? By Shelley Ferrell Advisor: Eileen VanDyke, PA-C PAS Spring 2006.
25
? By Shelley Ferrell Advisor: Eileen VanDyke, PA-C PAS Spring 2006
-
Upload
erin-pierce -
Category
Documents
-
view
222 -
download
2
Transcript of ? By Shelley Ferrell Advisor: Eileen VanDyke, PA-C PAS Spring 2006.

?By Shelley Ferrell
Advisor: Eileen VanDyke, PA-C
PAS Spring 2006

Behind door #1…
• 20 yo white female
• CC: menstrual irregularity over past year, no period in 5 months
• PE: obesity, acne, hirsutism
• Labs: (-) HCG, (+) hyperandrogenemia, (+) insulin resistance
• Diagnosis: ?

Behind door #2
• 21 yo white female
• CC: menstrual irregularity over past year, no period in 5 months
• PE: thin, mild acne, unremarkable
• Labs: (-) HCG, (+) hyperandrogenemia, (-) insulin resistance
• Diagnosis: ?
Treatment options
• Patient #1- Consider Metformin
• Patient #2- No obesity, no IR… Metformin???

The Use of Metformin in Non-obese Women with
Polycystic Ovarian Syndrome
By Shelley Ferrell
Advisor: Eileen VanDyke, PA-C
PAS Spring 2006

Why care about PCOS?
• Its common
• It causes other health problems
• It is emotionally painful for women

Making the diagnosis
• Two out of three
– Oligo and/or an-ovulation
– Clinical and/or biochemical hyperandrogenemia
– Polycystic ovaries on ultrasound
• Diagnosis of exculsion
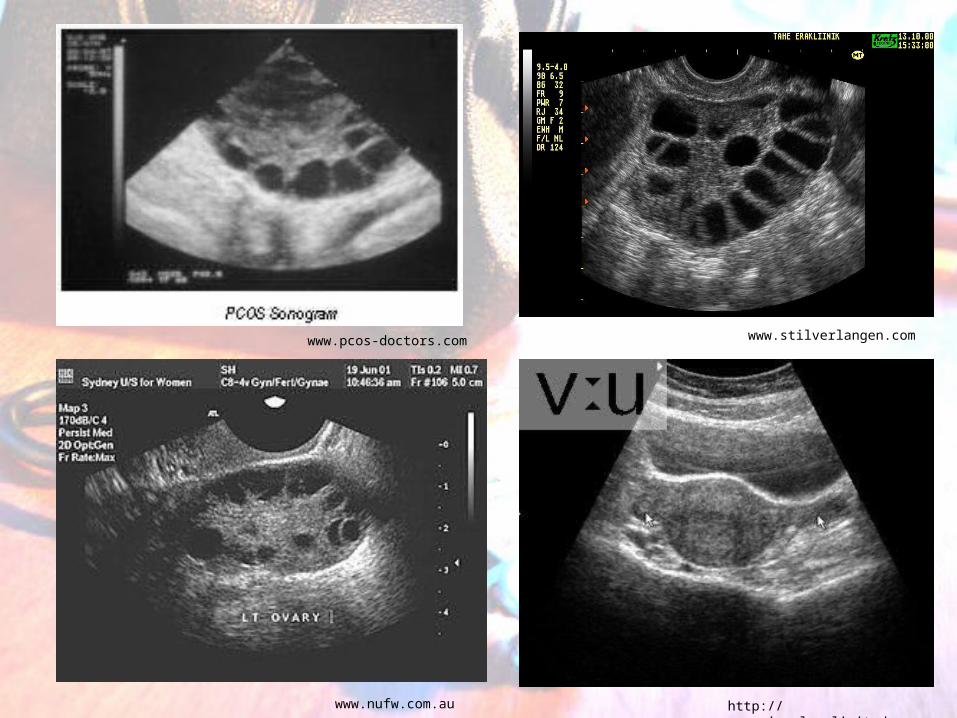
http://www.visualsunlimited.com
www.stilverlangen.com
www.nufw.com.au
www.pcos-doctors.com
Clinical Presentation• Is there a stereotypical PCOS patient?
Sign PrevalencePolycystic Ovaries 80-100%Oligo- or amenorrhea 70%Hyperandrogenism 20-80%Hirsutism 70%Obesity 50%Increased LH 30-90% Insulin Resistance 20-50%Acne 33%
• Other symptoms occur more rarely• Obesity makes a difference

Pathophysiology

Pathophysiology
• Three Theories:– Ovarian hypothesis
– Central hypothesis
– Insulin hypothesis
• Role of obesity in pathogenesis
• Obesity status/ IR status makes difference
Treatment Options
• Obese- weight loss!
• Non-obese- OCPs, anti-androgens, insulin-sensitizers
• Drawbacks to each
• Benefits of metformin
• Remember the initial question for Patient #2:– Do non-obese pts benefit from metformin? What if they
are not insulin resistant?
Lean Women with Polycystic Ovary Syndrome Respond to Insulin Reduction with Decreases in
Ovarian P450c17{alpha} Activity and Serum Androgens
• Nestler et al, 1997
• 31 normal weight women
• 1500 mg day metformin vs placebo, 4-6 wks
• Drop in serum sex steroids – (total T ↓48%, free T ↓70% and androstenedione ↓ 36%)
• Conclusions: Non-obese PCOS patients benefit from metformin treatment
Non-obese women with polycystic ovary syndrome respond better than obese women to
treatment with metformin
• Maciel et al, 2004
• 29 women in 2 groups: obese and non-obese
• Metformin 1500 g/day vs placebo, 6 months
• Results– Non-obese: ↑menstrual cyclicity, total T↓ 38%, free T
↓58%, androstendione↓30%
– Obese: total T ↓48%, otherwise no change
• Conclusions: Non-obese women experience more benefit than obese women with metformin txt

Effects of metformin and rosiglitazone, alone and in combination, in non-obese women with
polycystic ovary syndrome and normal indices of insulin sensitivity
• Baillargeon et al, 2004
• 100 non-obese women with normal insulin sens
• 1700 mg of metformin, 8 mg of rosiglitazone, a combination of both drugs or placebo daily for 6 months
• Results (met vs placebo): ovulation 6x more common, 100% ovulating monthly by study end- vs 10% placebo, sex steroids ↓67%
• Conclusions: Metformin benefits non-obese pts without IR

Metformin-diet benefits in women with polycystic ovary syndrome in the bottom and top quintiles for
insulin resistance
• Goldenberg et al, 2005
• 67 women in top and bottom quintiles for IR out of screening of 898 PCOS pts (all weights!)
• 2550 mg/day of metformin for 1 year + diet
• Results: menstruation doubled in non-IR
• Conclusion: metformin benefits non-IR
(many non-obese are also non-IR)
Predictive value of glucose-insulin ratio in PCOS and profile of women who will benefit from metformin therapy: Obese, lean, hyper or
normoinsulinemic?
• Onalan et al, 2005• 169 women into 6 groups based on glucose-insulin ratio
(normoinsulinemic and hyperinsulinemic) and BMI (lean, overweight and obese)
• 1700- 2550 mg/day of metformin (based on BMI) or placebo for 6 months
• Results: – IR/Lean group: ↑ ovulation, ↓ hirsutism– Both Lean groups, IR/obese group: ↓ Total T– No other significant results
• Conclusion: Pts who are both lean and IR benefit most from metformin therapy

Inconsistancy?
• Onalan did not show benefit to overweight women (still
considered non-obese)
Author Group Name Inclusion Criteria Average BMINestler Lean <23.7 21.6Maciel Non-obese <30 25.2 Baillargeon Non-obese <27 24.5 Onalan Lean <25 21.3
Overweight <30 28.2
• No inconsistancy- there may be an inverse relationship between BMI and response to metformin, even within non-obese or normal weight populations

Conclusion
• OCPs very effective
• Metformin should be considered also
• Talk to your patient- see what her goals are

If the intended result…

…isn’t quite achieved,
Yikes!

just try something else!
Find a treatment that the patient is satisfied with
Be sensitive to the effects that PCOS can have on self esteem
Let the patient know that there are websites and online groups for “cysters”

Bibliography• Allen H.F., C. Mazzoni, R.A. Heptulla R.A., et al. (2005) “Randomized controlled trial evaluating response to metformin versus standard therapy in
the treatment of adolescents with polycystic ovary syndrome.” J Pediatr Endocrinol Metab 18(8):761-8.• American College of Obstetricians and Gynecologists (2002). "Clinical Management Guidelines for Obstetrician--Gynecologists. Number 41,
December 2002: Polycystic Ovary Syndrome." Obstet Gynecol 100(6): 1389-1402.• Archer, J.S., R.J. Chang. (2004) “Hirsutism and acne in polycystic ovary syndrome.”
Best Pract Res Clin Obstet Gynaecol 18(5):737-54.•
• Baillargeon, J.P., D. J. Jakubowicz, et al. (2004). "Effects of metformin and rosiglitazone, alone and in combination, in non-obese women with polycystic ovary syndrome and normal indices of insulin sensitivity." Fertility and Sterility 82(4): 893.
•
• Baillargeon, J.P. and J. E. Nestler (2006). "Polycystic Ovary Syndrome: A Syndrome of Ovarian Hypersensitivity to Insulin?" J Clin Endocrinol Metab 91(1): 22-24.
•
• Balen, A. (2004). "The pathophysiology of polycystic ovary syndrome: trying to understand PCOS and its endocrinology." Best Practice & Research Clinical Obstetrics & Gynaecology 18(5): 685.
•
• Bhatia, V. (2005). "Insulin Resistance in Polycystic Ovarian Disease." Southern Medical Journal 98(9): 903-913.•
• Ciampelli, M., A.M. Fulghesu, F. Cucinelli, et al. (1999). "Impact of Insulin and Body Mass Index on Metabolic and Endocrine Variables in Polycystic Ovary Syndrome." Metabolism 48(2): 167-172.
• Cibula, D., M. Fanta, J. Vrbikova, et al. (2005) “The effect of combination therapy with metformin and combined oral contraceptives (COC) versus COC alone on insulin sensitivity, hyperandrogenaemia, SHBG and lipids in PCOS patients.” Hum Reprod 20(1):180-4.
•
• Deglin, J., A.H. Vallerand (2004). Davis' Drug Guide for Nurses. Philadelphia, F. A. Davis Company.• Dereli, D., T. Dereli, F. Bayraktar, et al. (2005). "Endocrine and Metabolic Effects of Rosiglitazone in Non-obese Women with Polycystic Ovary
Disease." Endocrine Journal 52(3): 299-308.•
• Diamanti-Kandarakis, E., K. Alexandraki, et al. (2005). "Metformin administration improves endothelial function in women with polycystic ovary syndrome." Eur J Endocrinol 152(5): 749-756.

BibliographyDiamanti-Kandarakis, E., J.-P. Baillargeon, et al. (2003). "A Modern Medical Quandary: Polycystic Ovary Syndrome, Insulin Resistance, and Oral Contraceptive Pills." J Clin Endocrinol Metab 88(5): 1927-1932.
Doi, S. A., P. A. Towers, et al. (2005). "PCOS: an ovarian disorder that leads to dysregulation in the hypothalamic-pituitary-adrenal axis?" European Journal of Obstetrics & Gynecology and Reproductive Biology 118(1): 4.
Elter, K., G. Imir and F. Durmusoglu. (2002) “Clinical, endocrine and metabolic effects of metformin added to ethinyl estradiol-cyproterone acetate in non-obese women with polycystic ovarian syndrome: a randomized controlled study.” Hum Reprod 17(7):1729-37.
Gennarelli, G., V. Rovei, et al. (2005). "Preserved Insulin Sensitivity and {beta}-Cell Activity, but Decreased Glucose Effectiveness in Normal-Weight Women with the Polycystic Ovary Syndrome." J Clin Endocrinol Metab 90(6): 3381-3386.
Goldenberg, Glueck, et al. (2005). "Metformin-diet benefits in women with polycystic ovary syndrome in the bottom and top quintiles for insulin resistance." Metabolism 54(1): 113.
Rotterdam consensus workshop group (2004). "Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome." Fertility and Sterility 81(1): 19.
Hann L.E., D.A. Hall, C.R. McArdle, et al. (1984). “Polycystic ovarian disease: sonographic spectrum.” Radiology 150(2): 531-4.
Hart, R., M. Hickey, et al. (2004). "Definitions, prevalence and symptoms of polycystic ovaries and polycystic ovary syndrome." Best Practice & Research Clinical Obstetrics & Gynaecology 18(5): 671.
Lam, P. M., L.P. Cheung, C. Haines (2004). "Revisit of metformin treatment in polycystic ovarian syndrome." Gynecologic Endocrinology 19: 33-39.Luque-Ramirez, M., J. L. San Millan, et al. "Genomic variants in polycystic ovary syndrome." Clinica Chimica Acta In Press, Corrected Proof.
Maciel, G. A., J. M. Soares Junior, et al. (2004). "Non-obese women with polycystic ovary syndrome respond better than obese women to treatment with metformin." Fertility and Sterility 81(2): 355.
Morin-Papunen, L., I. Vauhkonen, R. Koivunen, et al. (2003). “Metformin Versus Ethinyl Estradiol-Cyproterone Acetate in the Treatment of Nonobese Women with
Bibliography• Polycystic Ovary Syndrome: A Randomized Study.” J Clin Endocrinol Metab 88(1):148-56.•
• Nestler, J. E. and D. J. Jakubowicz (1997). " J Clin Endocrinol Metab 82(12): 4075-4079.
• Onalan, G., U. Goktolga, et al. (2005). "Predictive value of glucose-insulin ratio in PCOS and profile of women who will benefit from metformin therapy: Obese, lean, hyper or normoinsulinemic?" European Journal of Obstetrics & Gynecology and Reproductive Biology 123(2): 204.
•
• Orio, F., Jr., S. Palomba, et al. (2005). "Improvement in Endothelial Structure and Function after Metformin Treatment in Young Normal-Weight Women with Polycystic Ovary Syndrome: Results of a 6-Month Study." J Clin Endocrinol Metab 90(11): 6072-6076.
• Palomba, S., F. Orio, Jr., et al. (2005). "Prospective Parallel Randomized, Double-Blind, Double-Dummy Controlled Clinical Trial Comparing Clomiphene Citrate and Metformin as the First-Line Treatment for Ovulation Induction in Non-obese Anovulatory Women with Polycystic Ovary Syndrome." J Clin Endocrinol Metab 90(7): 4068-4074.
• Premoli, A. C., L. F. Santana, et al. (2005). "Growth hormone secretion and insulin-like growth factor-1 are related to hyperandrogenism in non-obese patients with polycystic ovary syndrome." Fertility and Sterility 83(6): 1852.
•
• Salehi, M., R. Bravo-Vera, et al. (2004). "Pathogenesis of polycystic ovary syndrome: what is the role of obesity?" Metabolism 53(3): 358.
• Velásquez, E.M., S. Mendoza, T. Hamer, et al. (1994) “Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy.” Metabolism 43(5):647-54.
•
• VrbIkova, J., D. Cibula, et al. (2004). "Insulin Sensitivity in Women with Polycystic Ovary Syndrome." J Clin Endocrinol Metab 89(6): 2942-2945.
•
•