بسم الله الرحمن الرحيم Kidney Transplantation Dr. Anmar Nassir, FRCS(C) Canadian...
111
-
date post
20-Dec-2015 -
Category
Documents
-
view
221 -
download
1
Transcript of بسم الله الرحمن الرحيم Kidney Transplantation Dr. Anmar Nassir, FRCS(C) Canadian...

بسم الله الرحمن الرحيمبسم الله الرحمن الرحيم

Kidney Transplantation
Dr. Anmar Nassir, FRCS(C)
Canadian board in General Urology
Fellowship in Andrology (U of Ottawa)
Fellowship in EndoUrology and Laparoscopy (McMaster Univ)
Assisstent Prof Umm Al-Qura
Consultant Urology King Faisal Specialist Hospital

Kidney Transplantation: Objectives
• Why transplantation? • Types of transplantations• Assessment of transplant recipient and donor• Transplant immunology • Immunosuppressants • Complications• New advances in transplantation • Challenges

ESRD: Incidence PMP
61
98
212
139
0
50
100
150
200
250
Australia Canada USA KSA
1992
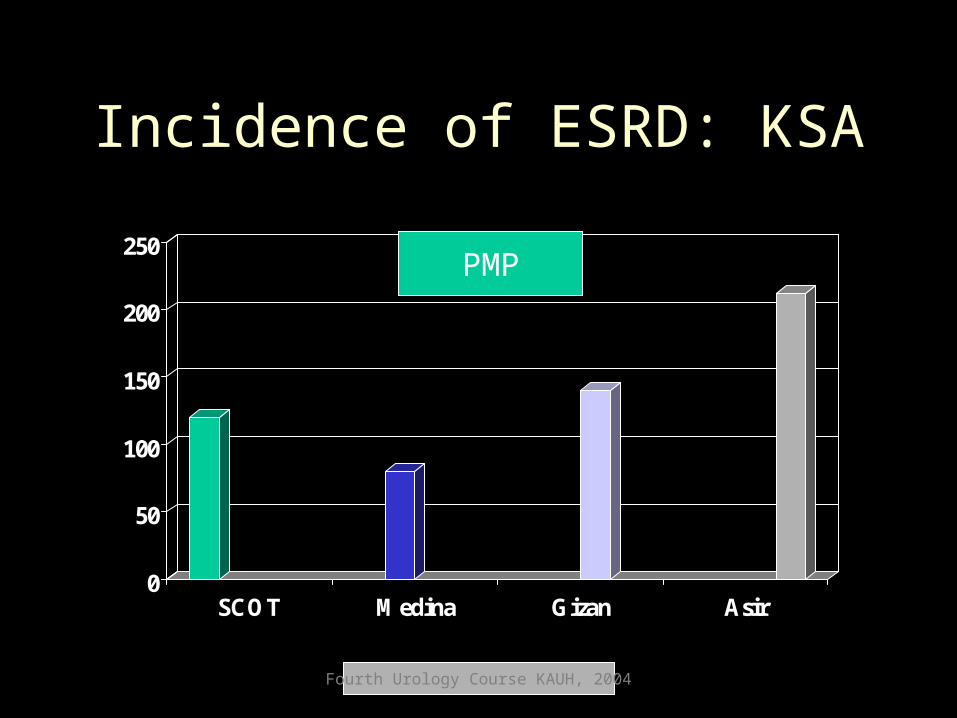
Incidence of ESRD: KSA
0
50
100
150
200
250
SCOT Medina Gizan Asir
PMP
Fourth Urology Course KAUH, 2004
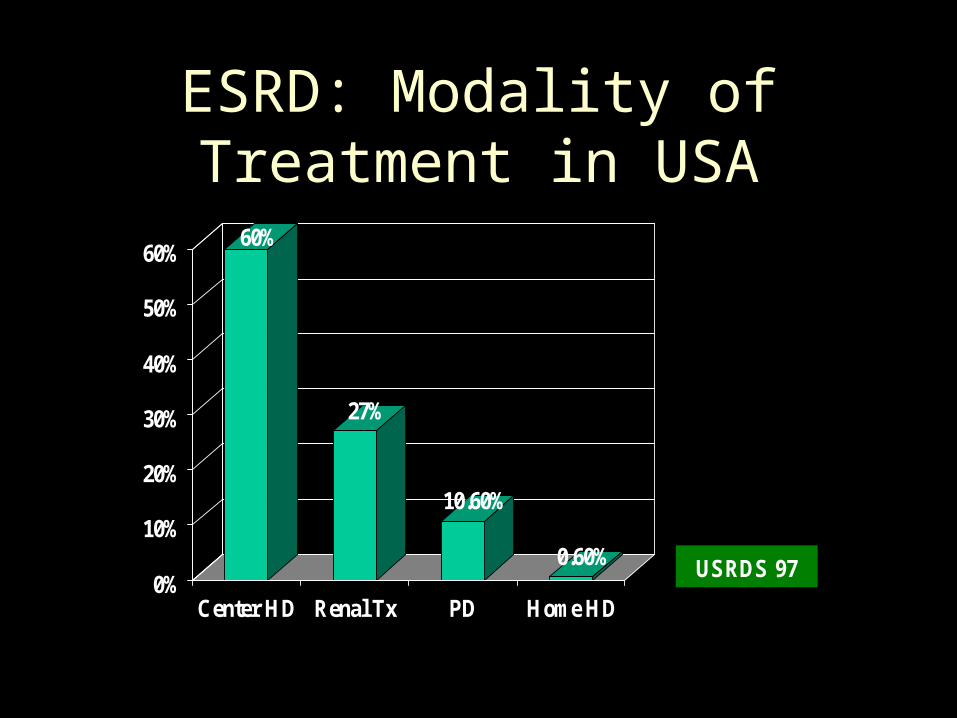
ESRD: Modality of Treatment in USA
60%
27%
10.60%
0.60%0%
10%
20%
30%
40%
50%
60%
Center HD Renal Tx PD Home HD
USRDS 97
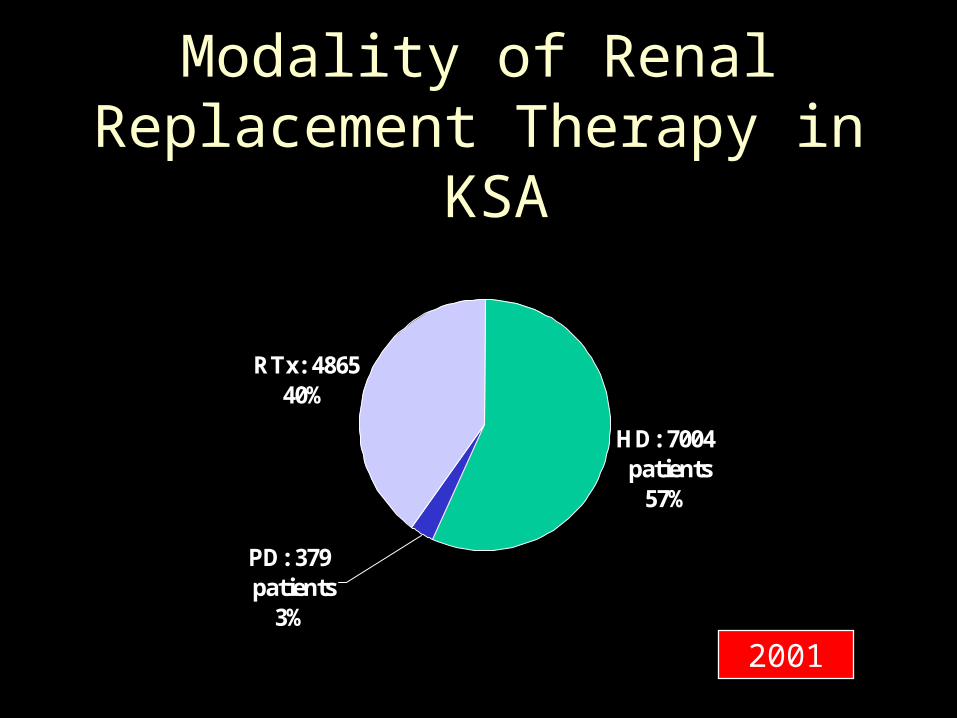
Modality of Renal Replacement Therapy in KSA
HD: 7004 patients
57%
RTx: 486540%
PD: 379 patients
3%
2001

Performed Cadaveric Renal Transplant in KSA
2 0
5974
65
154
83 84
59
89
57
0
20
40
60
80
100
120
140
160
84 86 88 90 92 94 96 98 2000 2001 2002
Kidney Transplantation: Why ?
• Better quality of life – Restoring healthy productive life – May restore sexuality and fertility
• Dialysis-associated morbidity– Access problems and other infections – Bone disease and dialysis-associated
amyloidosis
• Lower mortality

ESRD: Mortality
25 24
7.7
4.2
0
5
10
15
20
25
Dialysis AllESRD
CAD
Deaths/100 Pt. Year
USRDS 97LRD

ESRD: Risk of Death
1
0.32
0.21
00.10.20.30.40.50.60.70.80.9
1
Alldialysis
CAD LRD USRDS 97

Kidney Transplantation: Why?Special Reasons in KSA
• Increasing number of ESRD patients.
• Negative image of dialysis.
• High Incidence and prevalence of HCV infection.
• Poor dialysis therapy “inadequacy”.
• Improper treatment of anaemia and bone disease.

Causes of Morbidity and Mortality
• Hemodialysis– Access problems– Blood Stream Infection– HCV– Bone disease– Dialysis-associated
amyloidosis– Acquired cystic
diseases & RCC– IHD
• Peritoneal Dialysis – CAPD peritonitis
– Loss of Peritoneal membrane
– Hyperglycaemia
– Hyperlipidemia
– Acquired cystic diseases & RCC
– IHD
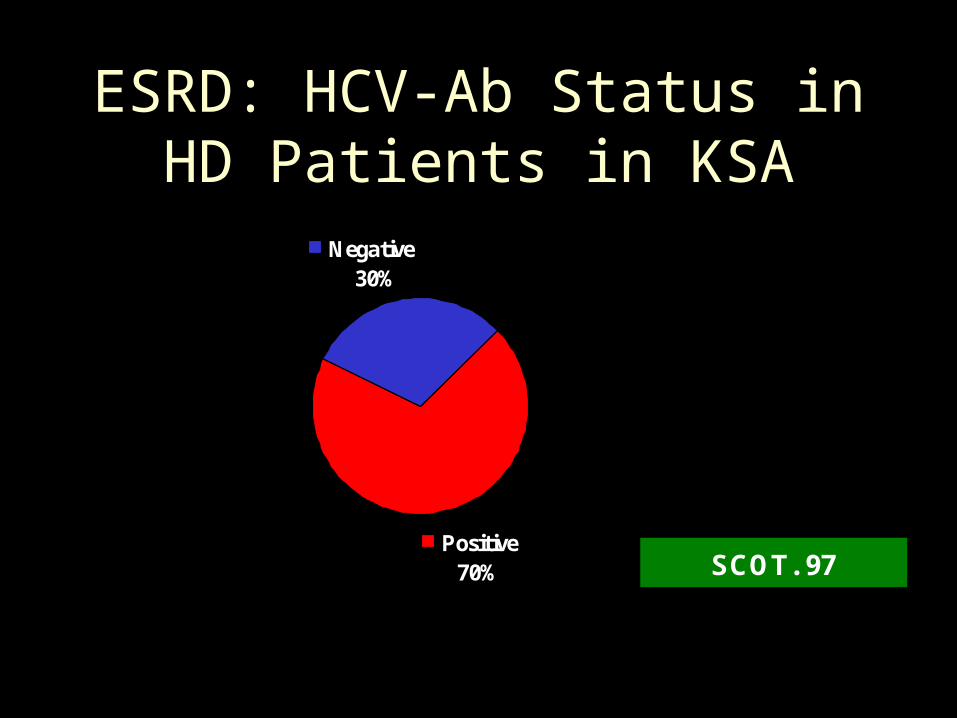
ESRD: HCV-Ab Status in HD Patients in KSA
Positive70%
Negative 30%
SCOT. 97
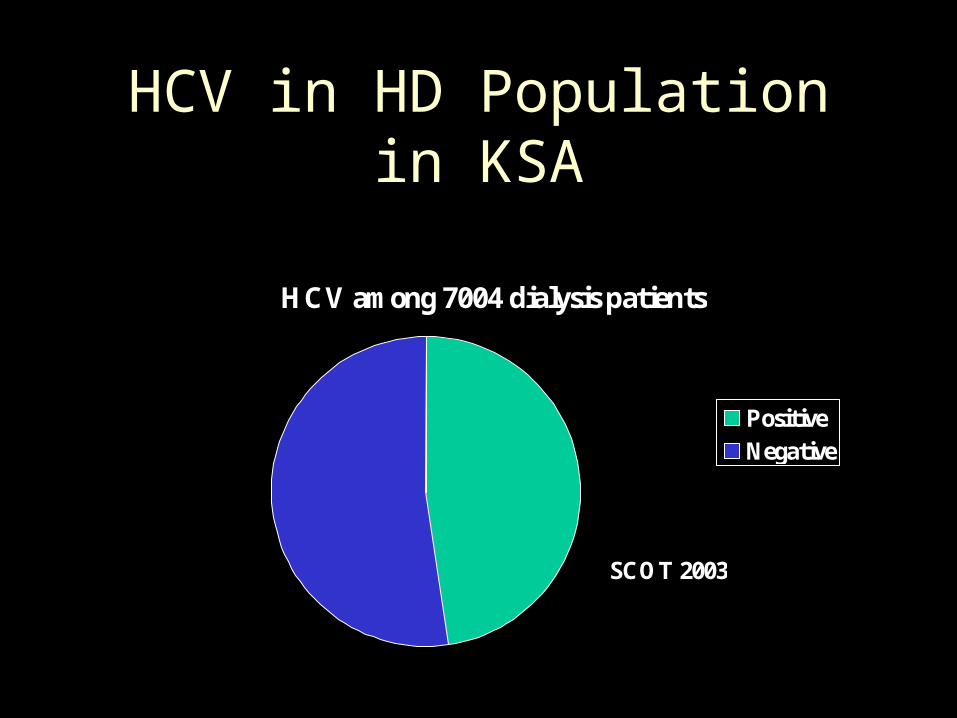
HCV in HD Population in KSA
HCV among 7004 dialysis patients
Positive Negative
SCOT 2003
Kidney Transplantation: Types
• Living-related
• Cadaveric
• Emotionally-related
• Living-non-related

Allograft
• (homograft)– Genetically
disparate individuals of the same species
Hx Background:• In 1933: the 1st Renal allograft by
Voronoy in Ukraine

Transplant Immunology: Components of Immune SystemAntigen presenting cells (APC)
Macrophages & dendritic cells, Langarhan’s cells & vascular cells
T lymphocytesCD4+ (helper T cells)CD8+ (suppressor or Cytotoxic T cells)
B lymphocytes (antibody-forming)
What can happen ?

Ab-dependent cell-mediated
cytotoxicity
Complement-dependent cell-mediated cytotoxicity
IFN-g & TNF-a: up-regulating HLA molecules & co-stim (B7) upon graft & APCs
Graft destruction:
Ag specific & graft-destructive
T-cell
Effector T-cell & NK cell stimulated by granzyme B & perforin
IL-2 & IL-10 plays important role
• In 1954: the 1st long term renal transplant in Boston
HOW ?


Isograft

Then….
• 1958: 1st histocompatibility Ag was described
• 1969: radiation was used

What is this coming drug?

Azathioprine(Imuran)
?
Became available for human use in 1951
Immunosuppressants:Azathioprine
Imidazole analogue Purine antagonist thus inhibiting cellualr
proliferation Poorly selective (suppress all cells
population)Dose 1-2mg/kg/day Allopurinol blocks its catabolism
Fourth Urology Course KAUH, 2004

Immunosuppressants:Azathioprine, Complications
Bone marrow suppression : usually one cell line (especially with allopurinol)
GranulocytopeniaRed cell aplasia Isolated thrombocytopenia
Fourth Urology Course KAUH, 2004
Prednisone
?
Became part of therapy w AZA in 1962
Immunosuppressants:Corticosteroids
Maximal effect on macrophages & lymphocytes Inhibits cytokines gene transcription
Inhibit IL-1, IL-2, IL-6Inhibits INF-gamma & TNFThis will lead to inhibition of T cell proliferation
Used as maintenance therapy (PO) and as a treatment for acute rejection (IV)
Fourth Urology Course KAUH, 2004
• 1962: tissue matching
• 1966: direct cross match
Then ….

Many Ag can serve as histocompatibility Ag:
ABOXenografts
• The strongest of the Tx Ag is the expression of a single chromosomal region called MHC:
– large gene that control traits which influence the entire immune response
– located on chromosome 6
– the gene products of MHC were first investigated on leukocyte & named HLA

• Only on the cells of immune system: mac. dend. B, & activated T• Not as strong
• Can be detected on the cell surface of almost all nucleated cells
• The best trigger of the proliferation of allogenic lymphocytes
On each chromosome 6 there are 6 genetic loci , and on each pair there are 12 loci
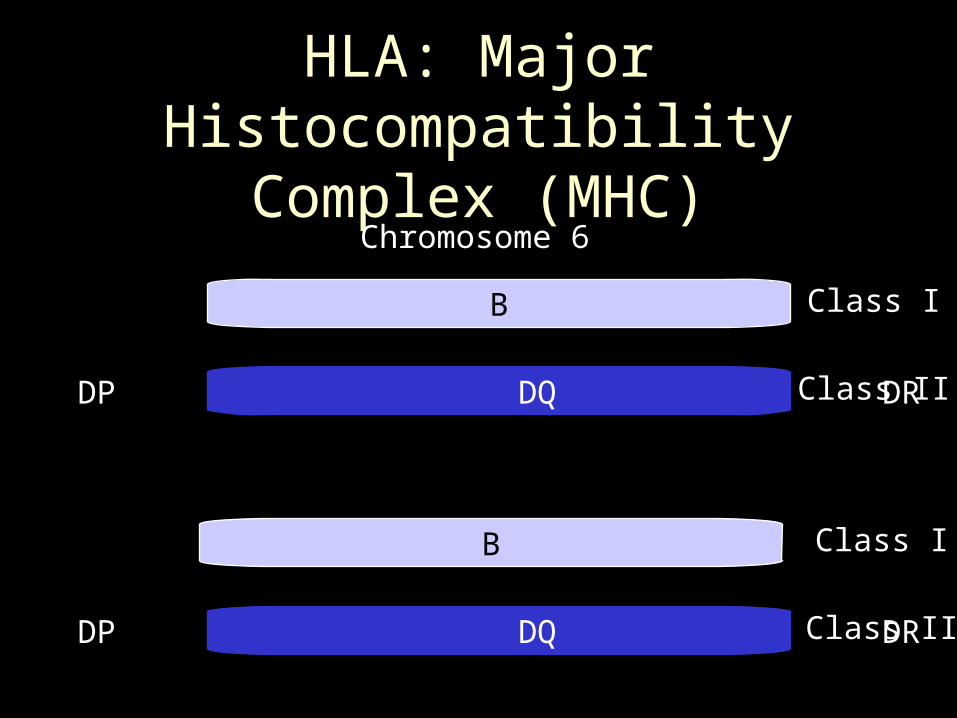
HLA: Major Histocompatibility Complex (MHC)
A B C
DP DQ DR
A B C
DP DQ DR
Class I
Class II
Class I
Class II
Chromosome 6

HLA: Mendelian Transmission
DR01
DP43
DQ7
A03
B14
C28
DR20
DP19
DQ31
A14
B8
C24
DR05
DP12
DQ 03
A18
B53
C11
DR22
DP18
DQ20
A31
B22
C10
A31,B22,C10DR5, DP12,DQ3
A14, B8, C24DR1,DP43,DQ7
A14, B8, C24DR1,DP43,DQ7
A03, B14, C28DR5, DP12, DQ3
A18, B53, C11DR20, DP19, DQ31
Father Mother
1 5432


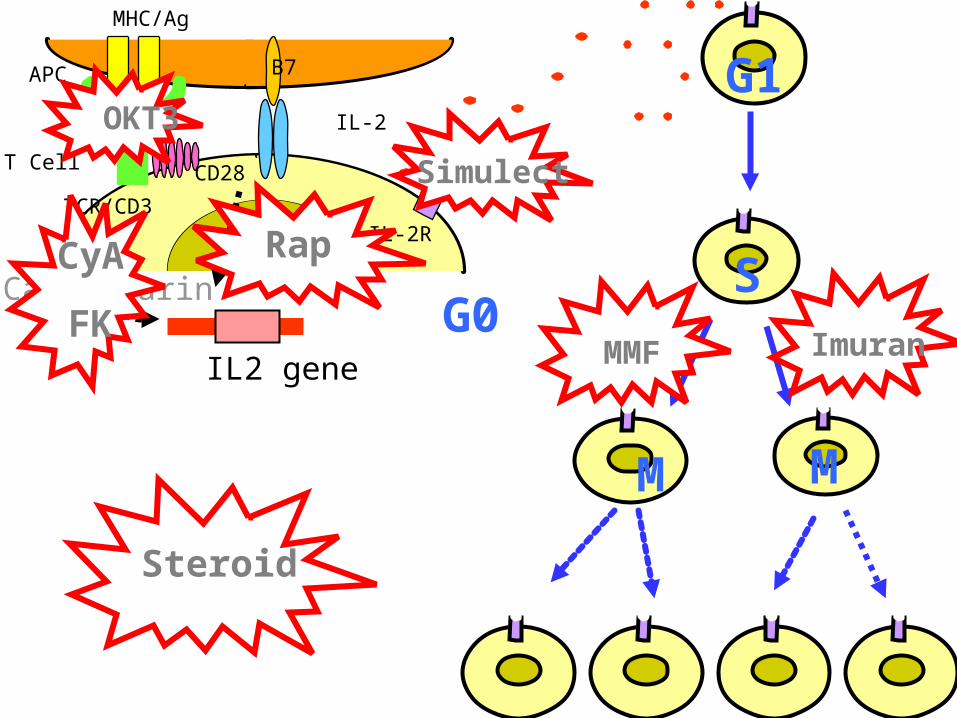
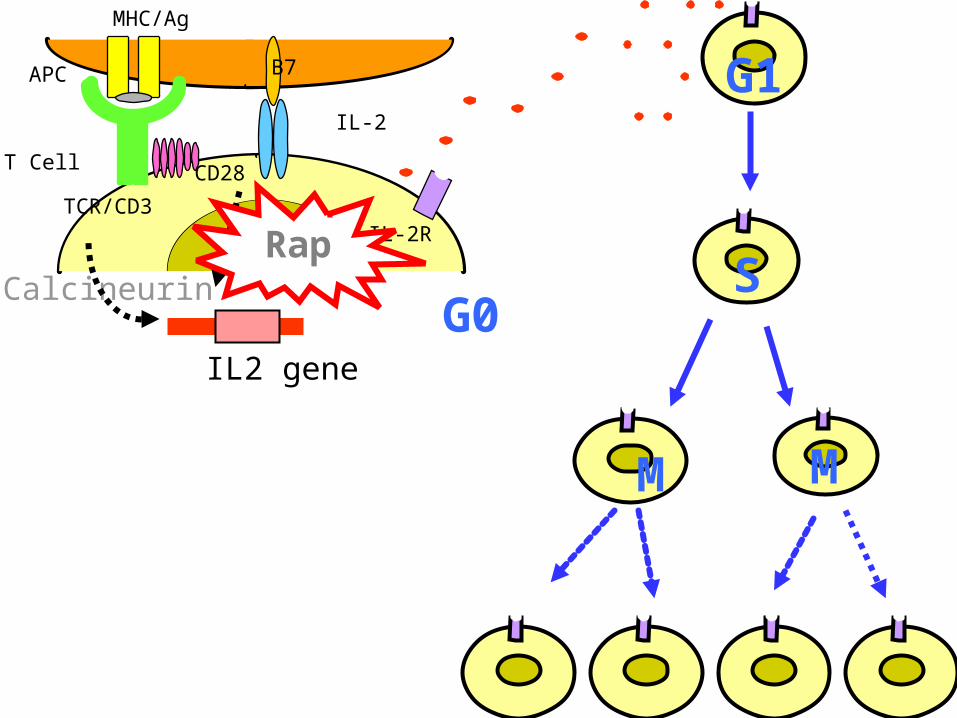
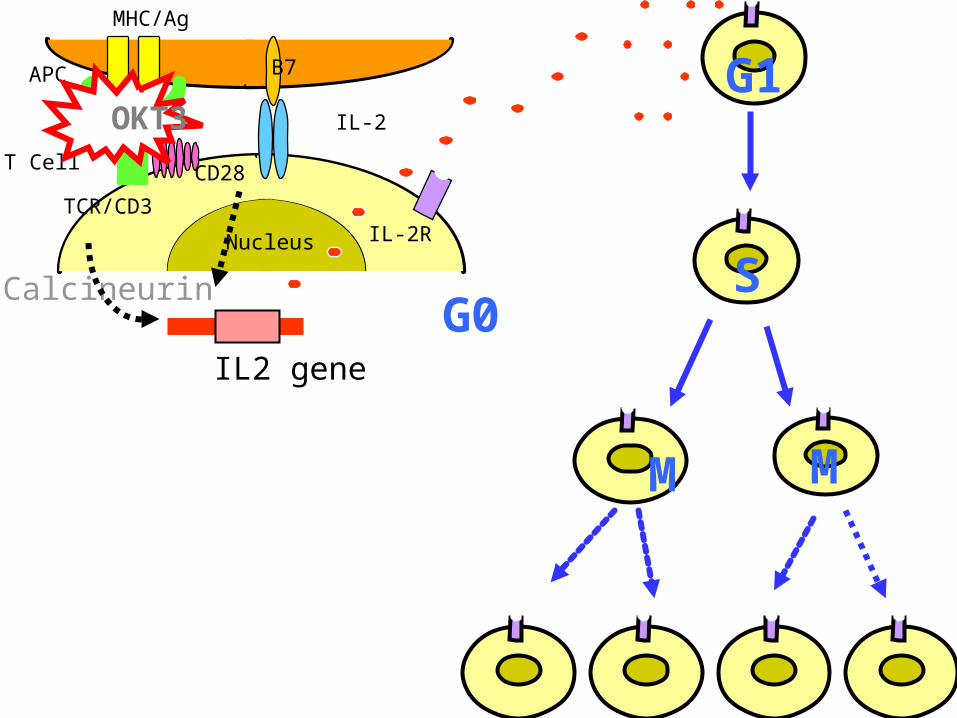
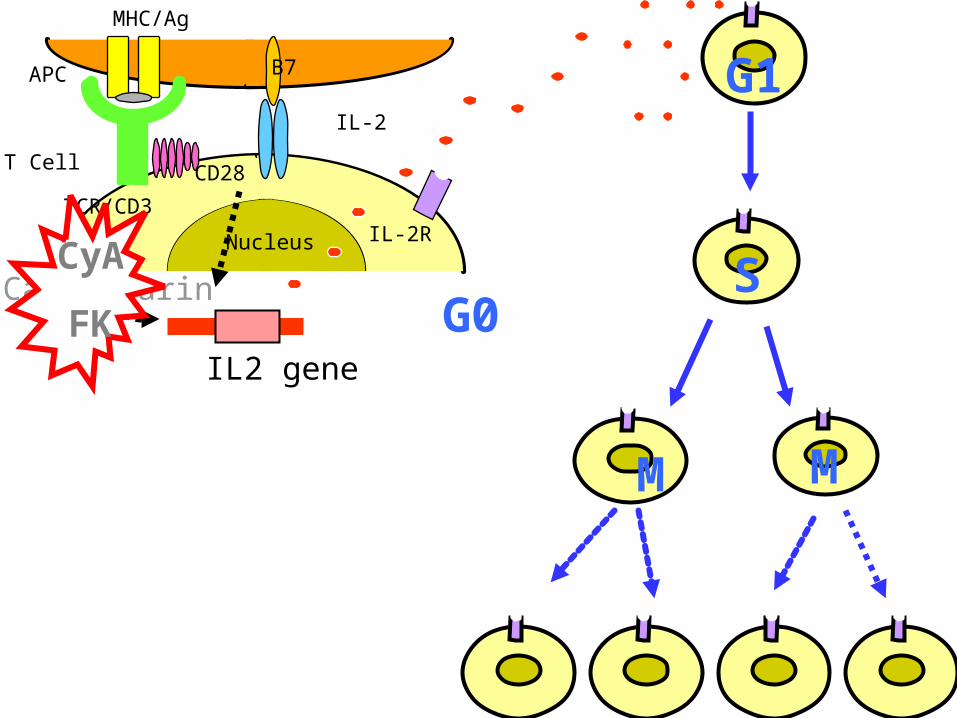
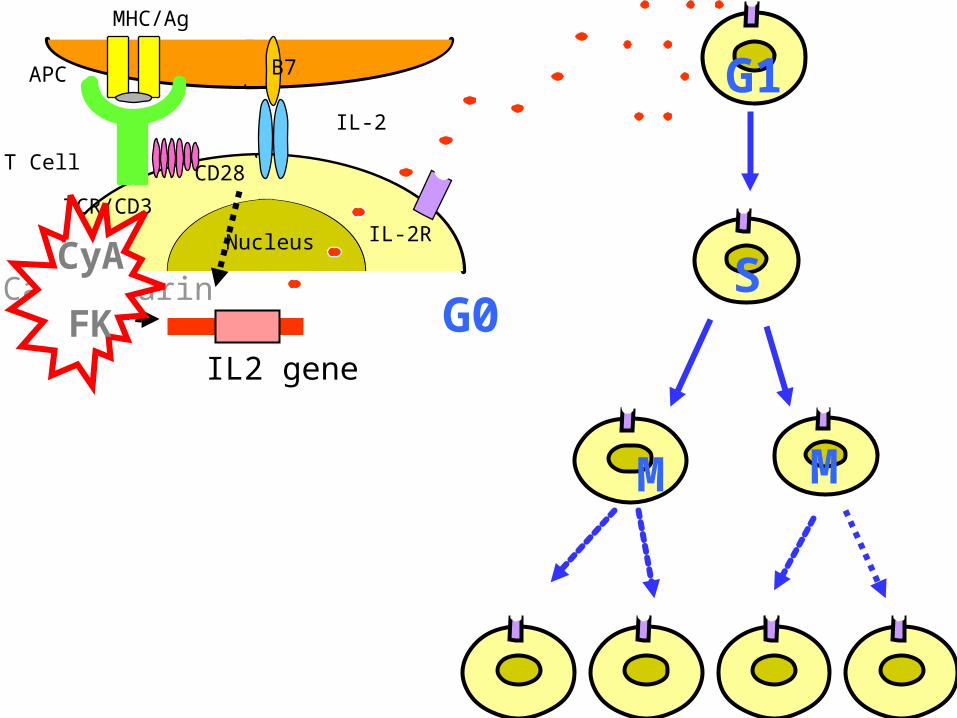
T-cell Activation
APC
T Cell
IL-2R
IL-2
Nucleus
B7MHC/Ag
TCR/CD3
CD28
CD
APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
SImuran
Simulect
MMF
RapCyA
FK
Steroid
M M
OKT3

B-cell stimulation:
• T-cell derived IL-2, IL-4
• Physical contact w T-cell
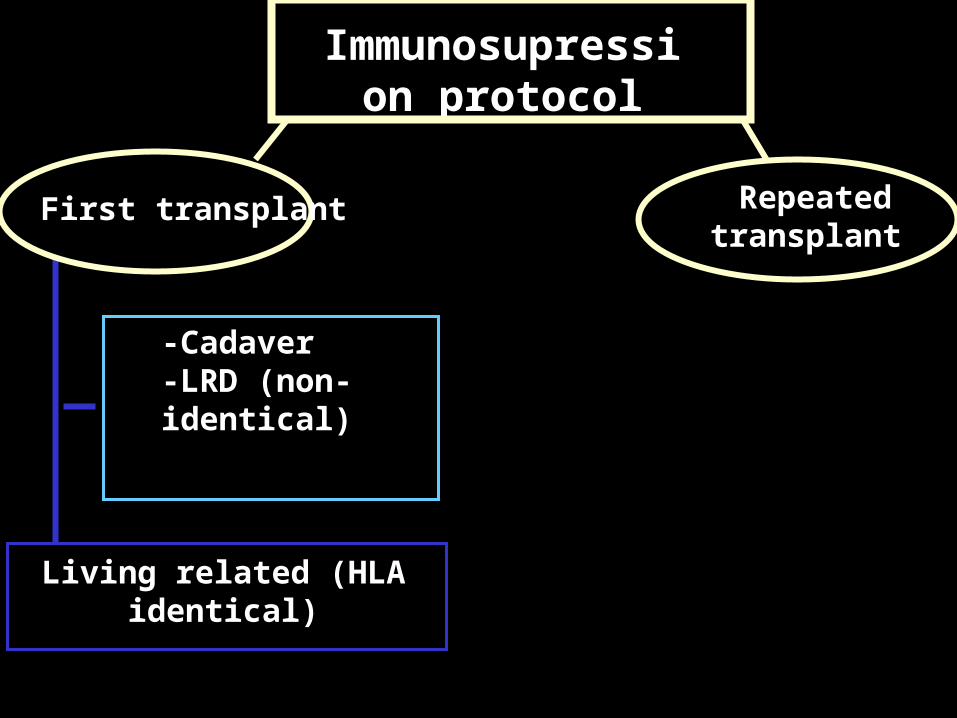
Immunosupression protocol
Repeated transplant
Living related (HLA identical)
-Cadaver-LRD (non-identical)
First transplant
First Cadaveric & LRD (non-identical)• Intra-op
– Methylprednisolone – CyA
• Post-op– CyA--> Neoral– MMF– Prednisone
First Cadaveric & LRD (non-identical)
• Out pt– Neoral– Prednisone
• Taper gradually
– MMF: • Maintain for 1 yr, then D/C
• Switch to Azatioprine if concern about rejection

Repeated Tx
• (Same protocol as 1st Tx) +
• Polyclonal Ab (ALG)– should be started in RR– Few days then start Neoral
• Most pts will remain on CyA, MMF, Pred.
First Living related (HLA identical)
• Same protocol as above w/o MMF (or Azathioprine)

Therapy of rejection
• Prednisone pulse therapy – 500 mg--10 mg / 9 days
• Sever or Steroid resistant– Monoclocal OKT3 for 14 days– Polyclonal ATG, ALG

There are 4 key needs which, if not met, could marginalize Tx as a form of therapy:
• 1-Achieving optimal immunosuppression
• 2-Overcoming chronic rejection
• 3-New therapeutic targets
• 4-Increasing the # of organ donation

• Immune factors
• Non-immune factors
2-Overcoming chronic rejection

Immune factors
• Multifactorial
• Needs more Ix of:– endothelial cell activation– expression of adhesion molecules – cytokines – chemokinse

Rapa
?
Sirolimus (Rapamycin): Side Effects
•Hyperlipidemia •Impair wound healing •More potent Immunosuppression when combined
with CNI•Pneumonitis •Thrombocytopenia •Hypokalemic•Early vascular thrombosis
Fourth Urology Course KAUH, 2004

Rapamycin
• It is a macrocylic ABx produced by Streptomyces hygroscopicus
• binds to– FKBP– TOR1 & TOR2
APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
SRap
M M

FKBP
P70 S6 pr kinase
RAPA
Immunosuppressants:rapamycin (Sirolimus)
Macrolide analogue It binds to FKBP (TOR) but does not inhibit
calcineurin It has different mechanism of action than
CSA and tacrolimus It inhibits growth factor cell transduction No nephrotoxicity
Non-immune factors
• It’s implication concerns clinical groups across the world
• Only 25-30% of R.Tx are normotensive
• Causes are multifactorial– angiotensin system– can be worse w hyperlipidemia

3-New Therapeutic Targets
• Tolerance
• Gene therapy
• Complement inhibition
Tolerance
• “specific absence of an immune response to an Ag.”
but may also involve active immune response !
– 1-clonal deletion– 2-clonal ignorance– 3-active suppression

Donor B.M. infusion in renal Tx
4-Increasing # Of Organ Donors• Live donation
– education• 3yrs f/u of 134 pt revealed:
• 1.3% morbidity
• No mortality
• Better results in term of graft survival
– non-heart beating
• Xenotransplantation
Melchor, 1998

Xenograft• (hetrograft)
Between different species (animal to human)

Ethical issues
• Potential recipient
• Psychological stress
• Risk of xenozoonoses

1-Achieving optimal immunosuppression:
?

AntilymphocyteALG
ATGAM
Thymoglobulin
?

OKT3
?
Antibody Therapy:
• Types:– Monoclonal : e.g. OKT3– Polyclonal: e.g. ATG
• M/A• Indications
– Induction– Steroid-resistant rejection
• Side effects
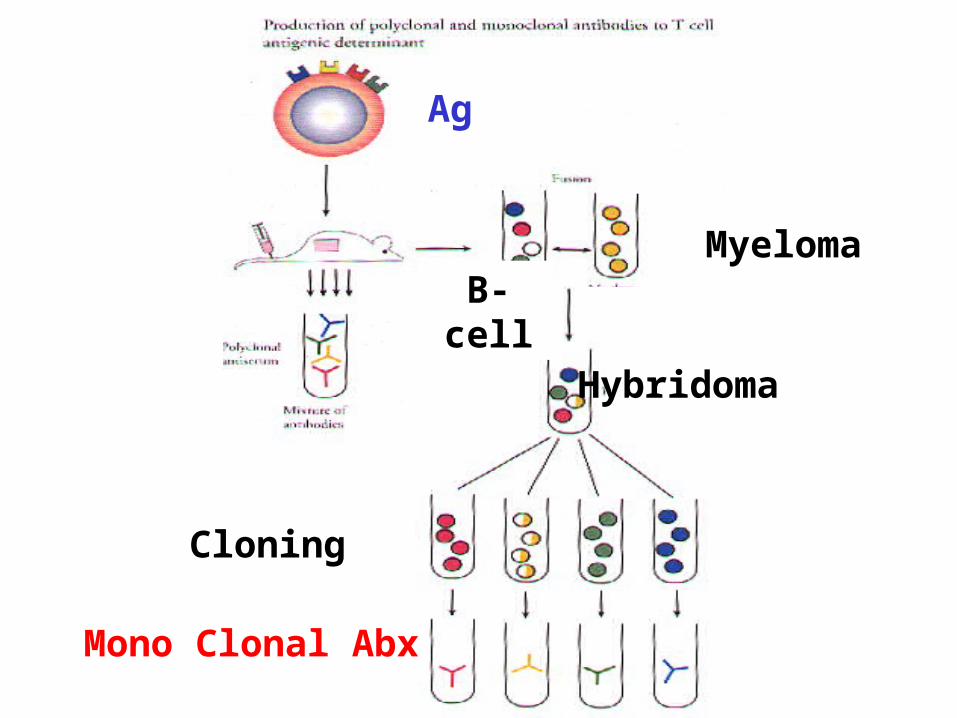
Hybridoma
Myeloma
B-cell
Cloning
Mono Clonal Abx
Ag
APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
S
M M
OKT3

e CD3
a B TCR
TCR/CD3

CyA KK
?
Immunosuppressants:Cyclosporine A
Inhibit cell growth by inhibiting of gene transcription of IL-2
It binds with cytoplasmic receptor protein (cyclophillin)
CSA-cyclophillin complex binds with Calcineurins and inhibits its phosphatase
activityThis will lead to inhibition of IL-2 gene
transcription & subsequently IL-2 production
Fourth Urology Course KAUH, 2004
Cyclosporine
• The introduction of CyA in 1980s established Tx as a routine procedure.
• Fungal peptide
• M/A
• Effect: reversible & specific for T-lymphocyte
• Side effects:
Achieving optimal immunosuppression
APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
SCyA
FK
M M
FK 506(Tacrolimus)
KK
MMF
?
Immunosuppressants:FK506 (Tacrolimus)
Inhibit cell growth by inhibiting of gene transcription of IL-2
It binds with cytoplasmic receptor protein (FKBP)
FK506-FKBP complex binds with calcineurin and inhibits its phosphatase activity
This will lead to inhibition of IL-2 gene transcription & subsequently IL-2 production
Fourth Urology Course KAUH, 2004

Immunosuppressants:Cyclosporine A & FK506 Use
CSA :Maintenance Immunosuppressants for all organ
transplant Dose 4-8mg/kg/day in divided doses
Tacrolimus (FK506): 0.15-.3mg/kgFor female patients Rescue therapy for renal transplant High immunogenicity
Fourth Urology Course KAUH, 2004
Immunosuppressants:differences Between Cyclosporine A & Tacrolimus
Cyclosporine More gingival
hyper-plasiaMore hirsuitismMore Hepato-toxic
TacrolimusMore potent than CSA More neurotoxicityAllopecia Hyperglycaemia (25%
Vs 4% for CSA)
Fourth Urology Course KAUH, 2004
APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
SCyA
FK
M M
MMF(Cellcept)
?

APC
T Cell
IL-2R
IL-2
Nucleus
B7
MHC/Ag
TCR/CD3
CD28
Calcineurin
IL2 gene
G0
G1
S
MMF
M M
Immunosuppressants
Site of action Classifications Immunosuppressants and their
side effects Adjuvant therapy
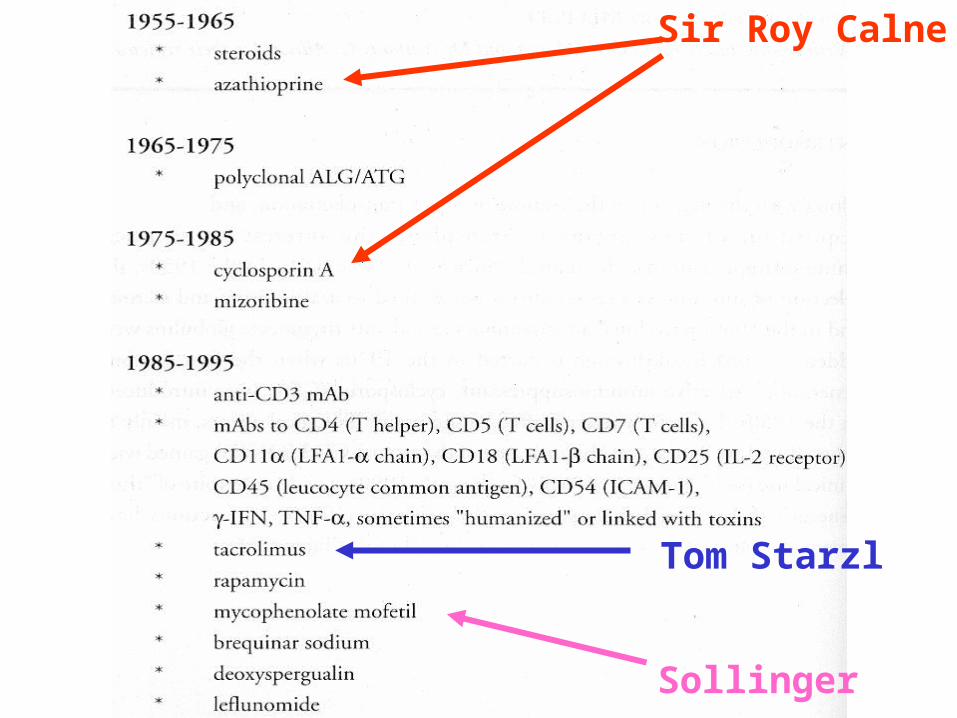
Sir Roy Calne
Tom Starzl
Sollinger

Immunosuppressants: Classification
Inhibitors of transcription Corticosteroids (IL-1, IL-2, IL-3, IL-6, TNF-
alpha, gamma-interferon)CSA: IL-2FK506 (tacrolimus): IL-2
Inhibitors of growth factors signal TransductionRapamycin (sirolimus): IL-2

Inhibition of Gene Transcription
• Azathioprine• Broad myelocytic suppressant (poorly selective)
– Inhibit T-cell proliferation
Inhibition of Gene Transcription
– Mycophenolate mofetil (MMF): Cellcept • Selective lymphocyte suppressant
• Down-regulate the expression of adhesion molecules
– Mycophenolate salt (MPS): Myofortic • Selective lymphocyte suppressant
• Less GI symptoms ?
• More potent ?

Kidney Transplantation: Workup of Recipient
• Comprehensive history and physical• Biochemistry tests• CBC• HBsAg, HCV-Ab, HIV, CMV, EBV• PPD• EKG, Echo, stress test, coronary catheterisation • CXR, US abdomen and pelvis , Mammogram, MRI
and VCUG • Dental, cardiology, urology, GI and ID consultations
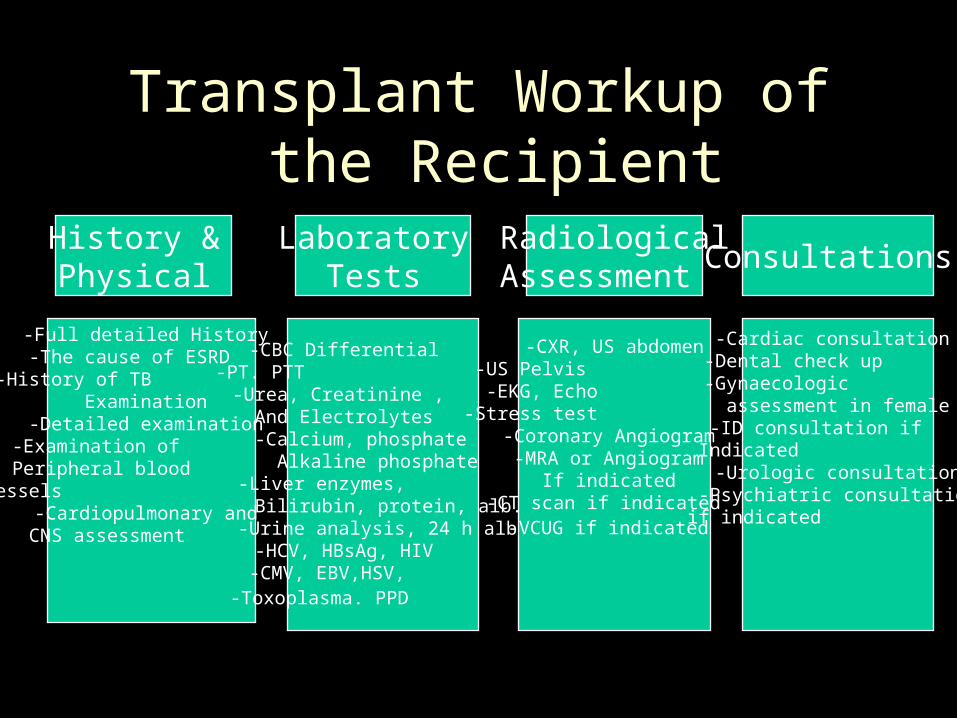
Transplant Workup of the Recipient
-Full detailed History -The cause of ESRD -History of TB
Examination -Detailed examination -Examination of Peripheral blood Vessels
-Cardiopulmonary and CNS assessment
-CBC Differential -PT. PTT -Urea, Creatinine , And Electrolytes
-Calcium, phosphate Alkaline phosphate
-Liver enzymes, Bilirubin, protein, alb.
-Urine analysis, 24 h alb.-HCV, HBsAg, HIV -CMV, EBV,HSV, -Toxoplasma. PPD
-CXR, US abdomen-US Pelvis -EKG, Echo -Stress test
-Coronary Angiogram -MRA or Angiogram
If indicated -CT scan if indicated -VCUG if indicated
-Cardiac consultation -Dental check up -Gynaecologic assessment in female-ID consultation if Indicated
-Urologic consultation-Psychiatric consultation
if indicated
History & Physical
RadiologicalAssessment
Laboratory Tests
Consultations

Kidney Transplantation: Contraindication to Tx .
• Active infection: Bacterial, TB, HCV, CMV
• Malignancies
• Active auto-immune disease
• High cardiac risk
• High operative risk
• Pregnancy
Kidney Transplantation: Workup of the Donor
• Same as recipient plus – Three 24 hour urine collections for protein and
Creatinine clearance – Three urine sediment exam – Renal Angiogram or MRA– Psychiatric consultation
Transplantation: Pre-Tx. Match
ABO match:As preformed natural anti-a, or anti-b abs will
cause accelerated rejection
HLA match:Lymphocyte match:
Circulating preformed Abs against major HLA (donor’s class-i HLA) cause hyperacute rejection

Kidney Transplant: Complications
• Hypertension• Metabolic abnormalities
– DM and hyperglycemias
– Hyperlipidemia
– Hyper & hypokalemia, hypomagnesaemia
– RTA
– Hyperuricemia
– Hypophosphatemia
– Osteoporosis

Transplant Complications:
• Gastro-intestinal tract• Peptic ulcer disease • Pseudo-membranous colitis • CMV colitis • Pancreatitis
• Polycythemia

Transplant Complications:(Continued)
Long and short term complications
• Malignancies
• Cardiovascular: CAD• HTN , DM & Immunosuppressants
• Renal artery Stenosis
• Obesity


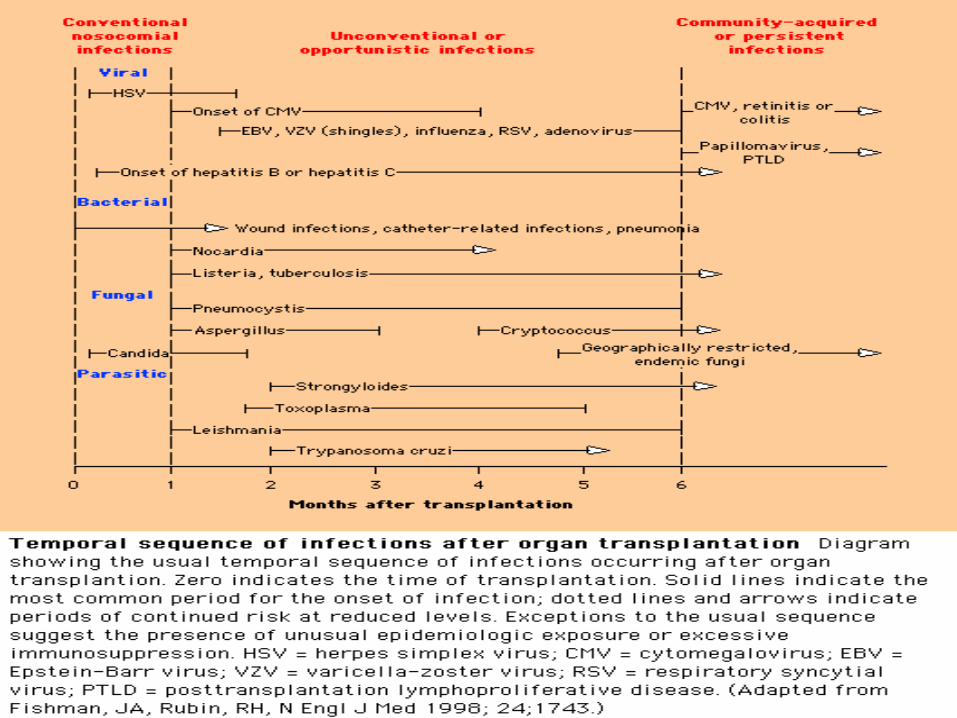
Infectious Complications of Transplantation
-Wound infections
-UTI
-Line-related infections
-HSV
- Oral candida
-CMV
-VZV
-EBV
-PCP
-Hepatitis
-Nocardia
-Listeria
-TB
- CMV
-TB
-Papilloma virus
-Other community-acquired infections
0-3 weeks Usual infections
1-6 months Opportunistic
6 monthsCommunity-acquired

Transplant Complications: Malignancies
• Cancer: (1.6%).• Skin cancer (squamous cell ca, basal cell ca &
melanoma).• PTLD.
• NHL.• EBV-related lympho proliferative syndrome.• Reticulum cell sarcoma.
• Caposi’s sarcoma.• Others: kidney, GU etc...

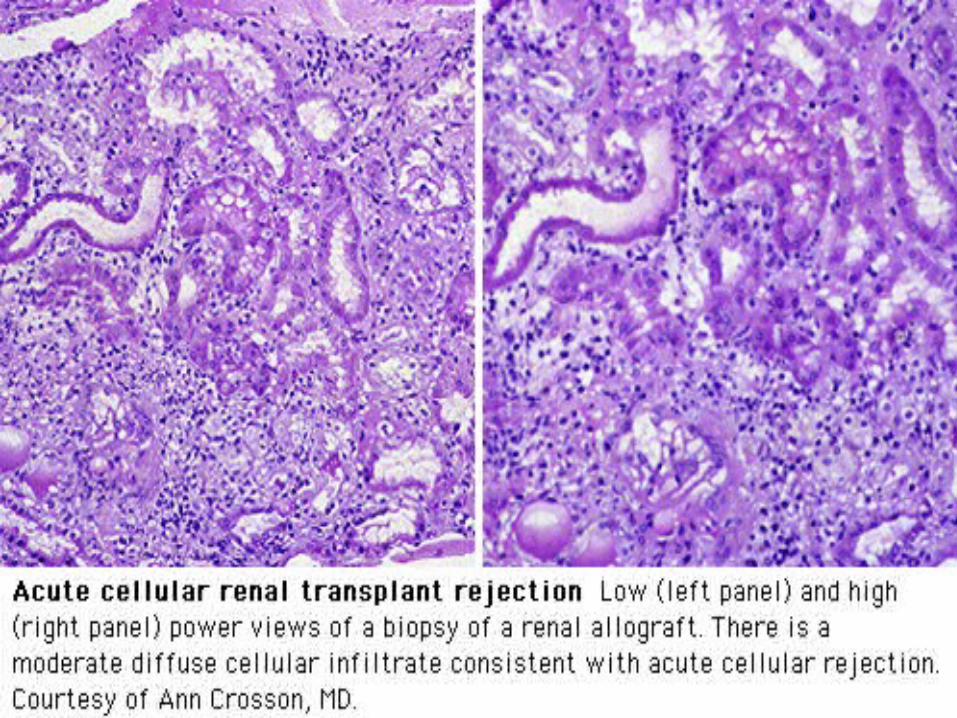
Renal Transplant Rejection
• Hyperacute rejection
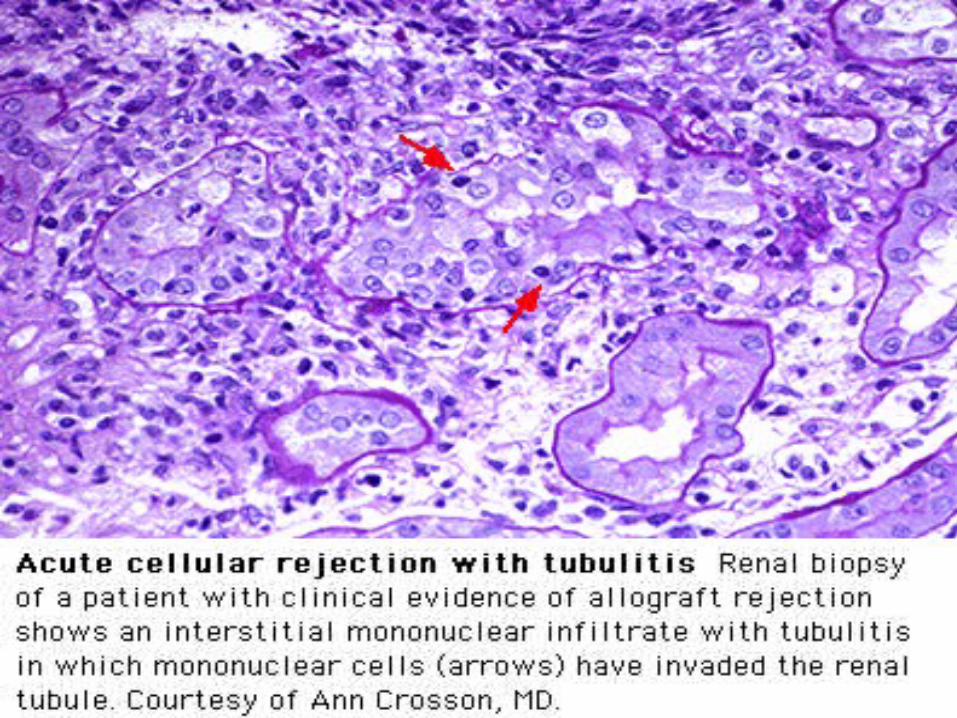
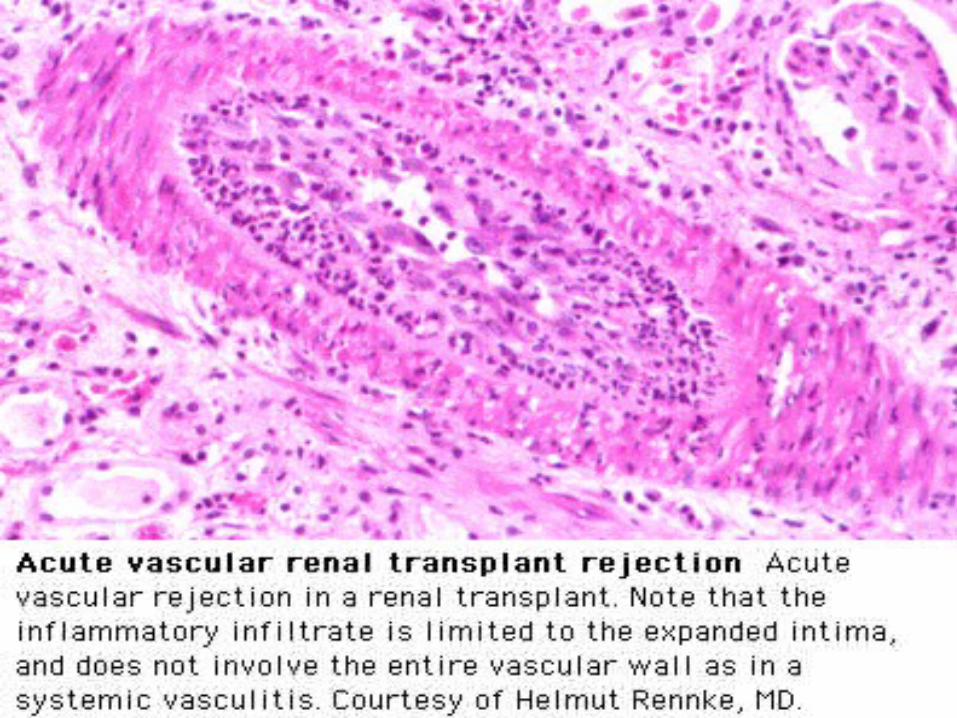
• Acute Rejection• Cellular • Vascular
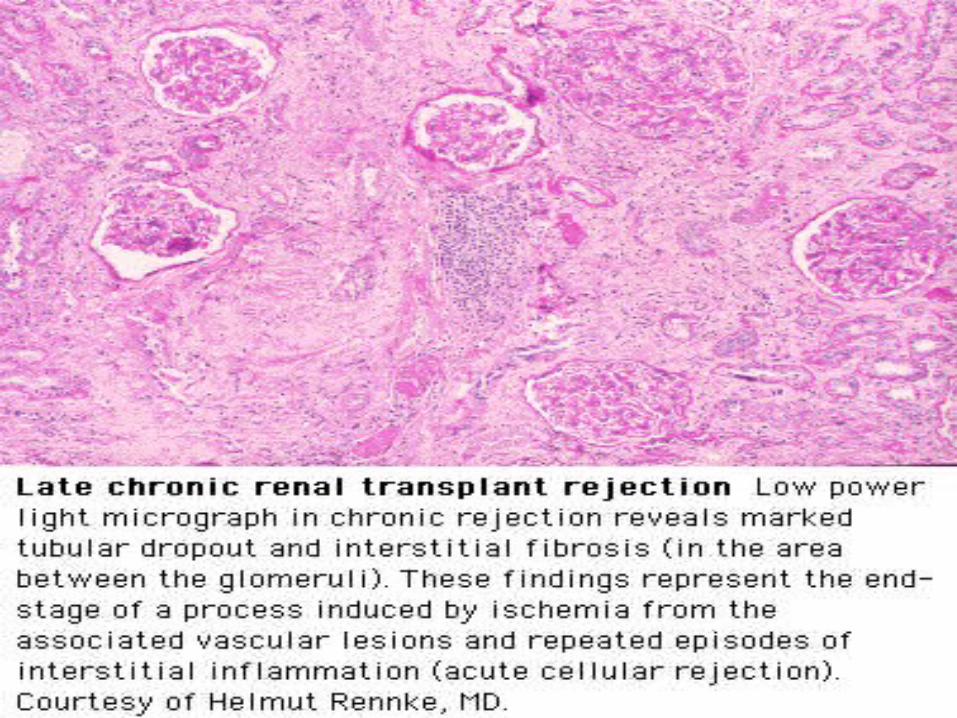
• Chronic rejection

Causes of Morbidity and Mortality
• Dialysis – Access problems
– Line-related sepsis
– HCV
– Anaemia
– Bone disease
– Dialysis-associated amyloidosis
– IHD
• Transplantation – IHD
– DM and hyperlipidemia
– Osteoporosis
– Opportunistic infections
– Malignancies
• PTLD
• Skin cancer
– Osteoporosis

Kidney Transplantation: Challenges
• Over or under-immune suppression – “Individualization and minimization”
• Chronic Rejection and Tx Glomerulopathy– CNI avoidance
– New agents
– Immune tolerance
• IHD – More aggressive approach to co-morbid conditions
• Hyperlipidemia and DM
Future of Transplantation
• “Individualization and Minimization”
• Immune tolerance – New agents– Gene therapy
• Xeno-transplantation