© 2007 McGraw-Hill Higher Education. All rights reserved. Chapter 1 Normal Physiology: Exercise.
33
2007 McGraw-Hill Higher Education. All rights reserved. Chapter 1 Normal Physiology: Exercise
-
Upload
miranda-cole -
Category
Documents
-
view
215 -
download
0
Transcript of © 2007 McGraw-Hill Higher Education. All rights reserved. Chapter 1 Normal Physiology: Exercise.

© 2007 McGraw-Hill Higher Education. All rights reserved.
Chapter 1Normal Physiology:
Exercise

© 2007 McGraw-Hill Higher Education. All rights reserved.
Topics
• Oxygen consumption• Respiratory muscles• Diffusion; blood-gas barrier• Pulmonary circulation• Cardiac output• Oxygen transport• Carbon dioxide transport• Blood-tissue gas exchange

© 2007 McGraw-Hill Higher Education. All rights reserved.
Case Study #1: Ann• Young, highly trained Cyclist
• High Vo2 max
– What contributes to this?• Pulmonary Ventilation• Gas diffusion• Pulmonary blood flow• Oxygen transport in the blood
• Blood-myocyte O2 exchange

© 2007 McGraw-Hill Higher Education. All rights reserved.
Case Study #1: Ann
0
0.5
1
1.5
2
2.5
3
3.5
4
0 100 200 300 400
Watts
Vo 2
(L/m
in)
0123456789
10
0 1 2 3 4
0
20
40
60
80
100
120
140
160
0 1 2 3 4
Vo2 (L/min)
BLa
- (m
mol
)V
E o
r Q
(L/
min
)
Note the magnitude of increase in each variable
Vo2: ↑~15 fold
VE: ↑ ~10 fold
Q: ↑ ~ 5 fold
BLa: ↑ 10 fold

© 2007 McGraw-Hill Higher Education. All rights reserved.
How Does Ann Increase Her Metabolic Rate So Much?
• Coordinated systems approach– Lung, heart, CV system and skeletal
muscle all work in concert– Disease in any area will reduce functional
capacity markedly– COPD, heart disease, CV disease,
metabolic disease and musculoskeletal disease will ALL reduce functional capacity

© 2007 McGraw-Hill Higher Education. All rights reserved.
Ventilation: How gas gets to the alveoli
• Diaphragm:– Thin dome-shaped sheet of muscle
attached to lower rib cage and spine– Acts like a piston in a flexible
cylinder– Compresses abdominal contents;
increases vertical dimension of thorax
– Increases antero-lateral dimensions of thorax as well
– Innervated by Phrenic n. (C3-5)– *Only muscle that is active at rest*

© 2007 McGraw-Hill Higher Education. All rights reserved.
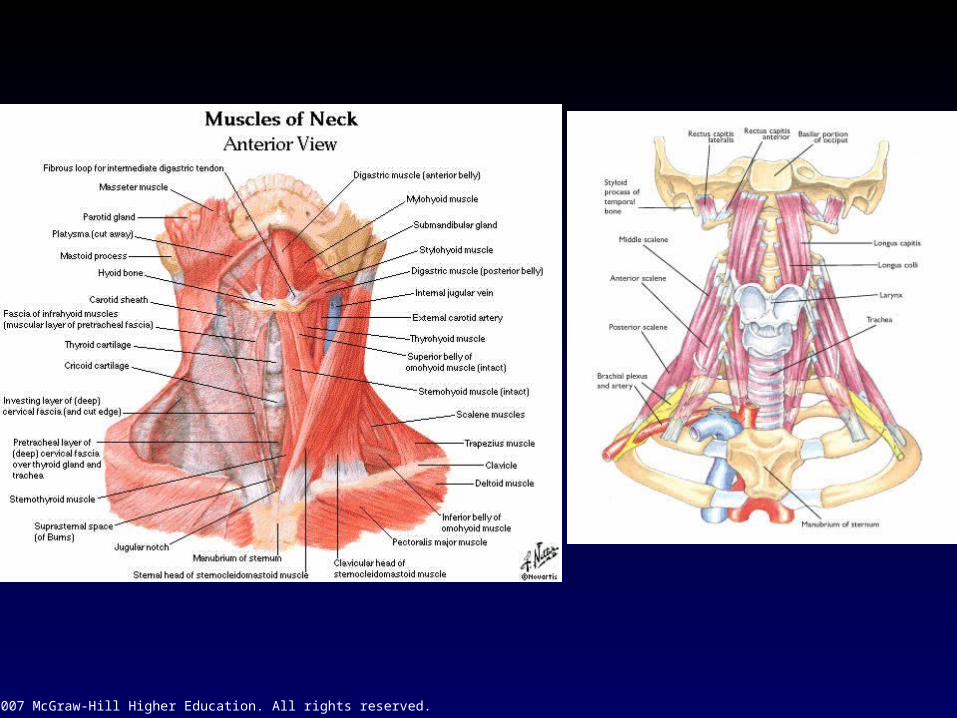
• External intercostals:– Inspiration; pull ribs up and
out– Increase in lateral
dimensions: “bucket handle” movement
– Intercostal nn.– Accessory muscles of
inpiration:• Scalenes• Sternocleidomastoid
Inspiration-Expiration: Muscles
© 2007 McGraw-Hill Higher Education. All rights reserved.
© 2007 McGraw-Hill Higher Education. All rights reserved.
Inspiration-Expiration: Muscles• Expiration:
– Passive at rest; why?• Chest wall and lung have elastic properties
– During exercise:• Becomes active; why?
– Large volumes have to be moved– Accessory muscles of expiration
» Abdominals: increase intra-abdominal pressure
» Internal intercostals: pull ribs down and in; stiffens rib cage
© 2007 McGraw-Hill Higher Education. All rights reserved.
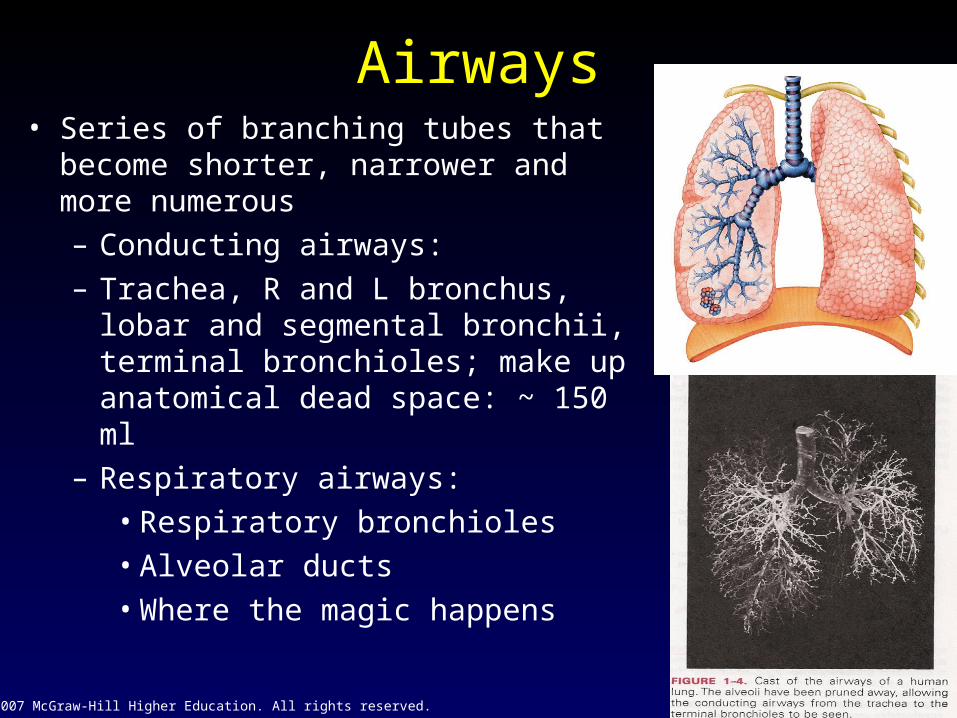
Airways• Series of branching tubes that become
shorter, narrower and more numerous– Conducting airways: – Trachea, R and L bronchus, lobar and
segmental bronchii, terminal bronchioles; make up anatomical dead space: ~ 150 ml
– Respiratory airways:• Respiratory bronchioles• Alveolar ducts• Where the magic happens
© 2007 McGraw-Hill Higher Education. All rights reserved.
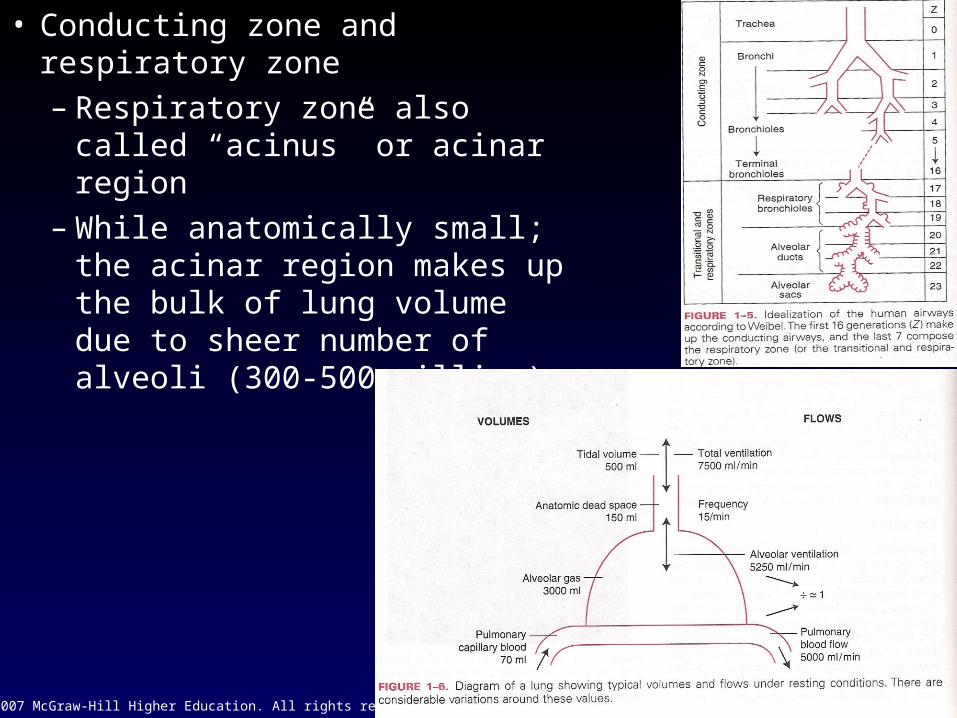
• Conducting zone and respiratory zone– Respiratory zone also called
“acinus” or acinar region– While anatomically small; the
acinar region makes up the bulk of lung volume due to sheer number of alveoli (300-500 million)
© 2007 McGraw-Hill Higher Education. All rights reserved.
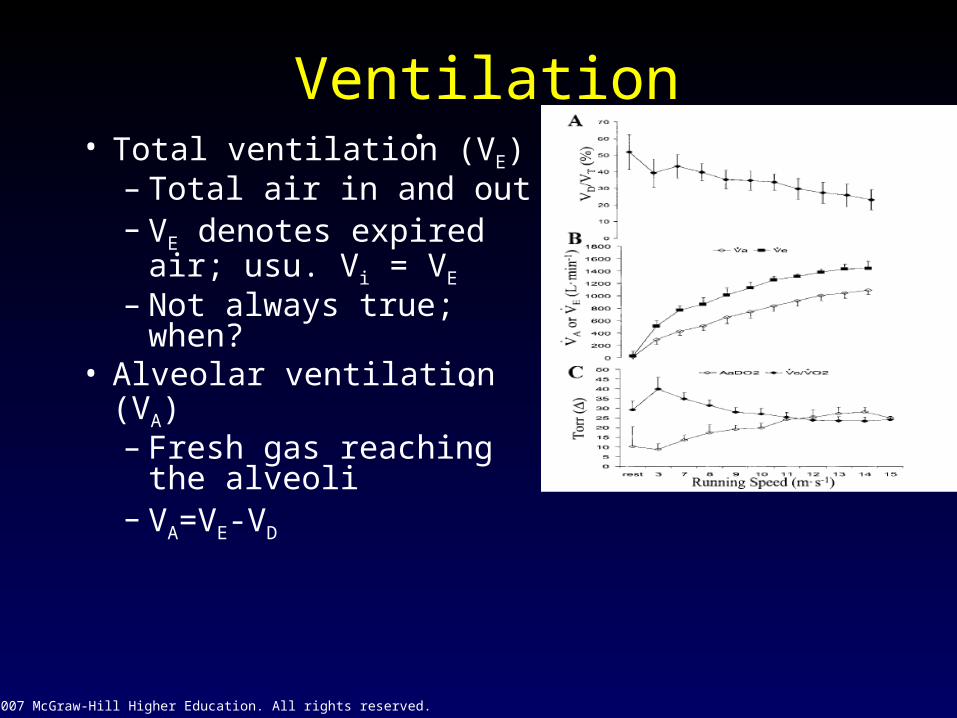
Ventilation• Total ventilation (VE)
– Total air in and out– VE denotes expired
air; usu. Vi = VE
– Not always true; when?
• Alveolar ventilation (VA)– Fresh gas reaching
the alveoli– VA=VE-VD
.
.
© 2007 McGraw-Hill Higher Education. All rights reserved.
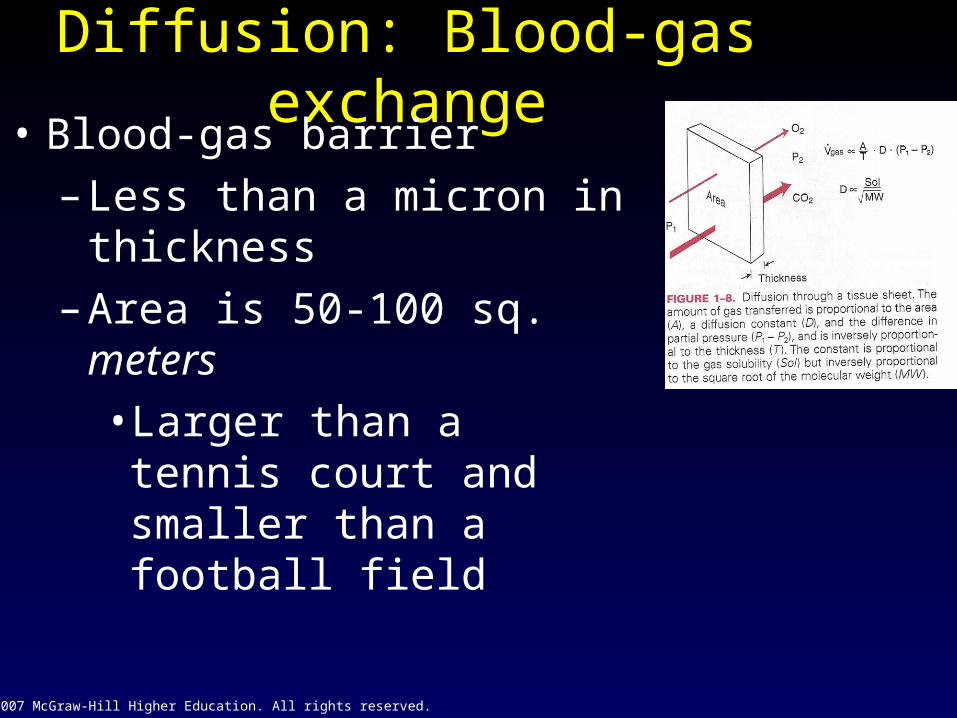
Diffusion: Blood-gas exchange• Blood-gas barrier
– Less than a micron in thickness
– Area is 50-100 sq. meters
• Larger than a tennis court and smaller than a football field
© 2007 McGraw-Hill Higher Education. All rights reserved.
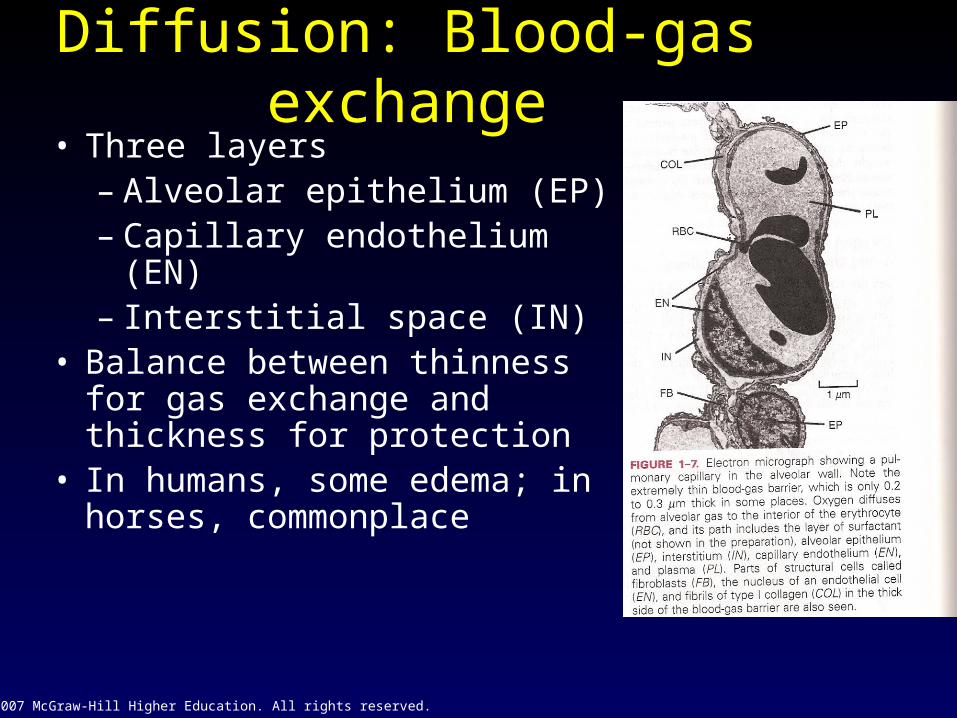
• Three layers– Alveolar epithelium (EP)– Capillary endothelium (EN)– Interstitial space (IN)
• Balance between thinness for gas exchange and thickness for protection
• In humans, some edema; in horses, commonplace
Diffusion: Blood-gas exchange

© 2007 McGraw-Hill Higher Education. All rights reserved.

© 2007 McGraw-Hill Higher Education. All rights reserved.
Principles of diffusion• ALL gases pass across the lung by simple diffusion• Fick’s Law:
– Volumetric rate of transfer of a gas is proportional to tissue area and the pressure difference between the two sides and inversely proportional to the tissue thickness
– Also dependent upon a constant, which is the diffusibilty of the particular gas in question
• D is proportional to the gases solubility and inversely proportional to it’s MW
– Co2 diffuses across the B-G barrier about 20 times as quickly due to it’s higher solubility
– What does this mean in practical terms?
© 2007 McGraw-Hill Higher Education. All rights reserved.
Oxygen Uptake along pulmonary capillary
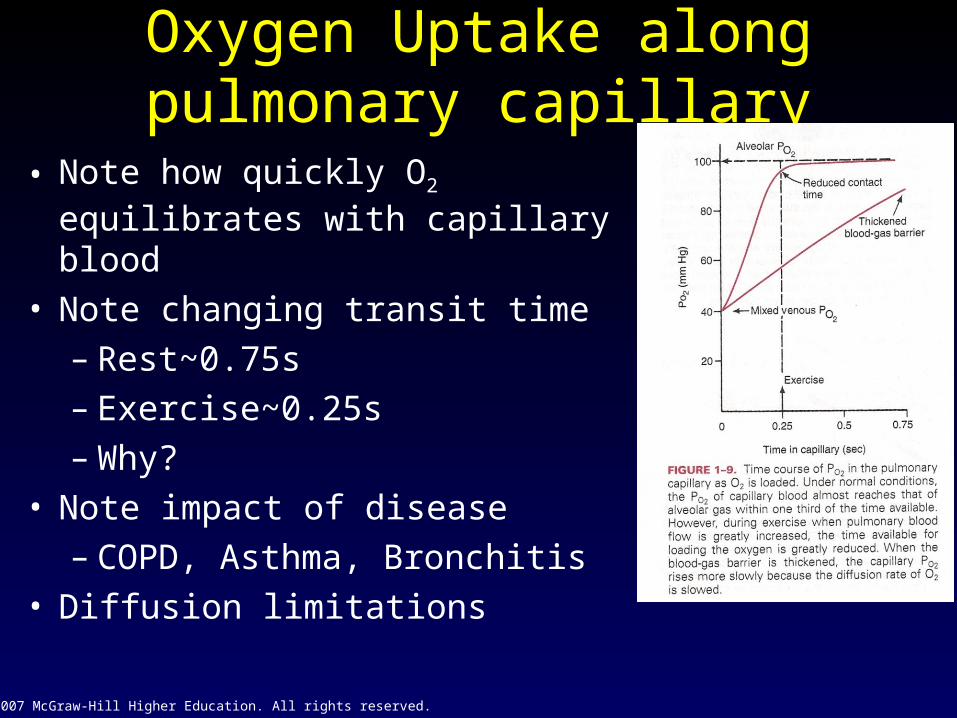
• Note how quickly O2 equilibrates with capillary blood
• Note changing transit time– Rest~0.75s– Exercise~0.25s– Why?
• Note impact of disease– COPD, Asthma, Bronchitis
• Diffusion limitations

© 2007 McGraw-Hill Higher Education. All rights reserved.
Diffusion limitations

© 2007 McGraw-Hill Higher Education. All rights reserved.
Pulmonary Blood Flow• R ventricle → Pulmonary artery → Pulm.
Capillaries → pulmonary veins → LA atrium → L ventricle → Aorta
• Pressures– In Humans: Low– Mean Ppa in horse ~100 mmHg– In Dog ~40 mmHg– Poisseuile’s law
• R=[Kℓη]/r4
• P=Q*R• So, pulmonary circulation is low resistance• In animals with high pulmonary pressures
– High Q– Elevated Pulm resistance
© 2007 McGraw-Hill Higher Education. All rights reserved.
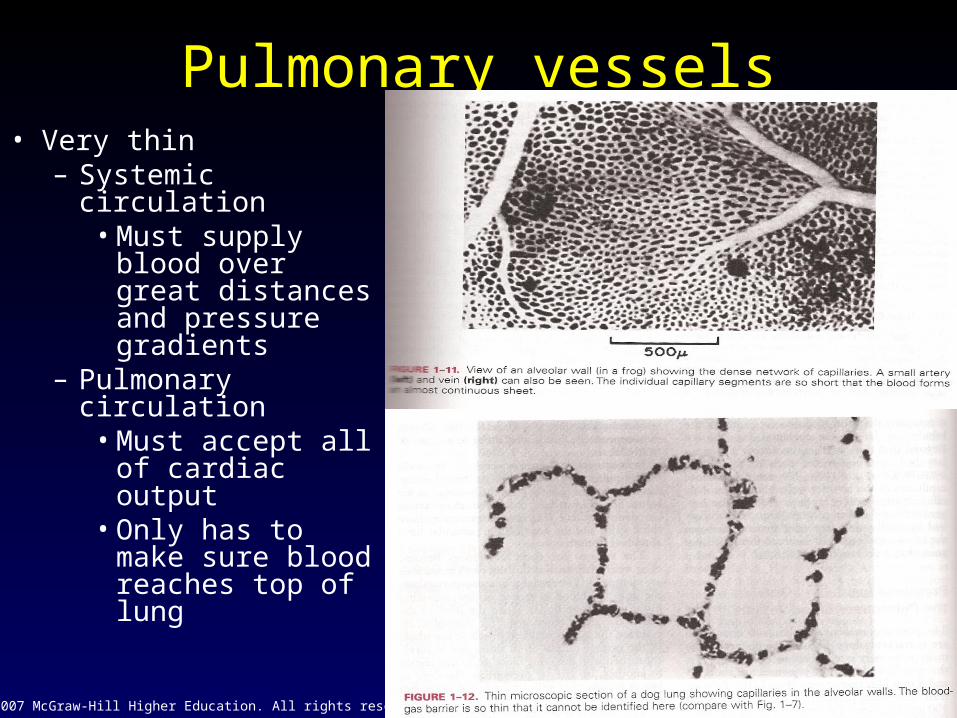
Pulmonary vessels• Very thin
– Systemic circulation• Must supply
blood over great distances and pressure gradients
– Pulmonary circulation
• Must accept all of cardiac output
• Only has to make sure blood reaches top of lung
© 2007 McGraw-Hill Higher Education. All rights reserved.
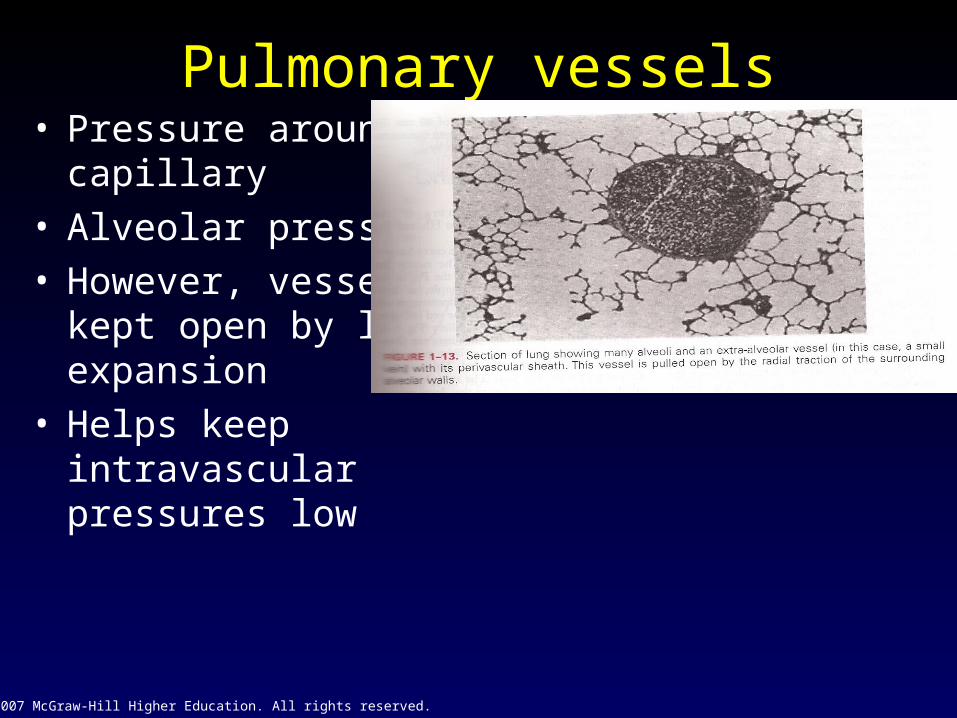
• Pressure around capillary
• Alveolar pressure• However, vessels kept
open by lung expansion
• Helps keep intravascular pressures low
Pulmonary vessels

© 2007 McGraw-Hill Higher Education. All rights reserved.
Cardiac Output• All of cardiac output goes through pulmonary circuit• Qc at rest is 5-6 L/min• Can increase to 25 L/min or more during maximal exercise• Can be measured using the Fick principle of Mass balance
– Q = Vo2/[a-vO2 diff]
– Vo2 = 3.5 L/min; CaO2 = 200 ml/L; CvO2 = 60 ml/L
• 3500ml/min ÷ [200-60]• 25 L/min
• Often, a non-invasive rebreathing method (acetylene rebreathing) is used; amount of soluble gas diffused is dependent (as thus proportional to) in this case upon blood flow
© 2007 McGraw-Hill Higher Education. All rights reserved.
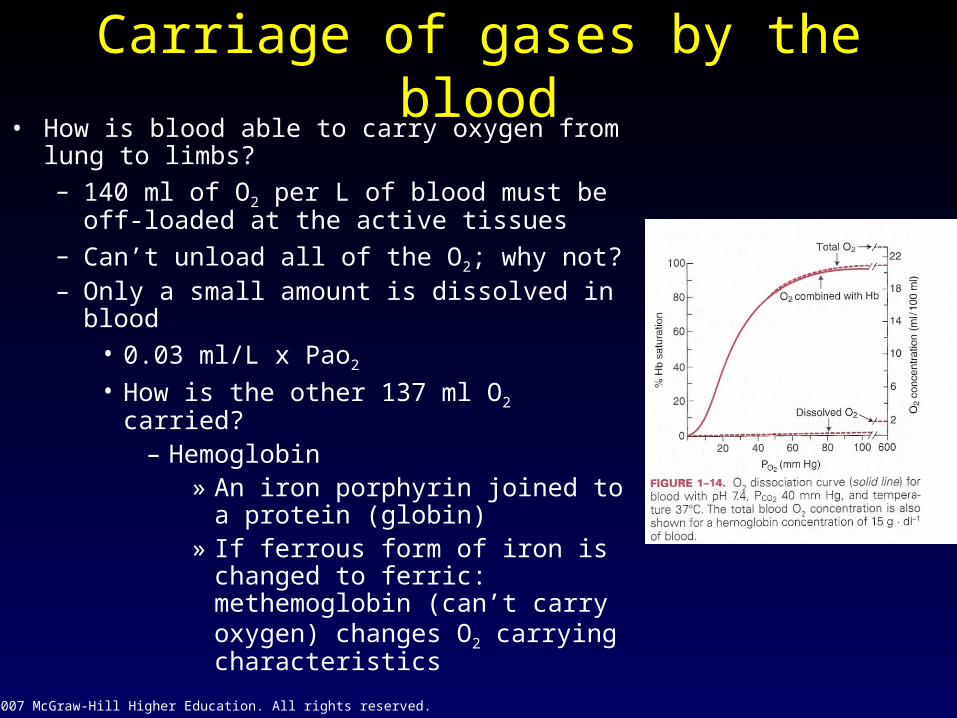
Carriage of gases by the blood• How is blood able to carry oxygen from lung to
limbs?– 140 ml of O2 per L of blood must be off-loaded
at the active tissues– Can’t unload all of the O2; why not?– Only a small amount is dissolved in blood
• 0.03 ml/L x Pao2
• How is the other 137 ml O2 carried?– Hemoglobin
» An iron porphyrin joined to a protein (globin)
» If ferrous form of iron is changed to ferric: methemoglobin (can’t carry oxygen) changes O2 carrying characteristics
© 2007 McGraw-Hill Higher Education. All rights reserved.
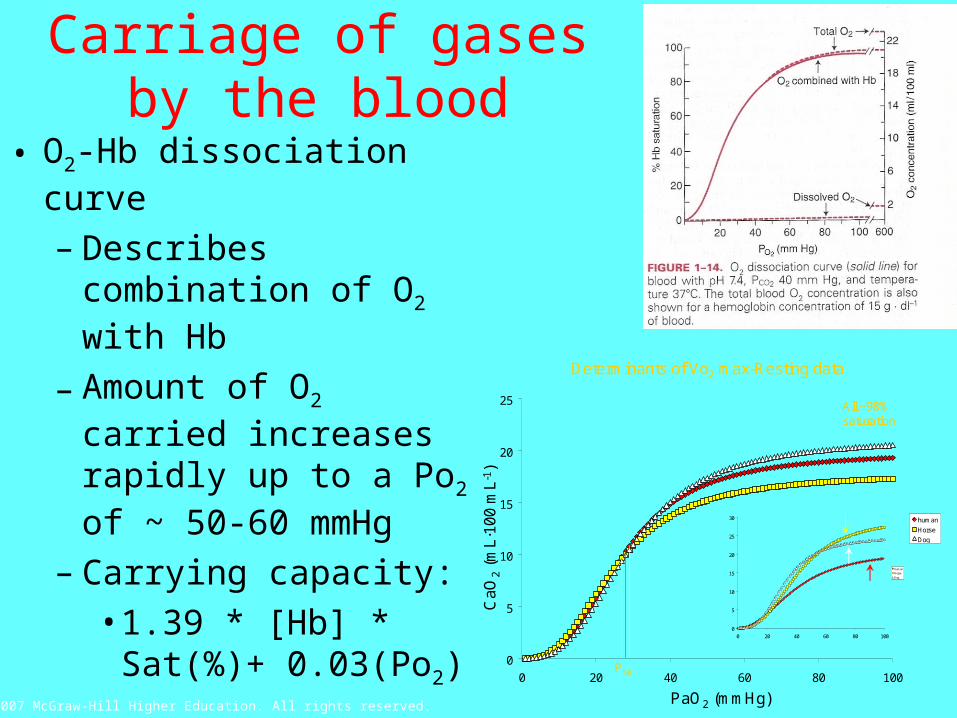
• O2-Hb dissociation curve
– Describes combination of O2 with Hb
– Amount of O2 carried increases rapidly up to a Po2 of ~ 50-60 mmHg
– Carrying capacity:• 1.39 * [Hb] * Sat(%)
+ 0.03(Po2)
Carriage of gases by the blood
0
5
10
15
20
25
0 20 40 60 80 100
human
Horse
Dog
Determinants of Vo2 max-Resting data
All ~98% saturation
CaO
2(m
L·1
00 m
L-1
)
PaO2 (mmHg)
P50
0
5
10
15
20
25
30
0 20 40 60 80 100
Human
Horse
Dog

© 2007 McGraw-Hill Higher Education. All rights reserved.
• So, maximal capacity of Hb– 1.39 ml O2/g Hb * [150g/l]*
100% - 0.03 (100) = ~208 ml/L– 1.39 is ideal, usu. About 1.34
due to methemoglobin, COHb and various other inactive forms of Hb
– Shape is ideal for O2 carrying molecule and is due to a property called cooperative binding
– Curve can be “shifted” by various physiological conditions
• Temperature• pH• Pco2
• 2,3 DPG– First 3 all result during exercise– 2,3 DPG is elevated at altitude
(due to chronic hypoxia)– P50: pressure at which blood is
50% saturated
© 2007 McGraw-Hill Higher Education. All rights reserved.
Oxygen transport• Carbon monoxide (CO)
– Combines much more readily with HB than O2 (~240 x) In other words the partial pressure of CO can be quite low and it will still bind preferentially with Hb
– COHb shifts O2-Hb curve to Left, which interferes with O2 off-loading
– So, you can have normal [Hb] and Po2, but very little O2 available to tissues

© 2007 McGraw-Hill Higher Education. All rights reserved.
Carbon Dioxide• Tissues also producing ~ 3.5 L/min of Co2
• So, ~ 140 ml Co2/L of blood (maybe more, why?) must be off-loaded at lung and exhaled
• CO2 carried in 3 major forms– Dissolved
• 20 times more soluble in blood than O2; ~10 % of Co2 carried
– Bicarbonate• Co2 + H2O ↔ H2CO3 ↔ H+ + HCO-
3
– HCO3- goes out, Cl- comes in
(Chloride shift)– Some H+ are bound to Hb (Haldane
effect; deoxygenated blood can carry more Co2); ~60%
– Carbamino compounds• Bound to terminal amine of blood
proteins (primarily Hb): ~ 30%
CA
© 2007 McGraw-Hill Higher Education. All rights reserved.
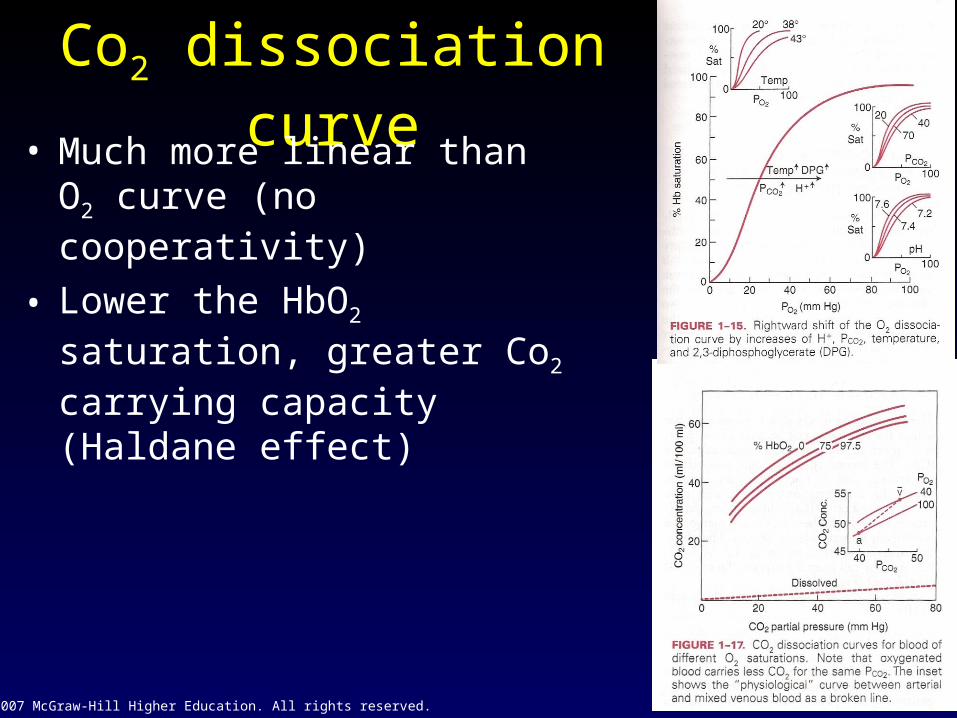
Co2 dissociation curve• Much more linear than O2 curve
(no cooperativity)
• Lower the HbO2 saturation, greater Co2 carrying capacity (Haldane effect)

© 2007 McGraw-Hill Higher Education. All rights reserved.
Blood-tissue gas exchange• O2 and Co2 move between tissues
by simple diffusion– Systemic capillaries and muscle– Pulm caps and alveoli
© 2007 McGraw-Hill Higher Education. All rights reserved.
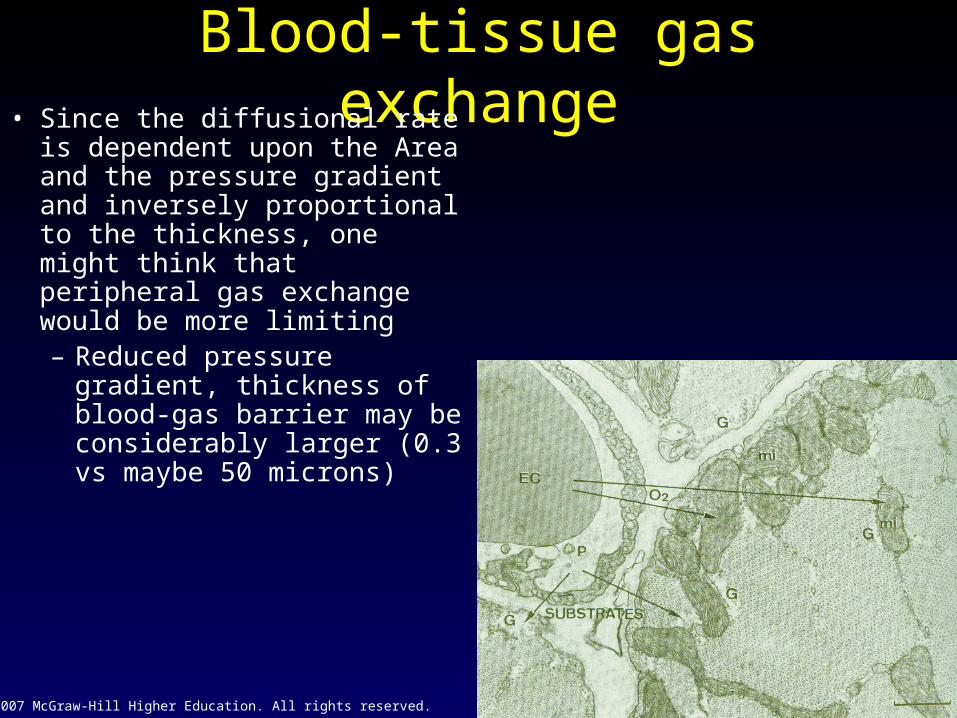
Blood-tissue gas exchange• Since the diffusional rate is
dependent upon the Area and the pressure gradient and inversely proportional to the thickness, one might think that peripheral gas exchange would be more limiting– Reduced pressure
gradient, thickness of blood-gas barrier may be considerably larger (0.3 vs maybe 50 microns)
© 2007 McGraw-Hill Higher Education. All rights reserved.
Sol
MG
WG
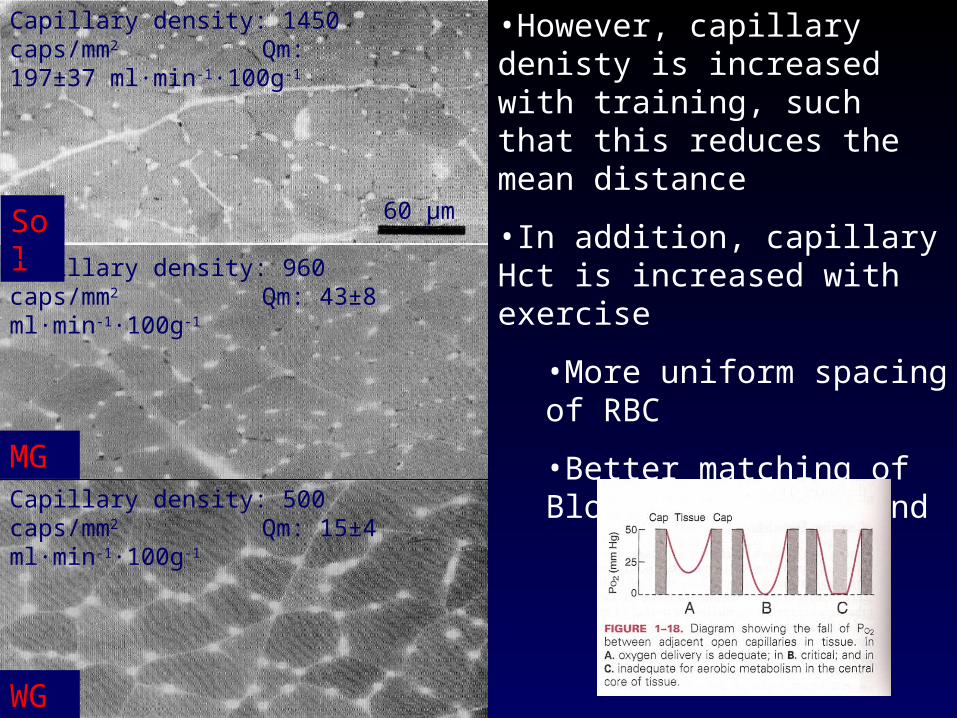
Capillary density: 1450 caps/mm2 Qm: 197±37 ml·min-1·100g-1
Capillary density: 960 caps/mm2 Qm: 43±8 ml·min-1·100g-1
Capillary density: 500 caps/mm2 Qm: 15±4 ml·min-1·100g-1
60 μm
•However, capillary denisty is increased with training, such that this reduces the mean distance
•In addition, capillary Hct is increased with exercise
•More uniform spacing of RBC
•Better matching of Blood flow to demand
© 2007 McGraw-Hill Higher Education. All rights reserved.
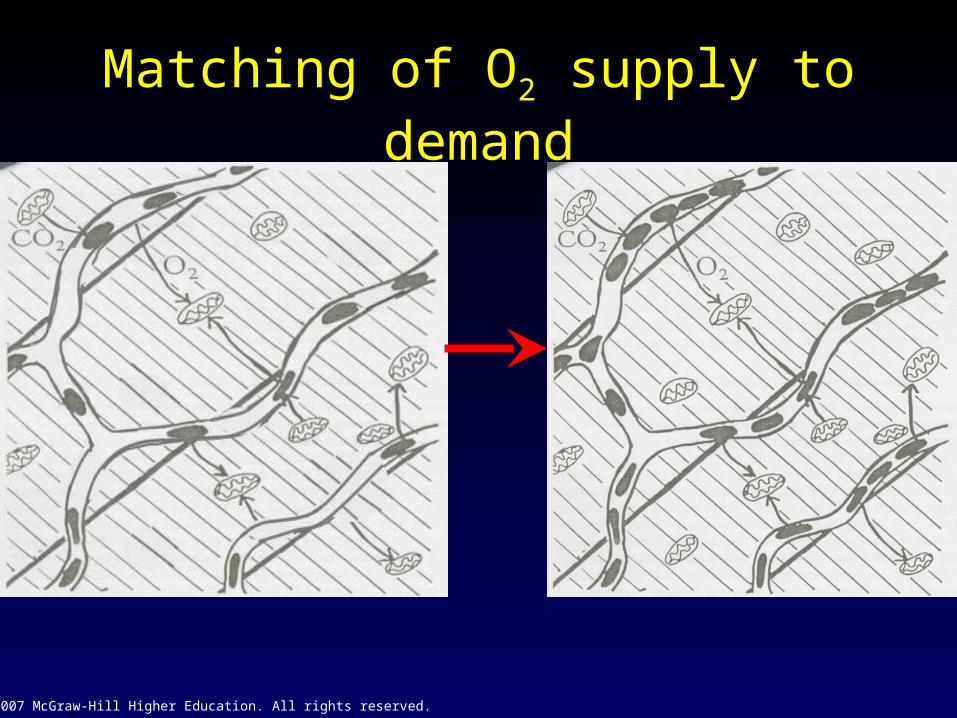
Matching of O2 supply to demand
© 2007 McGraw-Hill Higher Education. All rights reserved.
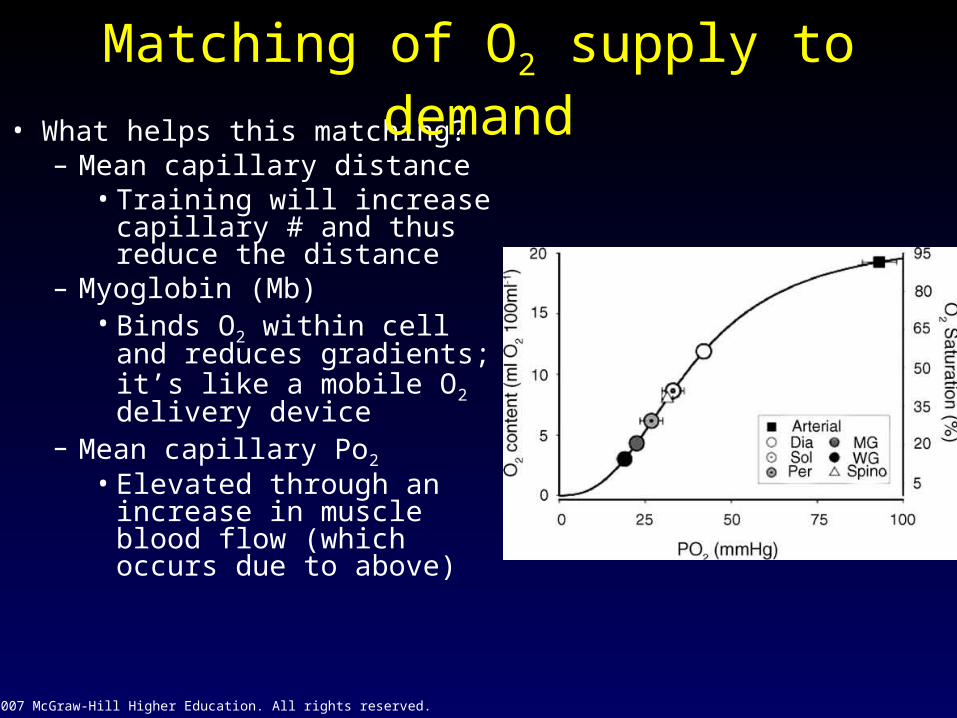
• What helps this matching?– Mean capillary distance
• Training will increase capillary # and thus reduce the distance
– Myoglobin (Mb)• Binds O2 within cell and
reduces gradients; it’s like a mobile O2 delivery device
– Mean capillary Po2
• Elevated through an increase in muscle blood flow (which occurs due to above)
Matching of O2 supply to demand