Exemplary Care Cutting-edge Research World-class Education Raghavan Murugan MD, MS, FRCP...
26
Exemplary Care Cutting-edge Research World-class Education Raghavan Murugan MD, MS, FRCP Associate Professor Dept. of Critical Care Medicine Clinical and Translational Science Core Faculty, Center for Critical Care Nephrology, CRISMA University of Pittsburgh School of Medicine Intensivist, Abdominal Organ Transplant ICU University of Pittsburgh Medical Center Understanding Mechanisms in Acute Kidney Injury
-
Upload
alaina-floyd -
Category
Documents
-
view
215 -
download
1
Transcript of Exemplary Care Cutting-edge Research World-class Education Raghavan Murugan MD, MS, FRCP...

Exemplary Care Cutting-edge Research World-class Education
Raghavan Murugan MD, MS, FRCPAssociate Professor Dept. of Critical Care Medicine Clinical and Translational ScienceCore Faculty, Center for Critical Care Nephrology, CRISMAUniversity of Pittsburgh School of Medicine
Intensivist, Abdominal Organ Transplant ICUUniversity of Pittsburgh Medical Center
Understanding Mechanisms in Acute Kidney Injury

Exemplary Care Cutting-edge Research World-class Education
AcknowledgementsJohn Kellum, MD, MCCM
Derek Angus, MD, MPH
Paul Palevsky, MD
Lisa Weissfeld, PhD
Michele Elder, RN, MSN
Melinda Carter, BS
Xiaoyan Wen, PhD
Francis Pike, PhD
Lan Kong, PhD,
Minjae Lee, PhD
CRISMA and CCN Staff
NIH KL2 (CTSI)

Exemplary Care Cutting-edge Research World-class Education
ObjectivesMechanisms related to AKI susceptibility
Mechanisms related to AKI outcomesRenal RecoveryMortality
CohortSepsis-induced AKI – community-acquired pneumonia
Genetic and Inflammatory Markers of Sepsis (GenIMS)Critically ill patients receiving renal replacement therapy (RRT)
Acute Renal Failure Trial Network (ATN) and the Biological Markers of Recovery for Kidney (BioMaRK)
Exemplary Care Cutting-edge Research World-class Education
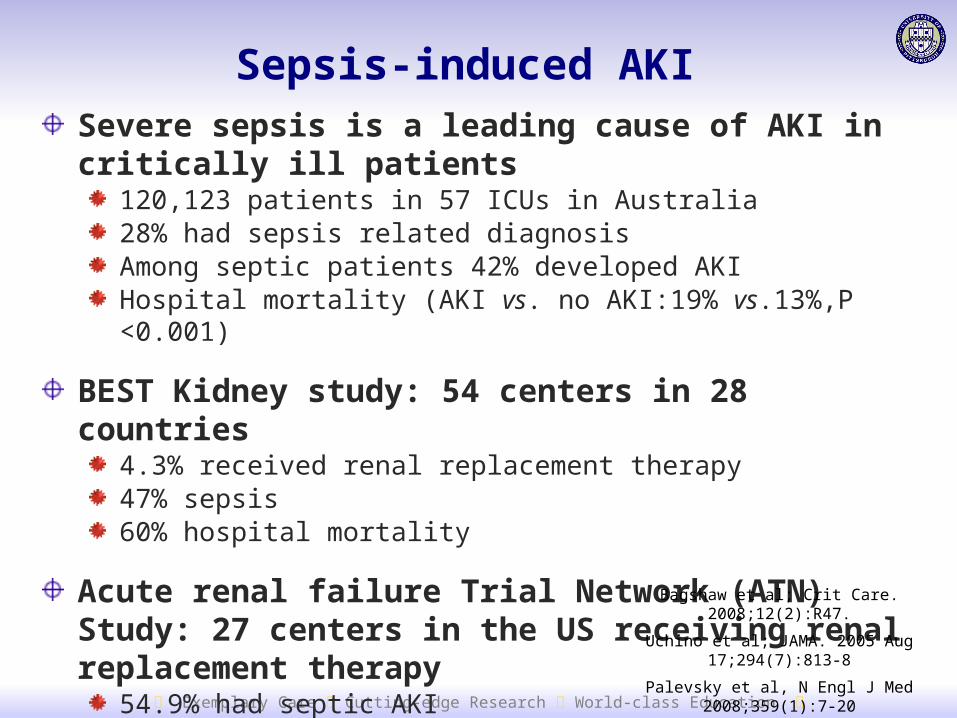
Severe sepsis is a leading cause of AKI in critically ill patients
120,123 patients in 57 ICUs in Australia 28% had sepsis related diagnosisAmong septic patients 42% developed AKIHospital mortality (AKI vs. no AKI:19% vs.13%,P <0.001)
BEST Kidney study: 54 centers in 28 countries4.3% received renal replacement therapy47% sepsis60% hospital mortality
Acute renal failure Trial Network (ATN) Study: 27 centers in the US receiving renal replacement therapy
54.9% had septic AKI60 day mortality: 54% for septic AKI Bagshaw et al; Crit Care. 2008;12(2):R47.
Uchino et al; JAMA. 2005 Aug 17;294(7):813-8
Palevsky et al, N Engl J Med 2008;359(1):7-20
Sepsis-induced AKI

Exemplary Care Cutting-edge Research World-class Education
Risk and outcome of AKI in community-acquired pneumonia (CAP)
Murugan, R, et al; Kidney International; 2010;77:527–535
1,836 patients with CAP
Risk of AKI = 34%
1 year mortality for AKI: adjusted HR range = 1.10-2.10, P <0.001

Exemplary Care Cutting-edge Research World-class Education
Risk of death following AKI in pneumonia
Days after pneumonia hospitalization
0
0.5
1.0
1.5
2.0
2.5
3.0
0 50 100 150 200 250 300 350 400
Haz
ard
rat
ios
wit
h 9
5% C
I
0
0.5
1.0
1.5
2.0
2.5
3.0
0
0.5
1.0
1.5
2.0
2.5
3.0
0 50 100 150 200 250 300 350 400
adjusted hazard ratio range = 1.10-2.10, P <0.001
Murugan, R, et al; Kidney International; 2010;77:527–535
Exemplary Care Cutting-edge Research World-class Education
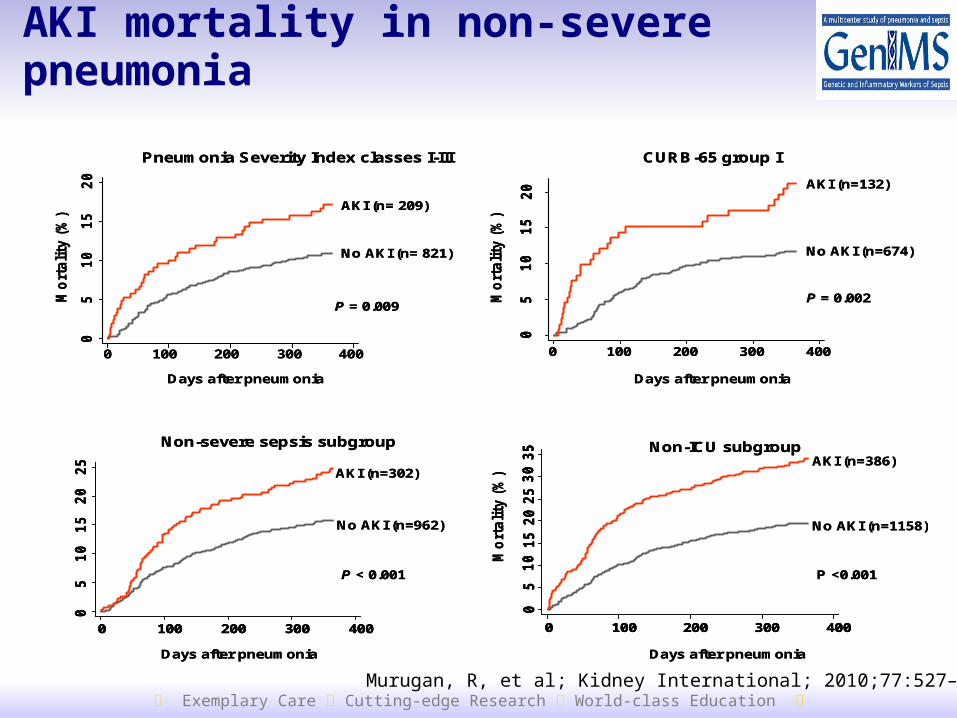
AKI mortality in non-severe pneumonia0
51
01
52
0
0 100 200 300 400
Days after pneumonia
Mo
rtali
ty (
%)
AKI (n= 209)
No AKI (n= 821)
Pneumonia Severity Index classes I-III
P = 0.009
Mo
rtali
ty (
%)
05
10
15
20
0 100 200 300 400
Days after pneumonia
CURB-65 group I
AKI (n=132)
No AKI (n=674)
P = 0.002
05
10
15
20
25
0 100 200 300 400
Days after pneumonia
Non-severe sepsis subgroup
AKI (n=302)
No AKI (n=962)
P < 0.001
05
10
15
20
25
30
35
0 100 200 300 400
Days after pneumonia
Non-ICU subgroup
P <0.001
No AKI (n=1158)
AKI (n=386)
Mo
rtali
ty (
%)
05
10
15
20
0 100 200 300 400
Days after pneumonia
Mo
rtali
ty (
%)
AKI (n= 209)
No AKI (n= 821)
Pneumonia Severity Index classes I-III
P = 0.009
Mo
rtali
ty (
%)
05
10
15
20
05
10
15
20
0 100 200 300 400
Days after pneumonia
CURB-65 group I
AKI (n=132)
No AKI (n=674)
P = 0.002
05
10
15
20
25
05
10
15
20
25
0 100 200 300 4000 100 200 300 400
Days after pneumonia
Non-severe sepsis subgroup
AKI (n=302)
No AKI (n=962)
P < 0.001
05
10
15
20
25
30
35
05
10
15
20
25
30
35
0 100 200 300 4000 100 200 300 400
Days after pneumonia
Non-ICU subgroup
P <0.001
No AKI (n=1158)
AKI (n=386)
Mo
rtali
ty (
%)
Murugan, R, et al; Kidney International; 2010;77:527–535

Exemplary Care Cutting-edge Research World-class Education
0
1
2
3
4
5
6
1 2 3 4 5 6 7
Hospital day
Lo
g m
ean
s CAP, severe sepsis, died
CAP, severe sepsis, alive
CAP, no organ failure
Kellum JA et al. Arch Intern Med 2007; 167(15):1655-63
IL-6 and severe sepsis

Exemplary Care Cutting-edge Research World-class Education
Inflammatory and Coagulation Markers in AKI and CAP
Day 1 BiomarkerConcentration in
CAP *AKI No AKI P Value
Interleukin-6 73.97 36 0.001
Tumor necrosis factor 7.46 4.82 0.001
Interleukin-10 7.03 5.14 0.002
Factor IX 122 121.5 NS
Anti-thrombin 85 89 NS
Thrombin-antithrombin 4.4 3.4 < 0.001Plasminogen activator inhibitor-1 6.71 4.95 < 0.001
D-Dimer 787.76 525 < 0.001
* Median values in pg/ml

Exemplary Care Cutting-edge Research World-class Education
Interleukin-6 and AKIIn
terl
euki
n-6
, p
g/m
l
0
20
40
60
80
100
120
1 2 3 4 5 6 7Days after pneumonia
AKI, Severe sepsis
AKI, No severe sepsis
No AKI, Severe sepsis
No AKI, No severe sepsis
Murugan, R, et al; Kidney International; 2010;77:527–535

Exemplary Care Cutting-edge Research World-class Education
Variable Odds Ratio 95% CI P-value
age 1.0461 1.0384 to 1.0538 < 0.001
IL-6 1.1283 1.0522 to 1.2098 < 0.001
TNF 1.5776 1.3258 to 1.8773 < 0.001
Baseline Cr 6.1672 2.7679 to 13.7416 < 0.001
Female 0.7007 0.5304 to 0.9256 0.012
AKI in Pneumonia Patients
16% 7% 10%67%
Risk of AKI
P < 0.001
0
20
40
60
80
100
120
No AKI Risk Injury Failure
Day
1 I
L-6
(p
g/m
l)

Exemplary Care Cutting-edge Research World-class Education
Risk of renal replacement therapy during CAP hospitalization
2.6% in patients with AKI9% in patients with severe AKI (RIFLE-F)
Renal recovery by hospital dischargeComplete: 46.2%Partial: 11.4%Non-recovery: 42.3%
Risk of end-stage renal disease by 3 months in survivors of AKI
1.8% in all patients with AKI5.6% in patients with severe AKI (RIFLE-F)37.5% in patients who receive inpatient RRT
Renal Recovery after AKI in CAP

Exemplary Care Cutting-edge Research World-class Education
1-year mortality by renal recovery
50
263 167 151 141Non-recovery71 55 48 46Partial
287 245 239 224Complete1205 1078 1014 977No AKI
Number at risk
025
0 100 200 300 400
Days after pneumonia hospitalization
Mo
rtal
ity
(%)
No AKIComplete
Partial
Non-recovery
P = <0.001

Exemplary Care Cutting-edge Research World-class Education
Cause of death after AKI
Cardiovascular Infection Malignancy Respiratory Renal/metabolic
Others0
5
10
15
20
25
30
35
40
No AKI
AKI
Cau
se-s
pec
ific
mo
rtal
ity
(%)
Murugan, R et. al.; Clin J Am Soc Nep 2012

Exemplary Care Cutting-edge Research World-class Education
Cardiovascular deaths by renal recovery
No AKI Complete Partial Nonrecovery0
5
10
15
20
25
30
No pre-existing CVD
Pre-existing CVD
Car
dio
vasc
ula
r d
eath
s (%
)

Exemplary Care Cutting-edge Research World-class Education
Statins and 1-yr Mortality in Patients with CAP-induced AKI
Murugan, R et. al.; Clin J Am Soc Nep 2012

Exemplary Care Cutting-edge Research World-class Education
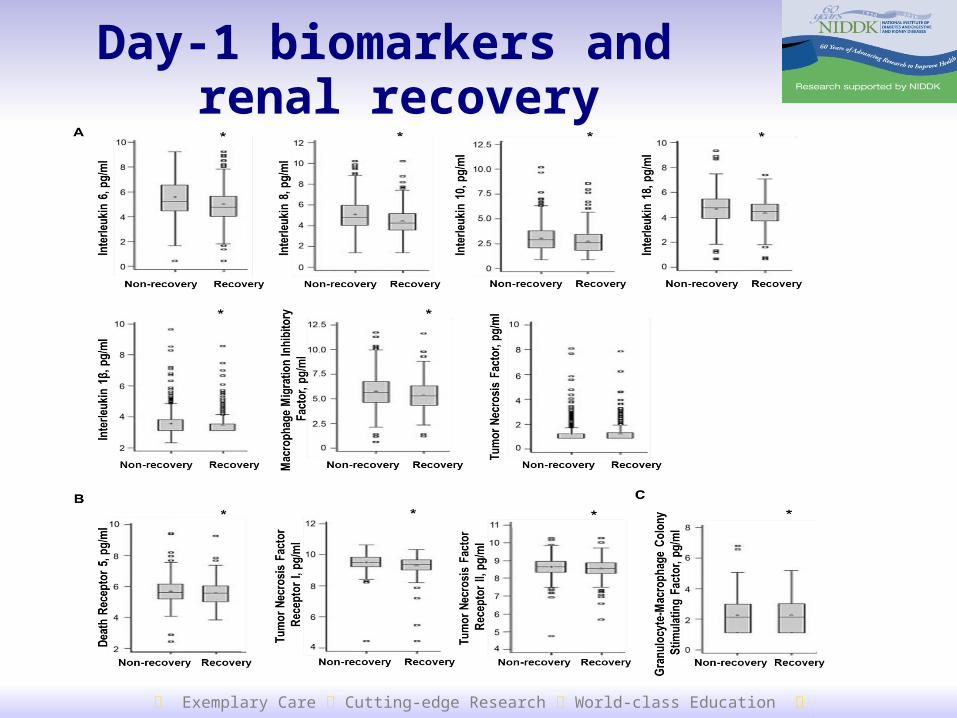
BioMaRK Study
Ancillary observational study to VA/ATN trial
Enrolled 819 critically ill subjects receiving RRT
Plasma biomarkers were sampled on days 1 and 8 after randomization in
inflammatory (IL-1,6,8,10,18,TNF,MIF)apoptosis (DR-5, TNFR-I, II)growth factor pathways (GM-CSF)
Outcome at day-60Renal recovery (alive and independent from RRT): 36%Mortality: 50%
Exemplary Care Cutting-edge Research World-class Education
Day-1 biomarkers and renal recovery

Exemplary Care Cutting-edge Research World-class Education
Inflammatory and apoptotic pathwaysand renal Recovery
Adjusted HR for renal recovery (95%CI)
IL-8: 0.84 (0.76-0.93)
IL-18: 0.88 (0.79-0.98)
TNFR-I: 0.84 (0.71-0.99)
Exemplary Care Cutting-edge Research World-class Education
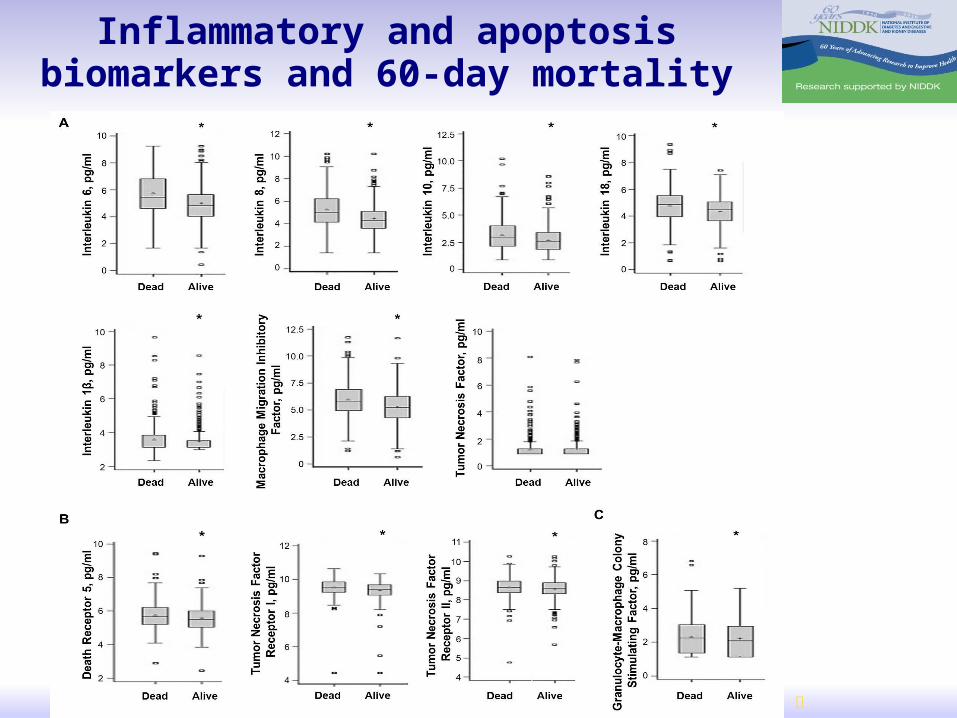
Inflammatory and apoptosis biomarkers and 60-day mortality

Exemplary Care Cutting-edge Research World-class Education
Inflammatory and apoptosis biomarkers and time to death
Adjusted HR (95%CI)IL-6: 1.26 (1.18-1.35)IL-8: 1.39 (1.29-1.51)
IL-18: 1.27 (1.14 -1.41)TNFR-I: 1.57 (1.22-2.02)
MIF: 1.16 (1.08-1.25)

Exemplary Care Cutting-edge Research World-class Education
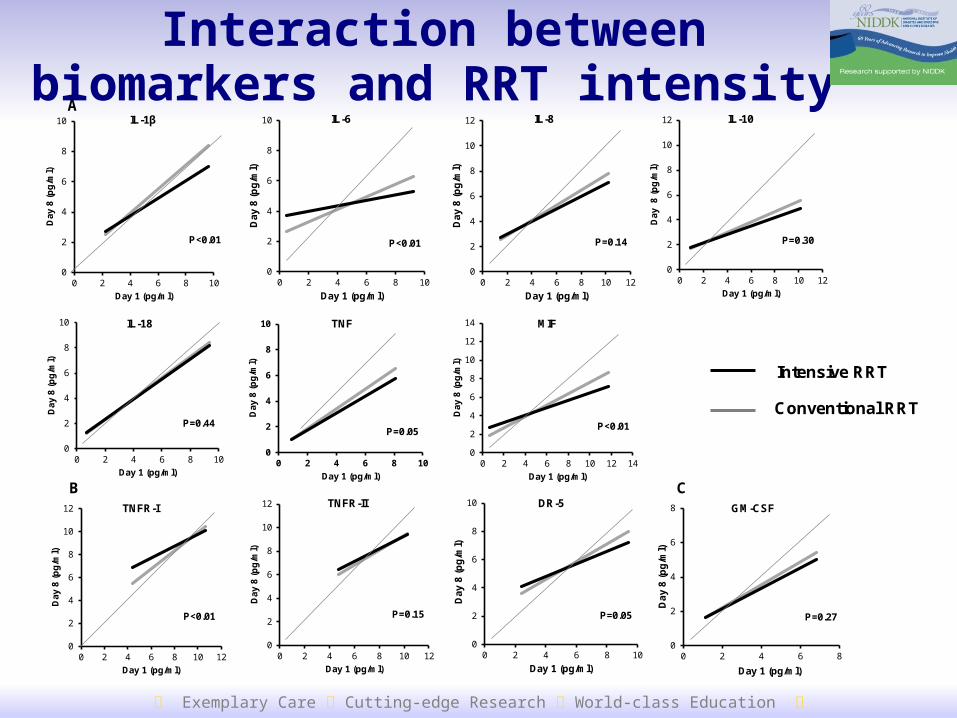
Biomarker concentration and intensity of RRT
Exemplary Care Cutting-edge Research World-class Education
Interaction between biomarkers and RRT intensity
0
2
4
6
8
10
0 2 4 6 8 10
Da
y 8
(p
g/m
l)
Day 1 (pg/ml)
IL-6
P<0.01
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Da
y 8
(p
g/m
l)
Day 1 (pg/ml)
IL-8
P=0.14
0
2
4
6
8
10
0 2 4 6 8 10
Day
8 (
pg
/ml)
Day 1 (pg/ml)
IL-1β
P<0.01
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Day
8
(pg
/ml)
Day 1 (pg/ml)
IL-10
P=0.30
0
2
4
6
8
10
0 2 4 6 8 10
Day
8 (
pg
/ml)
Day 1 (pg/ml)
IL-18
P=0.44
0
2
4
6
8
10
0 2 4 6 8 10
Day
8 (
pg
/ml)
Day 1 (pg/ml)
TNF
P=0.05
0
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14D
ay 8
(p
g/m
l)
Day 1 (pg/ml)
MIF
P<0.01
A
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Day
8 (
pg
/ml)
Day 1 (pg/ml)
TNFR-I
P<0.01
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Day
8 (
pg
/ml)
Day 1 (pg/ml)
TNFR-II
P=0.15
0
2
4
6
8
10
0 2 4 6 8 10
Da
y 8
(p
g/m
l)
Day 1 (pg/ml)
DR-5
P=0.05
B C
0
2
4
6
8
0 2 4 6 8D
ay
8 (
pg
/ml)
Day 1 (pg/ml)
GM-CSF
P=0.27
Intensive RRT
Conventional RRT

Exemplary Care Cutting-edge Research World-class Education
Association between intensive RRT and outcomes by day 1 marker levels
BiomarkerAdjusted Odds Ratio (95% CI)
Renal Recovery Mortality
IL-6 0.78 (0.55 - 1.10) 1.14 (0.81 – 1.59)
IL-8 0.82 (0.58 – 1.16) 1.09 (0.78 – 1.54)
IL-10 0.78 (0.56 – 1.11) 1.14 (0.82 – 1.60)
IL-18 0.76 (0.54 – 1.08) 1.20 (0.86 – 1.68)
MIF 0.77 (0.54 – 1.09) 1.20 (0.85 – 1.68)
TNFR-I 0.78 (0.55 – 1.11) 1.15 (0.82 – 1.60)
TNFR-II 0.79 (0.56 – 1.11) 1.15 (0.82 – 1.60)
DR-5 0.78 (0.55 – 1.10) 1.18 (0.84 – 1.65)
Exemplary Care Cutting-edge Research World-class Education
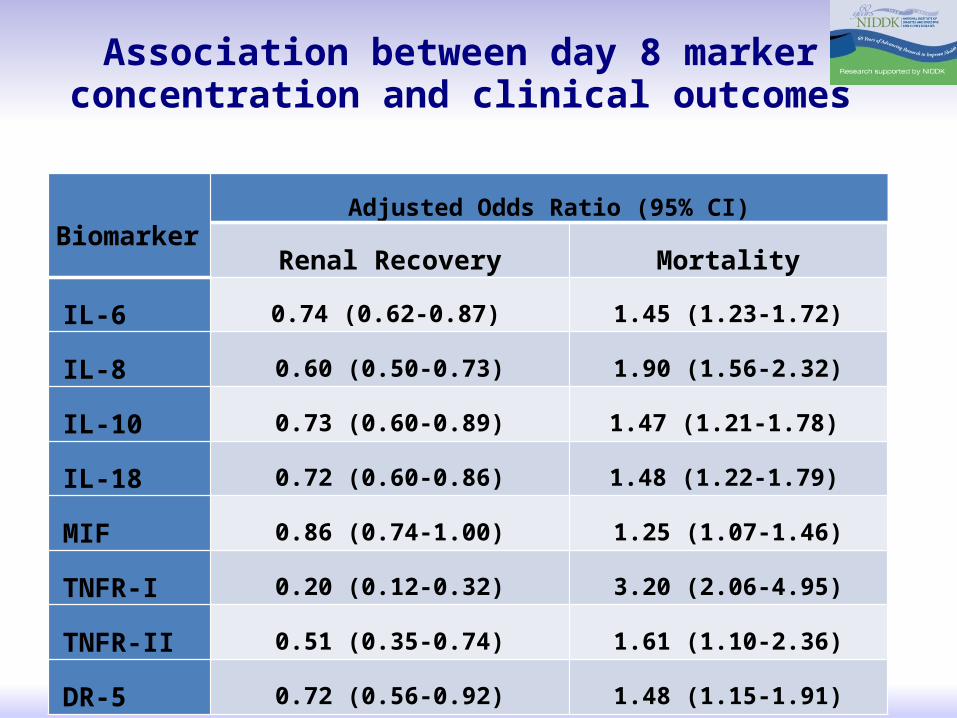
Association between day 8 marker concentration and clinical outcomes
BiomarkerAdjusted Odds Ratio (95% CI)
Renal Recovery Mortality
IL-6 0.74 (0.62-0.87) 1.45 (1.23-1.72)
IL-8 0.60 (0.50-0.73) 1.90 (1.56-2.32)
IL-10 0.73 (0.60-0.89) 1.47 (1.21-1.78)
IL-18 0.72 (0.60-0.86) 1.48 (1.22-1.79)
MIF 0.86 (0.74-1.00) 1.25 (1.07-1.46)
TNFR-I 0.20 (0.12-0.32) 3.20 (2.06-4.95)
TNFR-II 0.51 (0.35-0.74) 1.61 (1.10-2.36)
DR-5 0.72 (0.56-0.92) 1.48 (1.15-1.91)

Exemplary Care Cutting-edge Research World-class Education
ConclusionsIn CAP
inflammation is associated with AKI susceptibilityAKI is associated with increased short and long term mortalityone-third of patients receiving RRT during hospitalization following CAP develop ESRDcardiovascular disease accounts for one-third of all deaths in patients with AKI
In critically Ill patients receiving RRTincreased day-1 plasma inflammatory (IL-8, IL-18) and apoptosis (TNFR-I) are associated with RRT dependence plasma IL-6, 8, 18, MIF, TNFR-I are associated with mortalityoverall
no association between RRT intensity and biomarkers and outcomessignificant interaction exists within subgroup of patients with high and low day-1 concentrations
persistently elevated concentrations of these markers are associated with death and RRT dependence