Opioid pharmacology - A comprehensive subject seminar on Opioids
date post
22-Dec-2015Category
view
217download
2
© 2005 Rehabilitation Institute of Chicago
Opioid Pharmacology and Management Principles
Part I
Steven Stanos, DO

© 2005 Rehabilitation Institute of Chicago

© 2005 Rehabilitation Institute of Chicago
“Opiate”
“Opioid”
“Narcotic”

© 2005 Rehabilitation Institute of Chicago

© 2005 Rehabilitation Institute of Chicago
Can We Catch the Pendulum?
Avoidance
Will not prescribe opioids for any reason
Driven by fear of regulatory action or antiquated views of addiction exaggerating the perception of risk
Balance
Rational pharmacology; application of principles of addiction medicine
Tailor therapy to risk in individual patients
Widespread Use
Prescribing without recognition of dangers
The pendulum rarely stops in the middle
Adapted from Rich A. APS Bulletin. 2005.

© 2005 Rehabilitation Institute of Chicago
Holy Grail ?
• Potent analgesic
• More less potent agents
• Drugs for reduced renal function
• Better formulations
• Less divertible

© 2005 Rehabilitation Institute of Chicago
Products Commonly Prescribed in the US
IMS NPA+, 2006.Number of Prescriptions (in Millions)
0 20 40 60 80 100 120
Tramadol/Combo
Propoxyphene/Combo
Codeine/Combo
Hydrocodone/Combo
Oxycodone/Combo
Oxycodone
Morphine
Hydromorphone
Fentanyl
Atorvastatin
Amoxicillin
Highly PrescribedProducts in US

© 2005 Rehabilitation Institute of Chicago
Current Treatment Armamentarium
4-6 Hour
12 Hour
24 Hour
Do
sin
g In
terv
al
HYM, Morphine,OXYM, PROP,
Tramadol
Non-opioids Combination Opioids Single-Agent Opioids
Class of Therapeutic Agent
Unmet Needs
OXCD CR,Morphine CR,
OXYM ER
Tramadol ERMorphine CR
APAP, Aspirin
Naproxen
Celecoxib
COD/APAP,HC/APAP,
OXCD/APAP,TRAM/APAP

© 2005 Rehabilitation Institute of Chicago
Opioids—the Science
Mechanisms1
• Biogenesis of endogenous peptides
• Anatomic distribution• Endocrine changes• Endogenous opioids and
stress2
• Receptor characteristics
1. Bailey CP, et al. Curr Opin Pharmacol. 2005;5:60–68 [Evidence Level C] 2. Bruehl S, et al. Clin J Pain. 2004;20:283–292. [Evidence Level A]

© 2005 Rehabilitation Institute of Chicago
Genetic Polymorphisms and Response to Opioids
• Subtype variants of mu opioid receptor1,2
– Alter binding affinities
– Change in receptor densities3
• Interindividual variability in pain perception and sensitivity to analgesics1,2
– Efficacy– Side effects– Tolerance profiles– Risk of drug abuse
1. Landau R. Anesthesiology. 2006;105;235–237 [Evidence Level C]; 2. Pasternak GW. J Pain Symptom Manage. 2005;29(suppl):S2–S9 [Evidence Level C]; 3. Ross JR, et al. Pharmacogenomics J. 2005;5:324–336. [Evidence Level B]

© 2004 Rehabilitation Institute of Chicago
Le
vel o
f A
cti
vati
on
MOR-1 Variant 1
Drug 1
Drug 2
Receptor
Mu-opioid Receptor Activation and Incomplete Cross Tolerance
Adapted from Pasternak GW. Trends Pharmacol Sci. 2001;22:67-70.
MOR-1 Variant 2
MOR-1 Variant 3
MOR-1 Variant 4
MOR-1 Variant 5
Receptor Variation for Same Patient with Different Drug
55

© 2005 Rehabilitation Institute of Chicago
OpioidsI. Syntheric phenylpiperidines
Meperidine, Fentanyl,
II. Synthetic PseudopiperidinesMethadone, Propoxyphene
III. Naturally Occurring AlkaloidsA. Natural: Heroin, Morphine, CodeineB. Semi-synthetic: Hydromorphone, Oxycodone,
OxymorphoneC. Tramadol

© 2005 Rehabilitation Institute of Chicago
Opioid EffectsGeneral• Analgesia• Altered mood• Decreased anxiety• Respiratory depression• Inhibition central reflexes• (-) GI motility• Cough suppression• (-) CRF, ACH• Miosis• Pruritus, nausea, vomiting
Reinforcing effects• Reduce anxiety• Decrease boredom• Decrease aggression• Increase self-esteem
Epstein S. In: Clinical Manual Addiction Psychopharmacology, 2005.

© 2005 Rehabilitation Institute of Chicago
Characteristics of Immediate- and Extended-Release Opioids
Immediate-release opioids• Quick onset of action (within
minutes)
• Potential use for some types of acute pain and some types of BTP
• Can be used for dose finding during initial treatment
• Inconvenient repetitive dosing
• Peak and trough phenomenon
– Not ideal for chronic pain
– May increase frequency of end-of- dose (trough) breakthrough pain
– Increased potential for euphoria and adverse effects (peaks)
Extended-release opioids
• More stable blood levels
• Potential benefit for persistent acute pain and chronic pain because avoids peaks and troughs
• May reduce frequency of end-of-dose BTP
• Potential for lower incidence of side effects (fewer peaks)
• May decrease pain-related sleep interference
• Potential improvement in compliance and quality of life
McCarberg BH, Barkin Rl. Amer J Ther. 2001;8:181-186.

© 2005 Rehabilitation Institute of Chicago
Around-the-Clock (ATC) Medication - Treating Persistent Pain*
Therapeutic Window
ATC Medication
Pain ReliefThreshold
Over Medication
*Baseline or persistent pain is controlled by ATC medication.
Persistent PainPersistent Pain
TimeTime

© 2005 Rehabilitation Institute of Chicago
Treating Cancer Pain – Inadequate Management of Breakthrough Pain
Traditional BTP Medications*ATC Medication
Over Medication
*Delayed onset of action, type and dose may not adequately treat a BTP episode.
Persistent PainPersistent Pain
TimeTime

© 2005 Rehabilitation Institute of Chicago
Treating Cancer Pain – Ideal Management
Ideal Breakthrough Pain Medication* ATC
Medication
Over Medication
*Breakthrough pain treatment has rapid onset and matches the intensity and duration of BTP episode.
Persistent PainPersistent Pain
TimeTime

© 2005 Rehabilitation Institute of Chicago
Opioid Pharmacokinetics
Opioid Half LifeBioavail-ability(%) Active Metabolites
Morphine 2–4 10%–50% Codeine, M6G, M3G
Pethidine, Meperidine
3–4 30–60 Norpethidine, Normeperidine
Methadone 6–150 60–90 None
Fentanyl 3–7 <2 None
Hydrocodone 4–4.5 Hydromorphone, Norcodeine
Codeine 3–4 60–90 Morphine, Hydrocodeine
Oxycodone 2–6 40–130 Oxymorphone
Hydromorphone
2–4 35–80 None

© 2005 Rehabilitation Institute of Chicago
Propoxyphene (Darvocet)
• With acetaminophen (Darvocet-N100)
• Structurally related to methadone
• Peak plasma concentration 2 h
• Liver metabolism to norproxyphene

© 2005 Rehabilitation Institute of Chicago
FDA ruling on Propoxyphene
• UK: phased removal in 2005• Pubic Citizen petitioned for removal• ASHSP recommends FDA withdrawal (Jan ‘09)• No more effective than APAP alone, similar to tramadol• Supported by Beers Criteria as inappropriate for the
elderly• FDA Advisory Committee (Jan.’09):14-12 in support of
removing from market• July 7, 2009: FDA: black box warning, remain on market

© 2005 Rehabilitation Institute of Chicago
Hydrophilic• Slower entry into
CNS• Active metabolites
(M3G, M6G)
Morphine-3-glucuronide
• inactive?, CNS excitation
Morphine-6-glucuroide• Active analgesic, 2-100x
more potent (centrally), Induces liver enzymes
Morphine (Gold Standard)
MS IR®: 15, 30 mg
MS Contin®: 15, 30, 60, 100, 200 mg
Kadian®: 20, 30, 50, 60 mg
Avinza®: 30, 60, 90, 120 mg

© 2005 Rehabilitation Institute of Chicago
Modified Release OpioidsProduct Dosage Form Strength (mg) Dosing
frequency (h)
Morphine sulfate
Avinza ER capsules 30 ,60,90,120 24
Kadian SR capsules 20,30,50,60,100 12-24
Oramorph SR tablets 15,30,60,100 8-12
MS Contin CR tablets 15,30,60,100,200 8-12
Oxycodone HCL CR tablets
Oxycontin CR tablets 10,20,40,80,160 12
Oxymorphone HCL
Opana ER tablet 15,10,20,40 12
Amabile C, Bowman B. Ann Pharmacother 2006;40.

© 2005 Rehabilitation Institute of Chicago
Combination Opioids
Agent OnsetDuration of
ActionEquianalgesic
Oral Dose*
DEA Sched
Oxycodone Combos
10-15 min
4-6 hrs 30 mg† II
Hydrocodone Combos
30-60 min
4-6 hrs 30 mg III
Codeine Combos
30-60 min
4-6 hrs 130 mg III
Propoxyphene Combos
15-60 min
4-6 hrs 130 mg IV
Tramadol Combos
60 min 6-7 hrs 100 mgNot
sched
Gutstein HB, Akil H. Opioid analgesics. In: Hardman JG, et al. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 10th ed. New York: McGraw Hill; 2001:569-619.
www.musc.edu/pharmacyservices/medusepol/opiodanalgesicfinal.pdf.
Mild
to
Mo
der
ate
Mo
der
ate
to S
ever
e
Pai
n In
tens
ity
*Doses reflect opioid component only and are equianalgesic to 30 mg morphine†Doses for moderate to severe pain not necessarily equivalent to 30 mg morphine‡NA, not applicable

© 2005 Rehabilitation Institute of Chicago
– Prodrug (nonactive in form delivered)– Dependent on P450 2D6 enzyme system– Concurrent medication therapy may affect
prodrug metabolism if drug(s) inhibit P450 2D6– Tylenol combination: Norco, Lortab, Percocet,
Roxicet
Hydrocodone/ Oxycodone

© 2005 Rehabilitation Institute of Chicago

© 2005 Rehabilitation Institute of Chicago
Acetaminophen (Tylenol)

© 2005 Rehabilitation Institute of Chicago
FDA Decisions: June 30,2009
• 20-17: ban combination products
• 21-16: lower maximum daily APAP
• 24-13: limit maximum single dose APAP
• 26-11: 1,000 mg dose APAP prescription
• Final decision pending

© 2005 Rehabilitation Institute of Chicago
Acetaminophen (APAP)• A centrally acting analgesic that increases the pain threshold
• Mechanism of action is not fully known– May selectively inhibit a distinct form of COX (COX-3)– Most likely has no affinity for the active site of COX, but blocks activity by
reducing the active oxidized form of COX to an inactive form
• Indicated to reduce fever and for the temporary relief of minor aches and pains
• Fewer GI side effects than NSAIDs/COX-2 inhibitors
• Adverse effects associated with chronic use
Roberts LJ II, et al. In: Hardman JG, et al, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 2001:703-705.Lucas R, et al. FASEB J. 2005;19:635-637.

© 2005 Rehabilitation Institute of Chicago
Breakthrough Pain Medications
Immediate-Release Opioid
Onset of analgesia
(min)Duration of effect
(h)
Morphine 30–40 4
Oxycodone 30 4
Hydromorphone (oral) 30 4
Methadone 10–15 4–6
Fentanyl (transmucosal)
Oxymorphone
5–10
30
1–2
6-9
Bennett D, et al. Pharmacol Ther. 2005;30:296–301. [Evidence Level C]

© 2005 Rehabilitation Institute of Chicago
New Short-Acting Opioids for Breakthrough Pain (BTP)
• Transmucosal fentanyl (Actiq®)
• Fentanyl buccal tablet (Fentora™)
• Oxymorphone (Opana®)
• Tapentadol (Nucynta®)

© 2005 Rehabilitation Institute of Chicago
Oral Transmucosal Fentanyl Citrate (OTFC)
• First rapid-onset formulation • 50% bioavailability• Median onset of relief: 15 min• Peak plasma concentration
± 22 min• Approved for cancer
breakthrough pain
Lichtor JL, et al. Anesth Analg. 1999;89:732–738 [Evidence Level A]; Streisand JB, et al. Anesthesiology. 1991;75:223–229 [Evidence Level B]; Portenoy RK, et al. Pain. 1999;79:303-312 [Evidence Level A]; Payne R, et al. J Pain Symptom Manage. 2001;22:575-583. [Evidence Level B]

© 2005 Rehabilitation Institute of Chicago
Fentanyl Buccal Tablet (FBT)*
• OraVescent® drug delivery technology generates a reaction that releases carbon dioxide when the tablet comes in contact with saliva1,2
– Transient pH changes optimize dissolution (at a lower pH) and membrane permeation (at a higher pH)
1. Pather SI, et al. Drug Delivery Tech. 2001;1:54–57 [Evidence Level B]; 2. Durfee S, et al. Am J Drug Delivery. 2006;4:1–5. [Evidence Level B]

© 2005 Rehabilitation Institute of Chicago
Multiple Pathways of Pain Transmission: Neuronal Integration of Signaling1-3
Painful stimulus
Ascending
Descending
1. Terlinden R et al. Eur J Drug Metab Pharmacokin. 2007;32(3):163-169. 2. Vanderah TW. Med Clin North Am. 2007;91(1):1-12. 3. Tzschentke TM et al. J Pharmacol Exp Ther. 2007;323(1):265-276.
Ascending pathwayto the brain
Descending pathwayfrom the brain
Primary afferentSecondary afferent

© 2005 Rehabilitation Institute of Chicago
Drug Mechanism of Action (in vivo): Dual μ-Opioid Receptor Agonist and Norepinephrine
Reuptake Inhibitor1,2
Pain signal
Glut+
SP
Ascending pathwayto the brain
Descending pathwayfrom the brain
NE
2-AR
–
μ-OR
Tapentadol*
+
The yellow cylinder with the purple NE ball represents the NE reuptake transporter protein. NE = norepinephrine; 2-AR = alpha2-adrenoceptor; -OR = μ-opioid receptor; SP = substance P; Glut = glutamate.1. Tzschentke TM et al. J Pharmacol Exp Ther. 2007;323(1):265-276. 2. American Pain Society. http://www.npcnow.org/resources/PDFs/painmonograph.pdf. December 2001. Accessed March 7, 2008.
*The exact mechanism of NUCYNTA™ is unknown.
-
Secondary afferentPrimary afferent
-

© 2005 Rehabilitation Institute of Chicago
Tapentadol and Tramadol: Different Molecular Structures
OH
·HClN
(R)(R)
Tapentadol Tramadol
OH
OCH3
HOH ·HCl
N

© 2005 Rehabilitation Institute of Chicago
Tapentadol and Tramadol:Prescribing Information Differences
Feature Tapentadol Tramadol
Pain severity Moderate to severe Moderate to moderately severe
Mechanism of action
•Binds to μ-receptors•Inhibits reuptake of norepinephrine
• Binds to μ-receptors• Inhibits reuptake of norepinephrine• Inhibits reuptake of serotonin
Activity of metabolites
Metabolites are not active
M1 metabolite with 6- and 200-foldgreater potency than parent drug for analgesia and μ-OR affinity, respectively
Metabolism Primarily Phase 2 conjugation to glucuronide and sulfate
O-demethylation produces M1 (CYP2D6); N-demethylation (CYP3A4 and CYP2B6); sulfation/glucuronidation
Federal scheduling
Schedule II Unscheduled
OR = opioid receptor.

© 2005 Rehabilitation Institute of Chicago
Tapentadol: Indication and Dosing• Tapentadol is indicated for the relief of
moderate to severe acute pain in patients 18 years of age or older
• The dose is 50 mg, 75 mg, or 100 mg every 4 to 6 hours depending upon pain intensity– Good clinical practice dictates that the lowest starting dose
be used and, as always, the dose should be individualized for the patient
– 50 mg is the lowest dose available – Daily doses on first day of therapy above 700 mg and on
subsequent days above 600 mg have not been studied in controlled clinical trials and are not recommended
• Clinical considerations should include:– Patient's medical history and concomitant medication use– Previous experience prescribing similar drugs– Severity of the pain being treated– Ability to monitor the patient

© 2005 Rehabilitation Institute of Chicago
Tapentadol: Clinical Pharmacokinetics
• Bioavailability is 32% after single-dose administration in fasted state
• Low plasma protein binding (~20%)• 97% metabolized
– Occurs mainly via Phase 2 pathways (55% O-glucuronide, 15% sulfate of tapentadol)
– Other metabolism (15%) via P450 enzymes (13% by CYP2C9 and CYP2C19, 2% by CYP2D6)
• 99% of tapentadol and its metabolites eliminated via renal clearance • Metabolites lack analgesic activity
• Time to maximum serum concentration (Tmax): 1.25 h
• Half-life (t1/2): 4 h

© 2005 Rehabilitation Institute of Chicago
Mea
n C
um
ula
tive
SP
ID S
core
1
The
hig
her
the
SP
ID s
core
,th
e gr
eate
r th
e pa
in r
elie
f
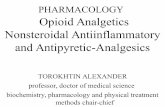
Osteoarthritis Hip/Knee Study: Efficacy Results
Placebo
Oxycodone IR 10 mg
Tapentadol IR 75 mg
Tapentadol IR 50 mg
N=659
130.6
229.2236.5
*
0
50
150
250
SPID-5 Days (Primary Endpoint)
100
200
223.8
SPID = sum of pain intensity differences, where a higher score indicates greater pain relief. *P<.001 for all comparisons vs placebo.1,2 † Both doses of tapentadol were noninferior to oxycodone IR 10 mg (prespecified analysis).
1. Data on file. 2. Hartrick C et al. Clin Ther. 2009;31(2):260-271.
* † * †

© 2005 Rehabilitation Institute of Chicago
Osteoarthritis Hip/Knee Study: Composite Incidence of Nausea and Vomiting1,2
IR = immediate release; GI = gastrointestinal. *Nominal P<.001 for both doses of tapentadol IR vs oxycodone IR 10 mg.
1. Hartrick C et al. Clin Ther. 2009;31(2):260-271. 2. Data on file.
N=666
8.3%
21.7%
57.0%
29.8%
0
30
50
Composite of Nausea and Vomiting
60
Placebo
Oxycodone IR 10 mg
Tapentadol IR 75 mg
Tapentadol IR 50 mg
20
40
10
Inci
den
ce (
%)
*
*

© 2005 Rehabilitation Institute of Chicago
New Long-Acting Opioids
• Tramadol ER (Ultram® ER) oral tablet– Q24h ER technology1
• Oxymorphone ER (Opana ER®) oral tablet2–4
– Q12h ER technology • Hydrophilic gel matrix with slowly eroding core
• Tramadol HCL ER (Ryzolt®)1. Gana TJ, et al. Curr Med Res Opin. 2006;22:1391–1401 [Evidence Level A]; 2. Prommer E. Support Care Cancer. 2006;14:109–115 [Evidence Level C]; 3. Durfee S. Am J Drug Deliv. 2006;4:1–5 [Evidence Level B]; 4. McIIwain H, et al. Am J Ther. 2005;12:106–112. [Evidence Level B]

© 2005 Rehabilitation Institute of Chicago
Once-Daily ULTRAM ER
ULTRAM® ER (tramadol HCl) Extended-Release Tablets Prescribing information.
Mean steady-state tramadol plasma concentrations on day 8 post-dose after administration of ULTRAM ER once-daily and tramadol every 6 hours
ULTRAM ER 200 mg qd
Tramadol 50 mg q6h
0 4 8 12 16 20 240
50
100
150
200
250
300
350
Time (h)
Tra
ma
do
l co
nc
en
trat
ion
(n
g/m
L)
2 6 10 14 18 22

© 2005 Rehabilitation Institute of Chicago
Tramadol HCL ER (Ryzolt)100mg, 200mg, 300mg

OPANAOPANA®® Tablets. Full Prescribing Information. Chadds Ford, PA. Endo Pharmaceuticals. 2006. Tablets. Full Prescribing Information. Chadds Ford, PA. Endo Pharmaceuticals. 2006.
Morphine Sulfate Extended-Release Tablets. Full Prescribing Information. Chadds Ford, PA. Endo Pharmaceuticals. 2004. Morphine Sulfate Extended-Release Tablets. Full Prescribing Information. Chadds Ford, PA. Endo Pharmaceuticals. 2004.
OxymorphoneOxymorphone
HOHOOO
N – CHN – CH33
HOHO
SOSO44
MorphineMorphine
OO
HClHCl
N – CHN – CH33
HOHO
OHOH
OO
Molecular Structures of Morphineand Oxymorphone

© 2005 Rehabilitation Institute of Chicago
Methadone (Dolophine)
• Synthetic, μ agonists, NMDA antagonist
• L/D enantiomers (50:50)• Oral bioavailability varies
(40%–99%)• Biphasic plasma level
decline• No active metabolites• Metabolized by liver (CYP
3A4)
L/D = light/darkness ratio; NMDA = N-methyl-D-aspartate.

© 2005 Rehabilitation Institute of Chicago
Methadone Dosing: Gradual ConversionMor-E (mg/d)
Calculate Meth (mg/d)
Initial Meth Dose Increment Example
<200 15 mg 5 mg q8h 5–7 d Mor 90 mg/d
Meth 5 mg q8h
200–500 ~7% Morph dose
Calculated dose given q8h
5–7 d 300 mg Mor = 21 mg/d Met
7.5 mg q8h
>500 ~7% Morph dose
1/3 calculated dose q8h
Add 1/3 dose q5d; ↓ previous opioid q5d
Complete conversion in 15 d
Goodman F, et al. Methadone Dosing Recommendations for Treatment of Chronic Pain. Available at: http://www.pbm.va.gov/monitoring/Methadone%20Dosing%20Final%20(Rev%20081103).pdf. Accessed November 28, 2006. [Evidence Level C]

Methadone: prolonged QT and Torsade de Pointes (TdP)
Risk Factors: heart disease, hypokalemia, hypomagnesemia, concomitant CYP3A4 inhibitors
MedWatch System (N= 5503)
— <1% with TdP or PQ prolongation
— Average dose 410 -/+ 349/day
— 30% within recommended range (60-100mg/day)
— 75% with risk factors
Pearson E. Pharmacoepidem Drug Saf 2005:14:747-53.

“Adverse EffectsCases
Risk Stratification
American Greetings.

Formulation Strategies Intended to Reduce Abuse
1. Gershell L et al. Nat Rev Drug Discov. 2006;5(11):889-890. 2. Katz NP et al. Clin J Pain. 2007;23(8):648-660.
Pharmacologic Approach1,2
Examples include• Addition of antagonist• Prodrug formulation
Physical Approach1,2
Examples include• Advanced dispensing formulations• Tamper-resistant formulations
Aversive Approach1,2
Examples include• Addition of non-treatment-related
ingredients such as niacin or capsaicin

EMBEDA™
2. If EMBEDA™ is crushed, chewed or extracted:
A. the naltrexone (opioid antagonist) releases and mixes with morphine
B. the morphine-naltrexone mixture is intended to prevent euphoria from morphine by competing for the same opioid receptor in the brain…thus deterring abuse of the product
1. If taken as directed, EMBEDA™ is intended to provide effective pain relief with long-acting morphine pellets; the naltrexone passes out of the body without effect
How Does the EMBEDA™ Pharmacologic Abuse-deterrent Technology Work?
Naltrexone Core Releases and Mixes
Chewing or Crushing Force
NALTREXONE CORE
MORPHINE SULFATEALO
-01
Opioid Receptor
Naltrexone Morphine

Aversion® Technology
Common Methods of Abuse Aversion Technology
InjectionExtract active ingredients from dissolved tablets or capsules
Gel-Forming Agenta
(polyethylene oxide)makes it difficult to extract active ingredient
Snorting Crushed tablets or capsules
Tissue Irritant (sodium lauryl sulfate)
Oral Ingestion Excessive Quantities
Niacincauses temporary unpleasant effects with ingestion of higher than recommended doses
1. Data on file. King Pharmaceuticals®, Inc.
a Two additional excipients synergize polyethylene oxide

Adverse Effects: Nausea and Vomiting
Chemoreceptor trigger zone (CTZ)
Cortex
Peripheral pathways
Vestibular sensitivity

Copyright restrictions may apply.Wood, G. J. et al. JAMA 2007;298:1196-1207.
Neural Pathways That Mediate Nausea and Vomiting

Common Clinical Scenarios of Nausea/ Vomiting (N/V)
Clinical Mechanisms First-line
Opioid Induced Stim CTZ (D2)
Gastroparesis (D2)
Constipation (H1, Muscarinic)
Sensitization Ear (H1, Muscarinic)
Metoclopramide
Prochlorperazine
Impaired Motility Gastroparesis (D2) Metoclopramide
Radiation Associated
N / V
Stimulation peripheral pathways via 5HT3
5HT3 Antagonists
Motion Associated Stimulation via vestibulocohclear nerve (Muscarinic acetylcholine )
Scopolamine
Diphenhydramine
Promethazine
Wood, G. J. et al. JAMA 2007;298:1196-1207.

Nausea:Treatment
Antihistamines (H1)
— Diphenhydramin (Benadryl): 25-50mg PO
— Scopolamine: 1.5mg TD patch Q 72hrs
Antipsychotics (D2/CTZ)
— Haloperidol (Haldol): 0.5 – 4mg PO
— Prochlorperazine (Compazine): 5-10mg PO; 25mg PR
— Promethazine (H1) (Phenergan): 12.5-25mg PO; 25mg PR
Prokinetic agents (D2)
— Metoclopramide (Reglan): 5-20mg PO/IV
Serotonin Antagonist (5HT3)
— Ondansetron (Zofran): 4-8mg PO or IVSwegle JM, Logeman CL. Amer Fam Phys 2006;74:1347-54

Opoid Induced Sedation
Methylphenidate1,2 (Sch II): 5-10 mg TID PRN
Dextroamphetamine (Sch II): 2.5 – 7.5mg BID, PRN
Caffeine
Donepezil (Aricept)3,4: 2.5 – 10mg/day
Modafinil (Provigil) (Sch IV): 100 – 600 mg/ day
Differential Diagnosis5: depression, hypothyroidism, opioid dose, opioid adverse effect, endocrine, sleep disorder 1. Bruera E, et al. J Pain Symptom Manage 1989;4:3-6.
2. Bruera e, et al. Pain 1992;50:75-7.3. Slatkin et al. J Pain Symptom Manage 2001;21:425-38.4. Bruera E, et al. J Pain Symptom Manage 2003;26:1049-54.5. Reissig JE, Rybarczyk A. Ann Pharmacother 2005;39:727-31.

Modafinil (Provigil): animal studies
• PROVIGIL promoted wakefulness without widespread CNS stimulation• PROVIGIL is thought to work selectively in areas of the brain believed
to regulate normal wakefulness
H = hypothalamusCA = caudate
PROVIGIL MethylphenidateAmphetamine
Lin JS, et al. Proc Natl Acad Sci USA. 1996;93:14128 14133.

Modafinil (Provigil)
Mechanisms: decrease GABA release in cortex, weak dopamine release, amygdala?
Scheduled IV: 100 mg, 200mg
FDA: narcolepsy, shift work sleep disorder
Webster L et al, Pain Medicine 2003;4:135-40
— Retrospective, N = 11, Epworth Sleepiness Scale (ESS)
— Dose range: 264 mg – 427mg/ day
— Opioid dose: 536 mg – 810 mg/ day

Opioid Induced Hypogonadism
Dopamine
Prolactin
Testosterone Estradiol, Progesterone
INHIBITED
Pulsitile GnRH
LH
FSH
Christo PJ. Anesthes Clin N Am. 2003;21:699-713.

Hypogonadism: (OPIAD)
Sexual dysfunction, infertility
Depression
Decreased energy level
Muscle wasting and osteoporosis
Lowered pain threshold
Impaired wound healing
“Opioid Induced Androgen Deficiency” (OPIAD)
Lab
Free testosterone (FT)
Total testosterone (TT)
Luetinizing hormone (LH)
Follicle-stimulating (FSH)
Estradiol (E2)
Prostate specific antigen (PSA)

Testosterone Patch in Men with OPIAD
24 week, open label pilot, N =23
Results:
(BL): subnormal FT, low normal LH
(Tx): elevated FT, TT, DHT, E2
Danniell H, et al. J Pain 2006;7:200-210.

Opioid Induced Sensorineural Hearing Loss
Hydrocodone/ APAP abuse1
15-60 tablets/ day
cochlear toxicity
• Hydrocodone/APAP2
50-300mg/ day
association with Hep C
Severe impairment
Propoxyphene abuse3
1.Oh AK. et al. Neurology 2000;54:2345.
2. Ho et al. Pain Physician 2007;10:467-72.
3. Harell M. et al. Laryngoscope 1978;88:1518-21.

Waldhoer M, et al. Annu Rev Biochem. 2004;73:953-990.
Opioid Receptor Structure
INHIBITORY
ECITATORY
Gi / Go
Gs

© 2005 Rehabilitation Institute of Chicago
Opioid-Induced Abnormal Pain Sensitivity
• Desensitization process leading to opioid tolerance
• Sensitization (pronociceptive) process leading to opioid-induced pain sensitivity
Increased spinal dynorphinIncreased spinal dynorphinDescending facilitationDescending facilitationGlutamatergic systemGlutamatergic system

© 2005 Rehabilitation Institute of Chicago
OPIOID
PRONOCICEPTIVE
DESENSITIZATION (TOLERANCE)
SENSITIZATION(INCREASED PAIN?)

© 2005 Rehabilitation Institute of Chicago
Opioid Induced Hyperalgesia (OIH)
• Mao, J (2002)• Post-Surgical Studies: Increased pain and
analgesic use (Guignard B, 2006)• Problems: opioid naïve patients, post-surgical,
methadone maintenance• (Cohen S, et al 2008)
– 355 patients, interventional procedures– Results: enhanced pain perception in opioid patients
with local lidocaine prep– Correlated with dose and duration of Tx

© 2005 Rehabilitation Institute of Chicago
“Men in general are quick to believe that with which they wish
to be true.”
- Julius Caesar

© 2005 Rehabilitation Institute of Chicago
TOLERANCE
and
DEPENDENCE
= ADDICTIONX

© 2005 Rehabilitation Institute of Chicago
Volkow ND. In: Madras et al. eds. Cell Biology of Addiction, 2006.

© 2005 Rehabilitation Institute of Chicago
Inadequate Pain ManagementInadequate Pain Management
ANGERANGER FRUSTRATIONFRUSTRATION
ISOLATIONISOLATION AVOIDANCEAVOIDANCE
CRISISCRISIS
PATIENTPATIENT TEAMTEAM
Weissman,Haddox, Pain (1989)Weissman,Haddox, Pain (1989)
“Pseudoaddiction”

© 2005 Rehabilitation Institute of Chicago
Predicting aberrant behaviors
• High risk– Family history of substance abuse– Legal problems– Drug or alcohol abuse
• Other – Cigarette use, higher opioid dose, less opioid
reported side effects, MVA– Mental health disorders
Michna E, et al. J Pain Sym Management 2004;28:250-8.

© 2005 Rehabilitation Institute of Chicago
Aberrant Drug-Related Behavior: Implications
• Differential diagnosis of aberrant drug-related behavior
– Addiction
– Pseudoaddiction
– Other psychiatric disorders
• Axis I and Axis II disorders• Mild encephalopathy • Family disturbances
– Criminal intent: diversion
Portenoy RK, et al. In Lowinson JH, et al.(eds): Comprehensive Textbook of Substance Abuse, Fourth Edition. Baltimore: Williams and Wilkins, 2005, pp. 863-903.

© 2005 Rehabilitation Institute of Chicago
Predicting opioid misuse at 1 year
Misuse (32%)• Predictors
cocaine abuseDUI convictionmalecannabinoids
“Opioid misuse”
• (-) tox screen• (+) for other• Multiple providers• Diversion• Forgery• Stimulant use
Ives TJ, et al. BMC Health Ser Res 2006;6:46.

© 2005 Rehabilitation Institute of Chicago
• Excessive pain intensity
• Extreme ratings of emotional distress
• Poor perception of coping effectiveness
• Use of multiple pain descriptions
• Poor perceived social support
• Multiple pain sites
• Poor employment history
• Long-term reliance on health professionals
• Addiction risk factors
• History of failure with chronic opioid therapy or allergic sensitivity
Nedeljkovik SS, et al. Clin J Pain. 2002;18:S39-S51.Portenoy RK, et al. J Pain Symptom Manage. 1990;5:S46-S62.Federation of State Medical Boards of the United States, Inc. Model Guidelines for the Use of Controlled Substances for the Treatment of Pain. May 2004.
None of these are absolute
contraindications and lack predictive validity at this point
Patients Who May Not Benefit From Opioid Therapy

© 2005 Rehabilitation Institute of Chicago
A Chronic Pain Patient vsan Addicted Patient
Pain Patient Abuse Addicted Patient
Appropriate use Inappropriate use: inadequate dose or excessive dose
Inappropriate use
Quality of life Quality of life or Quality of life
Function Function or Function

© 2005 Rehabilitation Institute of Chicago
Total Pain Population
Aberrant Behavior: 40%
Abuse: 20%
Addiction: 2%–5%
Aberrant Behavior vs Abuse
Webster LR, Webster RM. Pain Med. 2005;6:432–442;
Webster LR, et al. Pain Med. 2005;6:432–442.

© 2005 Rehabilitation Institute of Chicago
Summary
• Remember opioid pharmacokinetics
• Side effect management important to improving chances of success
• Opioid hyperalgesia
• Endocrine effects
• Risk stratify patients