· Lecture 33& 34 : Specimen collection and processing -1 ط Blood specimen types ط Venipuncture,...
30
· Lecture 33& 34 : Specimen collection and processing -1 طBlood specimen types طVenipuncture , procedure, precautions طPediatric venipuncture طSkin puncture, arterial puncture B3 39-50; C4 40 - 2
-
Upload
dion-fricker -
Category
Documents
-
view
260 -
download
3
Transcript of · Lecture 33& 34 : Specimen collection and processing -1 ط Blood specimen types ط Venipuncture,...

· Lecture 33& 34 : Specimen collection and processing -1Blood specimen types طVenipuncture , procedure, precautions طPediatric venipuncture طSkin puncture, arterial puncture ط B3 39-50; C4 40 - 2

IntroductionProper patient identification, correct equipment, adequate knowledge
(physiological & environmental factors)Proper collection (sample type, timely), transport, processing, analysis,
reportingPrevious chain is critical in providing most accurate clinical picture
(weakest link)Added investment of time & effort for patients care & management of
specific groupPediatric, obese, elderly, ICU, women?
Blood Specimen Types:Blood is most common specimen (Whole, serum, plasma)Blood can be obtained from veins, arteries, capillaries1. Arterial blood is commonly used for blood gases & pH2. Venous blood content varies depending on metabolic activity of tissue (time / site)3. Capillaries (veins & arteries)
Blood Specimen Types:1. Arterial blood is commonly used for blood gases & pHO2 is the largest differenceReflects the respiratory & metabolic statusOthers are protein, glucose, ammoniaLimited to some conditionsCollected & performed by trained personnel

Blood Specimen Types:2. Venous blood content varies depending on metabolic activity of tissue (time / site)Timing & site of collection are criticalObtained by venipunctureInstitute standardize collection, location, patient positioning, tourniquets

Blood Specimen Types:3. Capillaries (veins & arteries)Obtained by skin puncture Similar to venipuncture: high glucose, low K, total protein, Ca++Also contain intracellular & tissue fluidsUsed if venous is not accessible:Burns, chemotherapy, difficult veins (obese, elderly), risk of collapse (infants)Warming of site causes increase blood flow=> lead to vasodilation => result in arterialization of capillariesExcessive squeezing result in increase of K

Venipuncture1. evacuated-tube (vacutainer)Sample is completely contained toreduce risk of outside contaminantreduce hazards on the collector2. Syringe collectionnecessary when patient has fragile or damage veins3. Butter-fly infusionmore expensive but convenient when both vacutainer tubes & syringe
collected at the same timeused mostly on pediatric patients, difficult veins
TourniquetBelt or rubber or tubing used to apply venous pressureNO prolonged pressureFor convenient & comfortable collection

NeedlesBore size referred as gaugeLarger needles (18 gauge) used for blood donorsSmaller needles (21-22) used in routine collectionSmallest needles (23-25) used with butterfly infusion, could cause hemolysis1. single-sample needle: collecting with a syringe2. multiple-sample needle:allow tube change without blood leakage (vacutainers)plastic sleeves with stopper: differ is size depending on manufacturer

TubesColour-coded stopper indicating additive present preservatives, anticoagulants, accelerators, plain

Others1. Alcohol pads:to sterile site of punctureiodine used for blood
culturing2. Gauze:can use folded cotton
gauze3. Tape or adhesive
bandageavoid in under 3 years
old
site of venipunctureantecubical fossa most common, arm (median cubical vein)other sites are acceptable: hand, ankle, footavoid collecting from: hematomas, scarring, previous puncture, mastectomy side, IV fluid site
Procedure of venipunctureFrom 1 to 20 on page 49

Pediatric venipunctureHazard include: cardiac arrest, hemorrhage, venous thrombosis, arterispams, tissue damage, infectionUse butterfly (21-23 gauge), 3ml syringe (tube)Collect only form superficial veins, secure arm, no bandage for under 3 years
Precautions during venipunctureFainting, nausea, vomiting STOP immediatelyHead lowered, cold compression, ammonia, physician
Skin PunctureBlood is brought to the surface of the skin by applying pressure to the site
(infants)Alcohol pads used to sterileLancet with controlled depth (2.4mm) to avoid abscess, bruises, bone
damage.. Microcollection Tubes (additives are powder, freeze dried)Silican separator gel (separate liquid from cell components)Heel warmer, no more than 42ºC

Site of skinpunctureFinger: palmer surface, 3-4rd ring fingerHeel: middle of the large toe to heel

Procedure of skinpunctureFrom 1 to 17 on page 53-54

· Lecture 35& 36 : Specimen collection and processing-2Anticoagulants : mechanisms and uses طPreservation and transport ط,Factors affecting specimen collection, Sources of error ط B3 50-58; C4 40 - 2
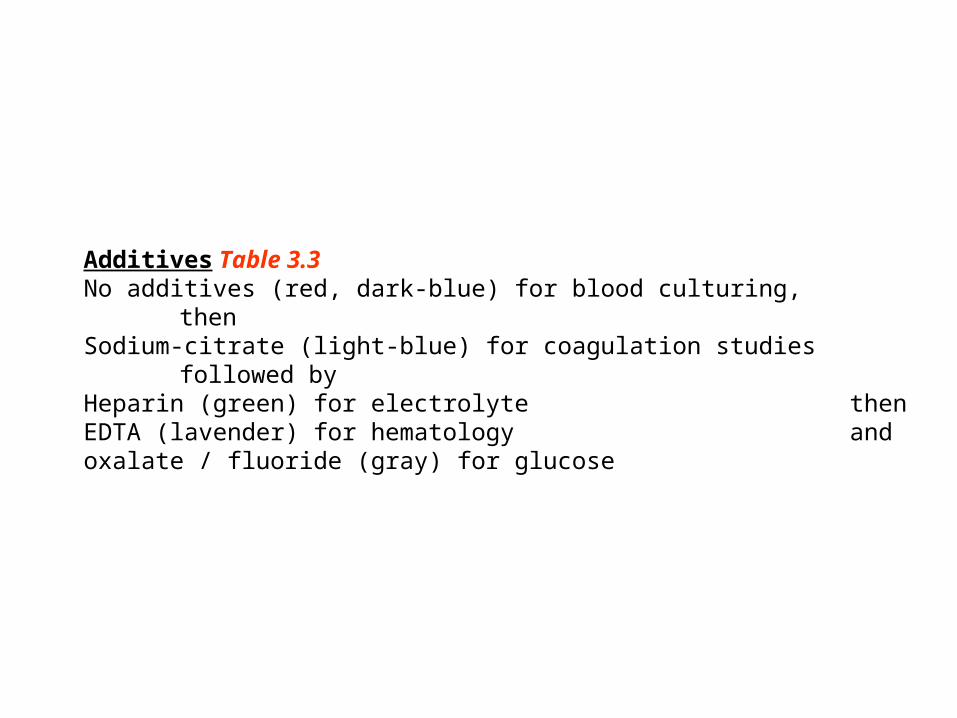
Additives Table 3.3No additives (red, dark-blue) for blood culturing, thenSodium-citrate (light-blue) for coagulation studies followed byHeparin (green) for electrolyte thenEDTA (lavender) for hematology andoxalate / fluoride (gray) for glucose

Specimen TransportUpon receiving in the lab, information should be matched and read correctly and acceptedThen sorted as to type of test and distributed to the lab unitAs soon as collected & quick as possible if no metabolic inhibitors presentAvoid common problems as hemolysisPrimary & secondary leak-proof containersIce to maintain integrity of analytesRemove serum within 1hr of centrifugation & centrifuge max 60 min after collectionMaintained in upright position, to promote clot & reduce hemolysisTemp 23-25ºC preferredPersonnel aware of handling requirement (cart, agitation, delay)Some require chilling to inhibit metabolism (tube)Certain tests require avoiding light (dark tube)
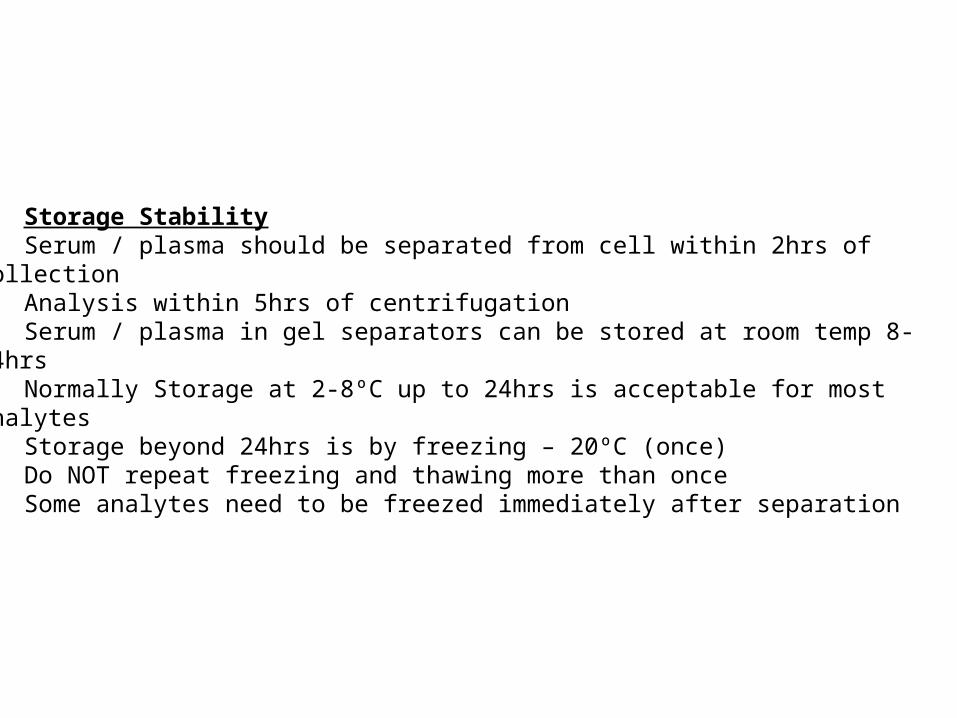
Storage StabilitySerum / plasma should be separated from cell within 2hrs of
collectionAnalysis within 5hrs of centrifugationSerum / plasma in gel separators can be stored at room temp 8-
24hrsNormally Storage at 2-8ºC up to 24hrs is acceptable for most
analytesStorage beyond 24hrs is by freezing – 20ºC (once)Do NOT repeat freezing and thawing more than onceSome analytes need to be freezed immediately after separation

Factors affecting specimen Table 3.1Timing:Best time is early morning (basal state)Time-intervals may be desired to observe metabolic process as glucose
tolerance and serum iron and also in therapeutic drug monitoringDiet:physicians must not if diet restriction is require to phlebotomistFasting Specimen: diet high in protein, glucose, saturated & unsaturated FA,
caffeine, serotoninsExercise:Moderate exercise can affect certain valuesStress:Emotions may falsely elevate white blood cellsPasture:Body diurnal rythms and pasture (sitting or laying)Hemolysis & Tourniquet** For forensic collection (law & medicine) in the presence of officer

Sources of error in venipuctureTable 3.5Sources of error in venipuctureTable 3.6

Other body fluids1. Cerebral Spinal Fluid:Obtained by lumber punctureFor glucose, total & specific protein determination, pH, CO2, bicarbonate2. Paracentess Fluid (pleural, pericardial, peritoneal):Collected by aspiration of siteFor specific gravity, protein, LDH determinationCollect blood sample in conjunction3. Amniotic Fluid:Obtained by aspiration of fetus amniotic sacFor fetal lung maturity, congenital diseases, hemolytic anemia, neural tube
defect, gestational age4. Urine:
A. Random (first void): for protein, glucose, specific gravity, osomlility,
Dark-colored contained for some test (e.g. bilirubin)
B. Timed (12-24hrs/befor or after a meal):Low electrolyte, catecholamine in morning
then peak at noonPreservatives (acid/base/refrigeration) used
in certain analytes and bact. growth