Inappropriate and anomalous speech;o Problems in distinguishing significant from
irrelevant information;o Problems in comprehending applied meaning;o Problems in integrating information;o Problems in speech pragmatics;

+Assessing Specific
Communication Skills
oAuditory comprehension of language;oWord-retrieval problems;oReading and writing problems; and oMotor speech disorders
Analyze the results of your assessment to obtain the strengths and limitations of the client.
Summarize the communication deficits. To diagnose aphasia, language disturbance should be due to recently acquired cerebral injury, except in some rare cases of gradual onset.

+Assessing Specific
Communication Skills
Language disturbances should outweigh any intellectual deficits observed.
To diagnose right hemisphere disorder, history and medical evidence should be consistent with right hemisphere injury, especially strokes, tumors, or head trauma.
In some individuals with aphasia and RHD, a concomitant cognitive problem exists.
Administer the Cognitive Linguistic Quick Test (Helm-Estabrooks, 2001) and compare linguistic and non-linguistic performance.

+Aphasia Versus Normal Language
Aphasia Normal Language
Positive hx of stroke, tumor, and/or other central neuropathology
Negative hx of central neuropathology.
Prior hx of normal language; deterioration in language skills.
Prior hx of normal (limited) language; no evidence of deterioration in language skills.
Lack of education does not explain the problems.
Lack of education could explain the problems.
Level of literacy does not explain the problem.
Level of literacy could explain the problem.
Current environment could not explain the problem.
Current environment could explain the problem.
Sudden onset. No apparent onset or lifelong problem.

+Aphasia Versus Schizophrenia
Aphasia Schizophrenia
Sudden onset. Gradual onset.Late onset (adult or old age). Early onset (adolescence or early
adulthood).Not a psychotic disorder; no hx of psychiatric disturbances.
A psychotic disorder; a hx of psychiatric disturbances.
Due to a general medical condition (e.g., cerebral infarct).
Not due to a general medical condition.
No perceptual disorders such as hallucinations.
Perceptual disorders, especially auditory hallucinations.
No confabulation; generally relevant. Confabulation; typically irrelevant.No evidence of disorganized speech. Disorganized speech.

+Aphasia vs. Schizophrenia (Cont.)
Aphasia Schizophrenia
Deficits in auditory comprehension. No deficits in auditory comprehension (may be inattentive).
Reading and writing affected. Reading and writing may not be affected.Appropriate emotional responses. Lack of emotional expression and
inappropriate/incongruent emotional responses.
Social behavior, personality, and general behavior not affected, except by motor limitations.
Social behavior, personal hygiene, and general behavior grossly disorganized, but not by motor limitations.
Appropriate sexual behavior. Inappropriate sexual behavior.

+Aphasia Versus RHD
Aphasia Right Hemisphere Disorder
Significant/dominant problems in naming, fluency, auditory comprehension, reading, and writing.
Only mild problems in naming, fluency, auditory comprehension, reading and writing.
No left-sided neglect. Left-sided neglect.No denial of illness. Denial of illness.Speech is generally relevant. Speech is often irrelevant, excessive,
rambling.Generally normal affect. Often lack of affect.Intact recognition of familiar faces. Possible impaired recognition of familiar
faces.Simplification of drawings. Rotation and left-sided neglect.

+Aphasia Versus RHD (Cont.)
Aphasia Right Hemisphere Disorder
No significant prosodic defect. Significant prosodic defect.Appropriate humor. Inappropriate humor.May retell the essence of story. May retell only nonessential, isolated
details (no integration).May understand implied meaning. Understands only literal meanings.Pragmatic impairments less striking. Pragmatic impairments more striking (eye
contact, topic maintenance, etc.).Communication is often good in spite of limited language skills.
Communication is very poor, in spite of good language skills.
Pure linguistic deficits are dominant. Pure linguistic deficits are not dominant.

+Aphasia Versus Apraxia of Speech
Aphasia without Apraxia Apraxia without AphasiaNeurogenic language problem. Neurogenic speech problem.
Trial and error, groping articulatory movements not significant.
Trial and error, grouping articulatory movements are significant.
Misarticulations less variable, more consistent. Misarticulations more variable, more inconsistent.
Some impairment in auditory comprehension. Generally no impairment in auditory comprehension.
Prosodic problems not dominant. Prosodic problems dominant.
Little difficulty initiating utterances. Obvious difficulty initiating utterances.
Omission of functors. Little tendency to omit functors.
Word-finding problems. No word-finding problems.
Limb/oral apraxia not dominant. Concomitant limb/oral apraxia.

+Aphasia Versus Dysarthria
Aphasia without Dysarthria Dysarthria without AphasiaNeurogenic language problem. Neurogenic speech problem.
Language problems are not due to muscle weakness.
Speech problems are due to muscle weakness, spasticity, rigidity.
No consistent misarticulations. Consistent misarticulations.
Intelligibility of speech not clearly related to speech rate.
Intelligibility clearly related to speech rate.
No respiratory problems associated with speech production.
Respiratory problems associated with speech production.
No significant phonatory problems. Possibly significant phonatory problems.
No significant resonatory disorders. Significant resonatory disorders.
Prosodic disorders not dominant. Prosodic disorder may be dominant.
No significant abnormal stress. Possibly significant abnormal stress.

+Goals of Assessment in Dementia
In general, the goals of assessment with dementia include: assessing language, cognitive, memory, and
visuospatial skills; assessing changes in behavior and personality; identifying the strengths and limitations of the
patient with a view to develop an intervention or management plan for the patient and family; and
identifying the stage of dementia progression.
Identifying advanced stage dementia is not as challenging as identifying early and mild forms of dementia.

+Goals of Assessment in Dementia Automatic tasks, such as pointing to named pictures and
reciting alphabets and days of the week are not especially diagnostic of mild dementia.
Syntactic disturbances are not evident in mild dementia, except in the case of multi-infarct dementia and dementia associated with Pick’s disease.
Articulation and phonological skills are not diagnostic of early dementia and are retained until the advanced stage when dementia is obvious.
Sentence repetition skills are not diagnostic of early dementia as they are preserved even when the patient cannot comprehend the meaning of repeated sentences.

+Goals of Assessment in Dementia Creative thinking and abstract reasoning tasks have
diagnostic value (e.g., verbal description, story telling, verbal fluency).
Language assessment alone will not determine the diagnosis; deterioration in memory, visuospatial skills, and general intellect also should be demonstrated.
Make a mental status examination.
Assess reasoning and event planning skills (knowledge of schemata) by asking the patient to describe how s/he would:

+Goals of Assessment in Dementia
o Plan a birthday party;o Plan a summer vacation, camping trip, or picnic;o Get an airline ticket; oro Obtain a doctor’s appointment.
Assess memory skills.
Assess drawing skills;
Assess abstract reasoning.

+Goals of Assessment in Dementia When assessing language and communication skills, assess:o Vocabulary—note that the PPVT is sensitive to early
phases of dementia;o Verbal description skills;o Story telling skills;o Verbal fluency or generative naming tasks;o Pantomime expression;o Reading comprehension; ando Pragmatic language skills.
There are several standardized tests that can be use in part or as a whole evaluate intellectual integrity and cognitive processing skills.

+Goals of Assessment in Dementia
Test PurposeArizona Battery for Communication Disorders of Dementia
To assess dementia through 14 subtests and screen it with four subtests
Benton Revised Visual Retention Test
To assess visual memory with figural recall
Brief Cognitive Rating Scale To assess cognitive decline due to any reason
Clinical Dementia Rating Scale
To rate dementia on a 5-point scale

+Goals of Assessment in Dementia
Test PurposeDiscourse Abilities Profile To assess various forms of
discourse during conversation with the client; between conversation with client/caregivers
Global Deterioration Scale To rate dementia on a 7-point rating scale
Mini-Mental State Examination To assess mental status
Wechsler Memory Scale-Revised To assess various memory functions

+Cognitive & Communicative
Appraisal
Once the informal/formal assessment protocol has been completed, integrate the clinical assessment data with those of the case history information and develop a picture of the client’s strengths and weaknesses.
Further differentiate dementia from aphasia, language of confusion, depression, right hemisphere syndrome.
Develop a summary statement of the significant findings.
Generally, impairment should be documented in (1) language; (2) memory; (3) visuospatial skills; (4) emotion or personality; and (5) cognition.
Minimally, three of the five listed functions should show impairment to diagnose dementia.

+Cognitive & Communicative
Appraisal
Definite diagnosis is possible only with autopsic or biopsic evidence of histopathology.
Distinguish among cortical dementias caused by Alzheimer’s disease or Pick’s disease.
Distinguish among mixed dementias caused by Lewy Body disease or multi-infarct dementia.
Distinguish among subcortical dementias caused by Huntington’s disease, Parkinson’s disease, Wilson’s disease, or supranuclear palsy.
+Cognitive & Communicative
Appraisal Generative naming is a more sensitive early sign
of dementia than is confrontation naming.
Early stage dementia has relatively intact phonological and syntactic skills.
Patients with fluent aphasia are more likely to be confused with dementia than are those with nonfluent aphasia.
Aphasia and dementia may coexist; an aphasic patient may develop a neurological disease resulting in dementia.
A patient with dementia may have a stroke resulting in aphasia.

+Dementia Versus Aphasia
Dementia AphasiaOnset mostly is slow Onset mostly is suddenBilateral brain damage Damage in left hemisphereDiffuse brain damage Focal brain damageMay be moody, withdrawn, agitated Mood usually appropriate, though
depressed or frustrated at timeCognition impaired; language skills intact until later stages
Impaired language, but generally intact cognition
Memory is impaired, often severely Memory is typically intact

+Dementia Versus Aphasia (Cont.)
Dementia AphasiaBehavior is often irrelevant, socially inappropriate, disorganized
Behavior generally relevant, socially appropriate, organized
Confused and disoriented to time and space
Alert and oriented to time and space
Disorientation to self, later stage No disorientation to selfProgression of deterioration from semantic to syntactic to phonological performance
Semantic, syntactic, and phonologic performance simultaneously impaired
Fluent Fluent or nonfluent

+Dementia Versus Aphasia (Cont.)
Dementia AphasiaPoor performance on spatial and verbal recognition tasks
Better performance on spatial and verbal recognition tasks
Poor story retelling skills Better story retelling skillsPoor description of common objects
Better description of common objects
Poor silent reading comprehension Better silent reading comprehension
Poor pantomimic expression Better pantomimic expression

+Dementia Versus Language of
Confusion
Dementia Language of ConfusionDegenerative disease TBI or toxic/metabolic disturbanceReduced range and variety of word usage
No significant problem with word usage
Slow onset Abrupt onsetDisorientation to time, place, and person only in advanced stages
Disoriented to time, place and person
Progressive worsening of symptoms
More rapid, positive changes in symptoms

+Dementia Versus Depression
Dementia Depression (Pseudodementia)Imprecise onset date More precise onset dateFamily members do not know about symptoms
Family members know about symptoms
Slow progression of symptoms Rapid progression of symptomsNo hx of psychiatric problems Hx of psychiatric problemsDo not complain of cognitive problems
Complain of cognitive problems in detail
Try to conceal their problems. Highlight their disability, failure, sense of distress.

+Dementia vs. Depression (Cont.)
Dementia Depression (Pseudodementia)Struggle to perform Make no or little effort to perform even
simple tasksSocial skills preserved until late stages Loss of social skillsAttentional deficits and poor concentration
No attentional deficits; good concentration
More severe loss for recent than remote events
Same degree memory loss for recent and remote events
Generalized memory problems Selective memory problemsConsistent difficulty in performing the same task
Variability in performing the same tasks

+Dementia Versus RH Syndrome
Dementia Right Hemisphere SyndromeSignificant problems in naming, especially generative naming
Only mild problems in naming, reading, and writing
Significant problems in auditory comprehension
Mild problems in auditory comprehension
No left-sided neglect Left-sided neglect
Mild prosodic defects Significant prosodic defect
Retell stories without context or location Retells only nonessential, isolated story details
Mild pragmatic impairments to later stages Striking pragmatic impairments
Significant linguistic deficits (except for syntactic and phonological skills until late stages)
Pure linguistic deficits are not common

+Differentiating Cortical Dementias
Alzheimer’s Disease Pick’s DiseaseGradual onset Gradual onset
Diffuse damage due to senile plaques, neurofibrillary tangles, granulovacuolar degeneration
Atrophy in frontal and temporal regions; Pick’s bodies
Impairment in semantic and pragmatic language functions in early stages
Impaired rate and prosody due to slow deliberate speech; naming problems; syntactic difficulties; auditory comprehension problems
Impaired memory but worse for remote events Impaired memory but worse for recent events
Willing to perform; tries to perform Apathetic; shows emotional lability
Generally normal motor functions until late stages
Impaired motor function in later stages
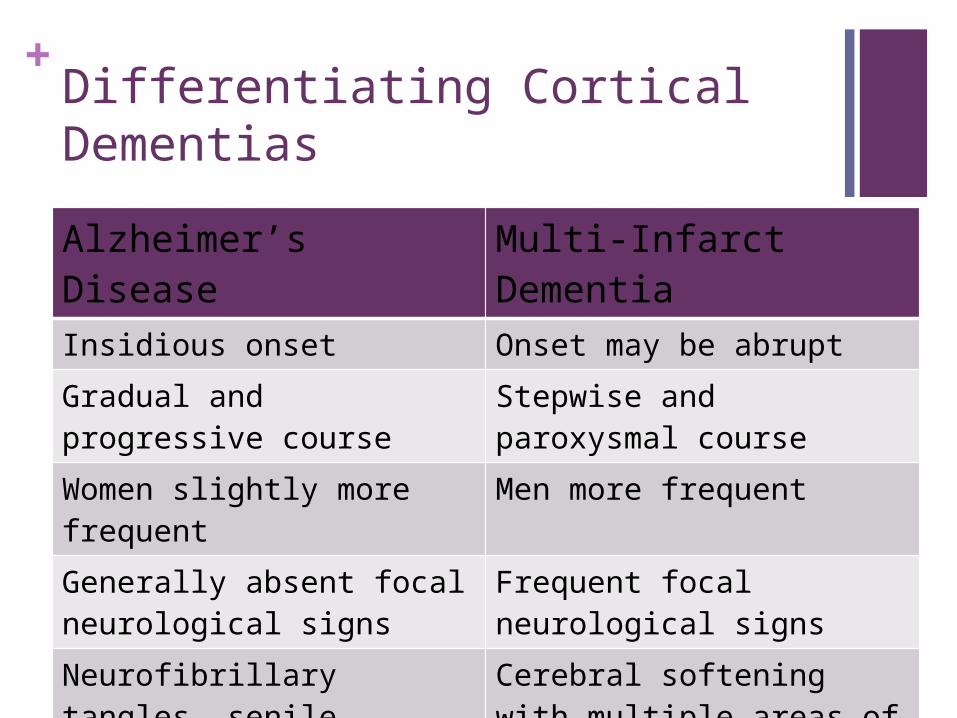
+Differentiating Cortical Dementias
Alzheimer’s Disease Multi-Infarct DementiaInsidious onset Onset may be abruptGradual and progressive course Stepwise and paroxysmal courseWomen slightly more frequent Men more frequentGenerally absent focal neurological signs
Frequent focal neurological signs
Neurofibrillary tangles, senile plaques, granulovacuolar degeneration
Cerebral softening with multiple areas of infarction; cardiovascular plaques; arteriosclerosis

+Alzheimer’s vs. VD
Alzheimer’s Disease Multi-Infarct DementiaIncreased family incidence of Down’s syndrome and leukemia
Strokes and other cerebral vascular accidents; cardiac pathologies; hypertension; TIAs; diabetes mellitus; obesity.
Impairment of semantic and pragmatic language functions in early stages; syntactic and phonological skills preserved until later stages
Aphasia and varied symptom complex depending on extent and location of neuropathology
Impaired remote memory Varied memory impairment

+Differentiating Mixed Dementias
CJD MIDOnset gradual or sudden Onset is suddenViral infection; cortical degeneration and encephalopathy
Vascular pathology; generalized cortical damage from multiple strokes.
Rapidly progressive Stepwise in progressionAphasia,apraxia, agnosia, and eventually mutism
Aphasia of varied symptomatology
Forgetfulness Varied memory impairmentApathy Variable emotional responsesRigidity; myoclonus; sensory impairments May have physical/sensory symptoms

+Differentiating Subcortical
Dementias
Huntington’s Disease
Parkinson’s Disease
Wilson’s Disease
Supranuclear Palsy
Sporadic onset Insidious onset Gradual onset Gradual onsetGenetic cases Degenerative
disease of CNSExcessive cooper in brain and liver
Substantia nigra Loss of Golgi cells in corpus striatum
Basal ganglia Reticular formation, thalamus, or hypothalamus
Shuffling and jerky gait; chorea
Tremor, rigidity, slowness, bradykinesia, postural instability
Tremor, rigidity, slowness, bradykinesia, ataxia, dysphagia
Dystonia, rigidity of head/neck, retracted head position

+Differentiating Subcortical
Dementias
Huntington’s Disease
Parkinson’s Disease
Wilson’s Disease
Supranuclear Palsy
DepressionSignificant language impairment
Significant speech impairment
Inaudible speech
Dysarthria Dysarthria—weak, breathy voice
Dysarthria—irregular articulatory breakdown; hypernasality
Dysarthria—harsh sounds
Intervals of inappropriate silence
Abnormal pitch and loudness
Intervals of inappropriate silence
















![The Practice of Neuropsychological Assessment - … · rated into the neuropsychological test canon ... Poppelreuter, 1990 [1917]; W.R. Russell ... 1 THE PRACTICE OF NEUROPSYCHOLOGICAL](https://static.fdocuments.in/doc/165x107/5b9c7f2609d3f272468cc5a2/the-practice-of-neuropsychological-assessment-rated-into-the-neuropsychological.jpg)

