بسم الله الرحمن الرحيم
37
1
-
Upload
erich-oliver -
Category
Documents
-
view
207 -
download
10
description
بسم الله الرحمن الرحيم. بسم الله الرحمن الرحيم. BRONCHIAL ASTHMA. BY Mohamed Magdy Zedan Resident of Pediatric,Mansoura University Children Hospital. Definition :. It is a diffuse obstructive lung disease ,with 3 characteristics: High degree of reversibility - PowerPoint PPT Presentation
Transcript of بسم الله الرحمن الرحيم

1

2
BYMohamed Magdy ZedanResident of Pediatric,Mansoura
University Children Hospital

3
Definition:
It is a diffuse obstructive lung disease ,with 3 characteristics:
(1) High degree of reversibility
(spontaneously or with treatment).
(1)Airway inflammation ( corner stone of asthma).
(2)Bronchial hyper-reactivity.

4
Pathogenesis of Asthma:-
Lies in 3 steps:-
1- Transformation of TH0 to TH2.
2- Genesis of atopic state.
3- Allergic reactions.
5

6
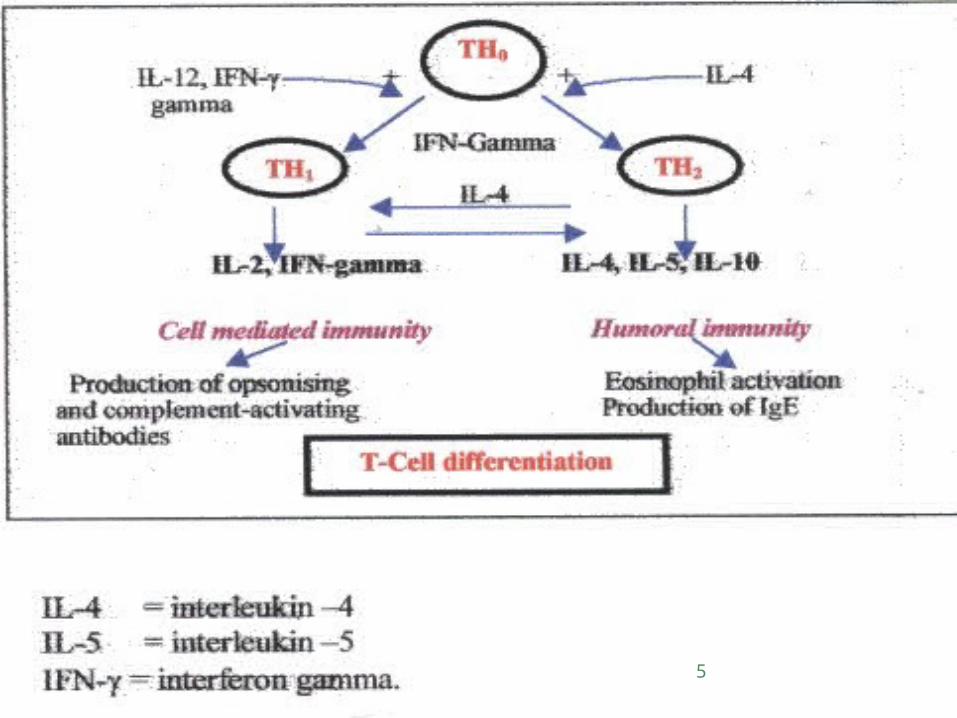
(1) Transformation of TH0 to TH2
T helper (CD4) lymphocytes are the maestro of the inflammatory process.TH0 is switched either to TH2 ( under the effect of IL-4) or TH1 ( under the effect of IL-12 and IFN-gamma).
TH1 is responsible for cell mediated immunity (normal immune response) whereas TH2 is responsible for humeral immunity (allergic reactions).The excess secretion of IL-4 results from disturbance in the long arm of chromosome no.5 , so the patient become phenotypically allergic (TH2 phenotype).

7
(2) Genesis of Atopic State
Inhaled allergen will be taken by APC that is homing in the airway.
Once APC presents the allergen to TH2 release of IL-4 &IL-5
a-IL-4 formation of IgE from B-lymphocytes fixed over the masts cells early allergic reaction.
b-IL-5growth, maturation, recruitment of the eosinophils to the airway late allergic reaction.

8
9
(3) Allergic Reactions 1- Early allergic reaction:-Occurs within 20 min from allergen exposure.Mediated by degranulation of the sensitized mast cells
with release of different mediators.Resulting in cough, bronchospasm, weal's and itching.
2- Late allergic reaction:-Occurs within 6-8 hours from allergen exposure.Mediated by eosinophils.Resulting in chronic wheeze,hyperactive airway and
nasal blockage.
10

11
12
(1) Asthma Symptoms:
Recurrent cough, wheeze, chest tightness, dyspnea.
These symptoms worsen at night and early morning and on exposure to a specific allergens.
These symptoms are variable and reversible and they are associated with reversible wide spread airflow obstruction.
13

14
(2) Asthma Exacerbations:
Asthma exacerbations are episodes of progressively worsening of asthma symptoms ,characterized by decrease in expiratory airflow.
These exacerbations usually reflects, a failure in long term management or exposure to a trigger.
Degree of asthma exacerbations is determined by: degree of wheeze, dyspnea and PEF value ( which is evaluated after the initial treatment with B2 –agonist every 20 min for one hour).

15
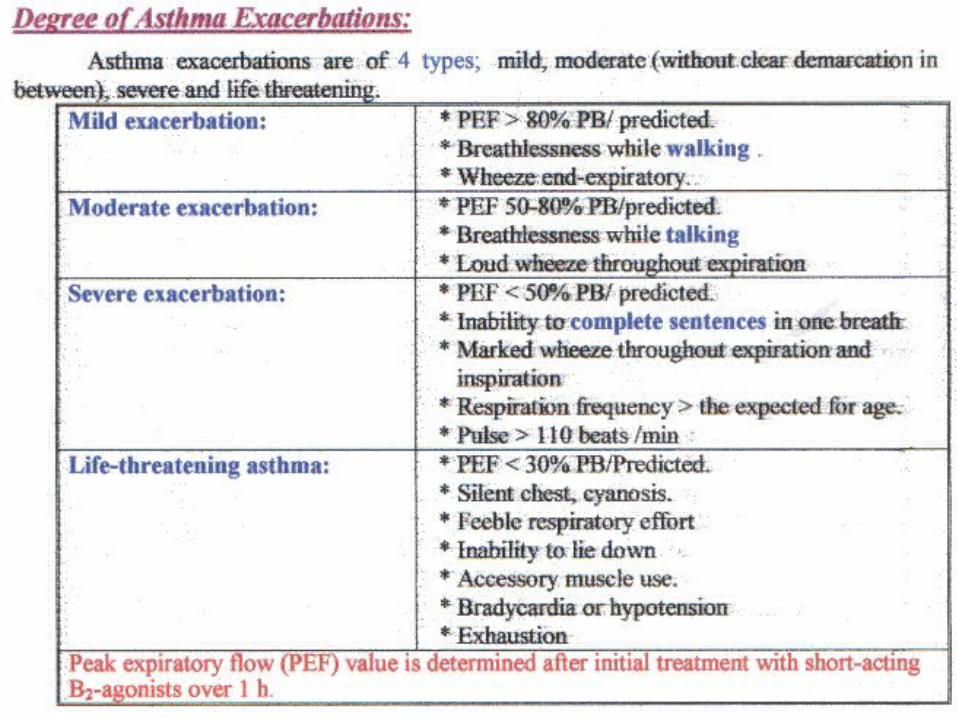
Degree of Asthma Exacerbations:
Mild exacerbation: - PEF > 80% PB/predicted. - Breathlessness while walking. - Wheeze end-expiratory.
Moderate exacerbation: - PEF 50-80% PB/predicted. - Breathlessness while talking. - Wheeze throughout expiration.
16
Sever exacerbation: -PEF <50% BP/predicted. -Inability to give complete sentences in one
breath -Marked wheeze throughout expiration and
inspiration. -Pulse > 110 beats/min.Life-threatening asthma: - PEF < 30% BP/predicted. - Inability to lie down. - Silent chest, cyanosis. - Bradycardia or hypo tension.

17
(3) Clinical types of Asthma:
* We have according to GINA guidelines 4 types Intermittent asthma and persistent asthma ( mild, moderate,sever).
* Basis for classification are: frequency of symptoms and level of pulmonary function and performance.

18
19
(4) Investigations
1- Chest x-ray.
2- CBC with differential: eosinophilia.
3- Serum IgG: total and specific.
4- Airway inflammatory markers: IL-2 receptors, ECP.
5- Pulmonary function test: FEV1 variability.
6- Skin test.

20
(4) Differential Diagnosis of Bronchial Asthma ( wheezy infant)
1- Laryngeal obstruction.2- F.B inhalation.3- Recurrent aspiration: a- Gastro-esophageal reflux. b- Disorders of swallowing (Neuromuscular disease).
4- Host defense defect: a- Cystic fibrosis, ciliary dyskinesia. b- Immuno-deficiency.
5- Cardiac asthma. Continue
21
6- Bronchiectasis.
7- Bronchiolitis oblitrans.
8-Developmental anomalies: a- Trachea-bronchial anomalies: 1- Tracheo-esophageal fistula.
2- Bronchomalacia.
3- Store-pipe trachea.
4- Bronchial compression:
- Vascular ring.
- Subclavian artery.
- Bronchial or pericardial cyst.
b- Congenital heart disease.
c- Granulomas or polyps.

22
23
Asthma medications have three categories:
I- Quick-relief medications.
II- Long term control medications.
III- Allergen immunotherapy.

24
I- Quick-relief medication (Rescue medications)
A- Inhaled short acting B2 agonist: - Albuterol (ventolin) or salbutamol (farcolin), it is
supplied as MDI (metered dose inhaler, 100mcg/puff)
or nebulizer solution (5mg/ml).
- Most effective and safe bronchdilator.
- Onset of action: 5-10 min following inhalation, with 4-6 hours of action.

25
- Dose: 0.15 mg/kg (minimum dose 2.5 mg = ½
ml & maximum dose of 5 mg = 1 ml).
- Side effects:
a- Tremors.
b- Tachycardia and palpitation (as a result of
hypotension caused by V.D)
c- Hpokalemia ( due to stimulation of Na/k pump)
d- Tolerance ( if given in large , frequent doses)
26
B- Anticholinergics
- Ipratropium bromide (atrovent), it is supplied as MDI or nebulizer solution ( 250 mcg/ml).
- Produce bronchodilatation , by antagonizing the activity of acetylcholine at the level of M3.
- Not sufficiently effective alone, used in addition to B2 agonist in sever exacerbation.
- Dose :- one unit dose ( 1ml / 6 hours ).

27
C- Systemic Corticosteroids
- Used when the patient not respond rapidly to bronchodilators.- Mode of action: They reduce bronchial inflammation & hyper- reactivity , through: 1- Anti-inflammatory effects:
- Inhibit PGs & LTs synthesis.
- Inhibit the release of inflammatory mediators. - Inhibit the release of proteolytic enzymes. - Reduce capillary permeability.
Continue -

28
2- Anti-allergic effects: - Inhibit cellular immunity. - Inhibit antibody formation. - Inhibit release of proteolytic enzymes.3- Potentiation of endogenous catecholamines: - Increase number of beta cells. - Decrease neuronal uptake of catecholamines.
- Dose:- Hydrocortisone (6mg/kg/6h , 1ml = 20 mg )
Methylprednisolone (1-2mg/kg/dose).
- Onset of action: Maximal response occur after 6 hours, but they start to reverse the tolerance to B2
agonist within one hour.

29
Mode of action: 1- Inhibit phosphodiesteraseIncrease c-AMP a- Bronchodilatation.b- Decrease release of bronchoconstrictor sub. From mast cells.2- Block adenosine receptors a- Bronchodilatation.b- Decrease release of histamine from mast cells.3- Increase sympathetic Bronchodilatation ,by :-a- Stimulate release of catecholamines.b- Inhibiting COMT.4- Increase diaphragmatic contraction & decrease respiratory
muscle fatigue.
D- Systemic bronchodilator therapy (aminophylline)

30
Dose: 6 mg/kg by I.V infusion.
Adverse effects: 1- C.N.S : Insomnia, irritability and convulsions.
2- C.V.S : Palpitation, tachycardia and arrhythmias.
3- G.I.T : Nausea, vomiting, diarrhea & intestinal bleeding.
4- Rapid I.V. Injection of aminophylline cause
hypo tension,syncope,arrhythmias and convulsions.

31
D- Subcutaneous epinephrine
Mode of action: a- Stimulation of B2 receptors Bronchodilatation.
b- Stimulation of α receptors decrease mucosal edema .
Dose: 0,01 mg/kg (maximum dose of 0.3 mg) every 20 minutes to a maximum 3 doses.

32
II- Long-term control medication (maintenance medications)
1- Inhaled corticosteroids.2- Leukotriene modifiers.3- Sodium cromoglycate and nedocromil.
4- Long-acting B2 agonists as : a- Formoterol (Foradil). b- Salmeterol (Serevent).5- Methylxanthines.

33
I-Inhaled corticosteroids:Action:- - Improve airflow obstruction.
- Improve lung functions.
- Improve daytime and nighttime symptoms.
- Improve airway hyper responsiveness and airway
remodeling
- They reduce frequency of exacerbations.
Side effects: - Sore throat,hoarseness of voice,candidate infection.
- Decrease bone density and growth.

34
Available inhaled steroids :- Beclomethasone dipropionate (Becotide). - Budesonide (pulmicort). - Fluticasone propionate (flixotide)

35
II- Leukotriene modifiers Two subclasses: a- 5-lipoxygenase inhibitors. b- Leukotriene receptor antagonist: - Montelukast. - Zafirlukast.Actions:a- Inhibition of exercise induced and aspirin induced
asthma. b- Bronchodilatation. c- Decrease need of steroid use in acute asthma. d- Decrease nocturnal and daily asthma exacerbations. e-Decrease mucus production.Dose: one chewable tab (5mg) once daily at bedtime.

36
III- Allergen immunotherapyIndications: 1- Unavoidable exposure to allergen to which the patient is
sensitive,such as house dust mites or pollens. 2- Symptoms occur allover the year. 3- Difficult in controlling symptoms with pharmacological
management.
Mechanism of action: Shift of TH2 asthma phenotype to TH1 normal immune- response.
Method: -Choose the proper patient with IgE mediated asthma. -Use one or maximum 3 allergens in the course. -The course usually 3-5 years on maintenance doses.

37